





































 medicine
medicineSimilar presentations:










Exanthema
1.
EXANTHEMA (rash) is discrete pathologicalformation of skin like answer for influence or toxins and
metabolites of causative agent.
The reaction of skin manifests by plethora of vessels
of microcirculation, increase of vascular permeability with
development of edema and hemorrhage, necrosis of
epidermis and deeper layers of skin, dystrophic changes of
cells (ballooning degeneration), serosal, purulent, serosalhemorragic inflammation.
Depending on predominance and degree of expressed
of these processes one or another type of exanthema is
formed.
The presence of rash is important for diagnostics and
in a number of cases for estimations of severity of duration
of illness and its prognosis.
2.
CLASSIFICATIONCriteria of classification of exanthemas :
type of elements of rash : roseola,
macula, erythema, papula, tubercle, nodus,
urtica, vesicula, pustula, bulla, petechia,
ecchymosis;
sizes: small − up to 2 mm in a diameter,
middle − to 5, large – more 5 mm;
form: right, wrong;
3.
homogeneity of elements of rash :− monomorphous (all elements behave to
one kind and have identical sizes);
− polymorphic (the elements of rash are
different by kind, sizes or form);
localization of elements :
symmetric,
asymmetric,
mainly in one area of skin;
4.
abundance of rash :single (till 10 elements),
unabundant (elements can be counted),
abundant (plural);
transformation of rash : appearance of element,
its development, often with the transition of
element of one kind in other and extinction of
rash;
terms of appearance (day of illness) :
early 1-2th day,
middle - 3-4th day,
late — after the 5th day.
5.
At description of rash the background of skin(pale, hyperemic) is specified.
Exanthema is important for diagnostics of infectious
diseases because it meet at many infectious diseases.
Some exanthemas are characteristic for some infectious
disease. For example, «morbilliform rash»
«scarlatiniform rash», however it can be accompanied
with other diseases, consequently, even at such
exanthemas it is necessary to make differential
diagnostics.
6.
Rashe presents at:many skin illnesses,
bites of insects,
allergic reactions on natural allergens and
on different medicinal preparations,
at the chemical irritation of skin.
7.
Frequency of exanthemas at different infectiousdiseases is different.
Among infectious diseases with exanthema it is
possible to distinguish diseases at that exanthema:
1)is obligatory component of clinical symptomatology
(measles, scarlatina, chicken-pox);
2)is facultative (at 50-70% of patients) − rubella,
spotted fever, typhoid fever;
3)meets relatively rarely (infectious mononucleosis,
leptospirosis, viral hepatitis of and other).
In this connection the diagnostic value of presence (or
absence) of exanthema at different infectious diseases
differentiates substantially.
8.
Exanthemas at infectious diseases arevery heterogeneous and differentiate:
by the nature of elements of rash,
by localizations,
by the terms of appearance,
by stage of appearance,
by the dynamics of development of
separate elements.
9.
Dermatologists and infectiologists not always simplydesignate one or another elements of exanthema. Most
infectiologists use terminology of проф. A.I. Ivanov from
1970 and now.
A roseola (roseula) is a round spot of pink, red or purple
color measuring to 2-5 mm, disappeared at pressing or
tension of skin. Thise is a local plethora of vessels of
microcirculation at papillary layer of skin.
Small (about 1 mm in a diameter) abundant roseolar rash is
designated as punctulate.
Every element some overpeers above the level of skin
stipulating the special «velvetiness» of skin in area of rash.
This element is typical for typhoid fever, spotted fever; it
can be present also at a generalized salmonellosis,
rickettsiosis, syphilis.
10.
A spot (тасиlala) is an element of rash, similar with aroseola, but more large sizes (5-20 mm), does not come
forward above the level of skin, colouring is the same a
roseola.
Also it is contingently dilation of vessels.
A form of spots can be oval, rounded or incorrect with the
scalloped edges.
At pressing or stretch of skin disappears spot, at stopping of
pressure it appears again.
Infectiologists distinguish:
small spotted rash− 5 - 10 mm in a diameter,
large spotted rash 11-20 мм in diameter.
It has a differential-diagnostic value. For example, small
spotted rash appears at rubella, large spotted rash appears at
measles.
11.
A papula (papula, nodus) is noncavitarysuperficial formation elevated above the skin. It
has soft or dense consistency and develops back
without formation of scar, can be inflammatory
and noninflammatory papulae. At infectious
diseases only inflammatory papulas appear due
to proliferation of epidermis and development of
infiltration in the papillary layer of derma with
dilation of vessels and limited edema. Colouring
of papulae is like roseolas or spots. The size of
papulae is different (1-20 mm) :
Miliary − 1-1,5 mm),
Lenticular − more large (2-3 mm),
Confluence of papulae is patchs.
12.
Papulae can be:Sharp (cone-shaped form),
flat,
semispitsical.
surface of papulae : 1) smooth or 2) covered by scales.
in future papulae can pass to other elements of rash —
vesicles, pustulas.
The sequence of transformation has an important
diagnostic value:
At appearance of other element of rash in place of
papula it is talked already not about a papula but about
new element of rash
13.
If the elements of rash are unhomogeneous andsimultaneously both papulae and spots such
mixed
rash
is
named
maculopapular,
roseolopapular rash is possible too.
Original combination of roseolas and papulae is
marked at typhoid fever. For these illnesses
roseolas slightly overpeering above the skin are
characteristic.
14.
Erythema (еritетаritетаеritетата) is vast areas of hyperemic skin ofred, purple-red or purple color. Erythema arises up as a
result of dilation of vessels of papillae of skin and
subpapillary vascular interlacement, the expressed
inflammatory process is absent.
It can appear as a result of confluence of large spots for
example at a measles, infectious erythema of Rosenberg
It has scalloped edges, separate areas of skin with the
normal colour can be present into erythematous fields.
Erythemas appear also as a result of sharp local
inflammation (for example at an erysipelas, anthrax,
traumas) with edema (inflammatory areas are raised
above the level of skin) and sickliness at palpation.
15.
Thise is not complete accordance between terms«erythema» and «erythema nodosum», when noduses are
elements of rash but not erythema.
Hyperemia of vast areas of skin is not erythema also, for
example, so-called «symptom of hood» (hyperemia of
face, neck and upper departments of trunk) that often
meets at many infectious diseases (leptospirosis,
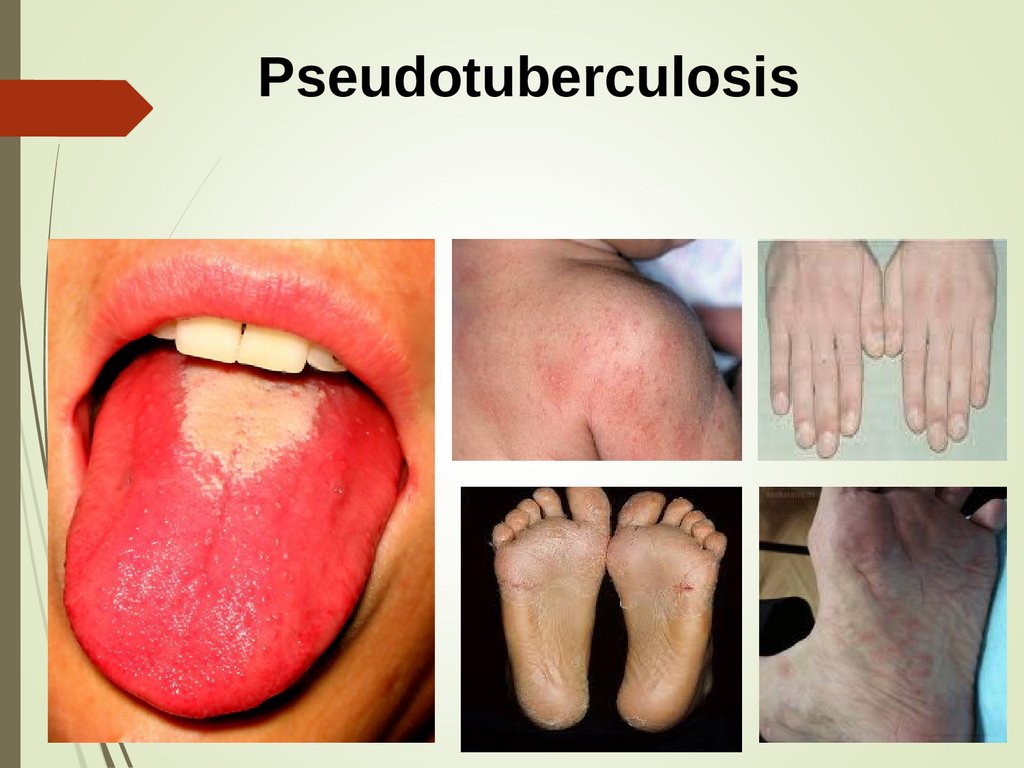
Denguenfever and other), local hyperemia of hands and
soles (symptom of «gloves» and «socks» at
pseudotuberculosis) and also general hyperemia at
scarlatina.
Unlike infectiologists dermatologists understand under a
term «erythema» inflammatory areas diameter from 2 cm
to a few ten of centimetres (active erythema), and also
cyanosys, conditioned by venous stagnation (massive
erythema).
16.
A tubercle (tuberculum) is noncavitary formationarising up because of development of inflammatory
infiltration of granulomatous structure (inflammatory
tubercles) in the derma. Similar with a papula (on sizes,
color, consistency).
It is elevated above the skin but placed deeply in a
derma.
At palpation infiltration is always determined.
Diameter from 3-5 to 20 мм.
Color is from pink-red or red-yellow-red to coppercoloured.
It have clear borders and tendency to the
groupment. Unlike papulae at furthis tubercle can
necrotize forming ulcers and scars.
17.
For finding out of nature of tubercle determination ofresistance to pressure by probe is used (for example, at
tubercular tubercles easy pressure by probe causes
destruction of tubercle with bleeding).
Tubercles appear both at infectious diseases (skin and
visceral leishmaniasis, deep mycosiss) and at illnesses
that is observed by other specialists (tuberculosis,
syphilis).
Noninflammatory tubercles are local indurations of skin
as a result of development of fibrotic tissue in the derma,
accumulations of pigmental cells and not important for
differential diagnostics of infectious diseases.
18.
Nodus (поdus) dus) is large (from 1 to 5 cm and more)formation in the layer of derma or hypoderm, rounded or oval
form as a result of specific granulomatous inflammation.
Can develop:
aqutely (nodusted erythema), elevated above the skin and
soldered with an epidermis, disappear without trace.
chronically (leprous noduss, syphilitic gummas) and
located in the deep layers of derma, dens consistency,
movable, i.e. not soldered with an epidermis, ulcerate and
disappear with formation of scar.
19.
A blister (urtica) is a noncavitary element ofinflammatory character.
Dilation of capillaries of papillary layer of derma →
increase of their permeability → exit through the
vascular wall of exsudate → compression of vessels →
the sharp limited edema of papillary layer of skin → on
the surface of skin different size and form formations
elevated above the skin suddenly develop.
Elements of rash :
In the beginning − pink-red (due to dilation of vessels),
Then it quickly blanchs (as a result of compression of
blood vessels by exsudate).
20.
The pale porcelain-white colouring is typical in acenter and pink-red on periphery.
Itch and burning of skin present.
Blisters have a tendency to the peripheric height
and confluence inter se forming circinate
garland-like rash as geographic map.
In rare cases a bubble can appear on the surface
of blister, sometimes it can exist long time.
Blisters appear at serum illness, medicinal allergy
and sometimes at some infectious diseases
(leptospirosis, viral hepatitis and other).
21.
A vesicle(vesicиla1а) is small cavernous formationcontaining a serosal or rarely serosal-hemorragic
liquid; dome-shaped vesicles have diameter 5-10
мм.
It is localised in epidermis or subepidermaly.
It appears as a result of ballooning degeneration
of cells of acanthceous layer of epidermis, with
formation of general cavity (unicameral vesicula)
or a few cavities with internal septums
(multicameral vesicula).
It can break forming superficial erosion or get
dry covering by a crust, after falling off of that an
area of unstable depigmentation forms.
22.
It can be surrounded by the halo of hyperemia orerythema, umbilicate impression appears sometimes in a
center. At suppuration of exsudate it transforms in
pustula.
Usually vesicle is one of stages of development of
exanthema (spot or roseola → papula → vesicula →
crust).
If a vesicle is broken (damaged) moist superficial erosion
pink or red color appears in its place.
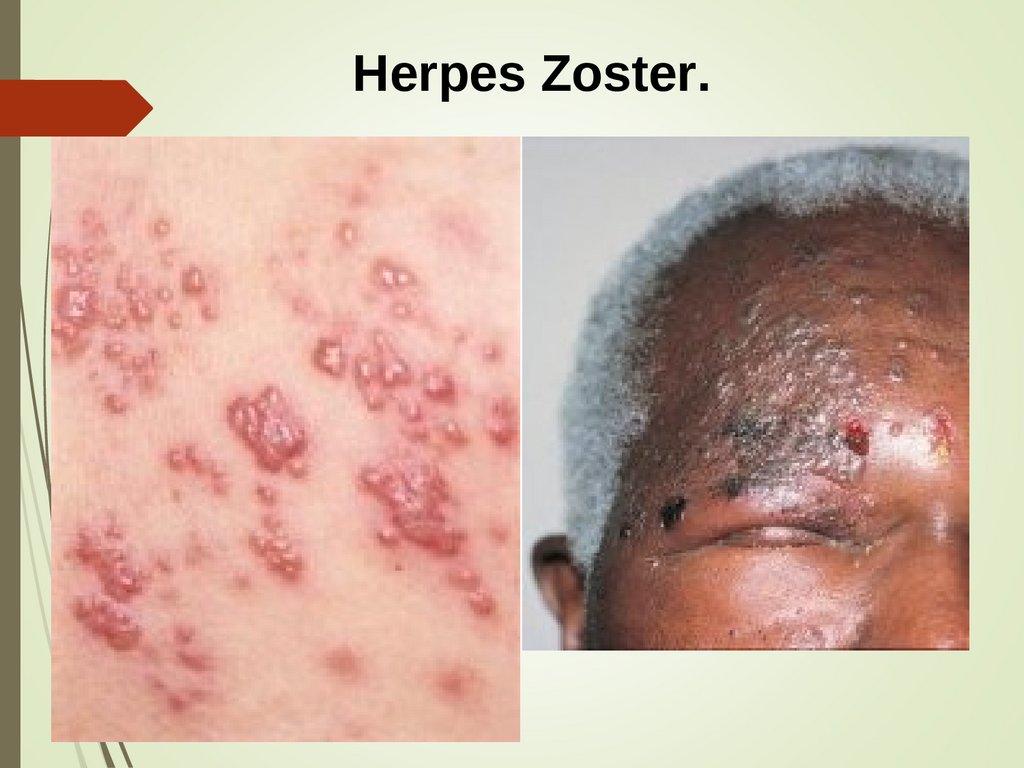
Vesicular rash is characteristic for chiken pox, small pox,
vesicular rickettsiosis, herpetic infection, herpes zoster
and other).
23.
Pustula (рustu1а),ustетаu1а), or pustule, is the vesicle also,with purulent or purulent-hemorragic exsudate.
It appears as a result of suppuration of content of
vesicula or primary (at a sepsis).
It surrounded by the halo of hyperemia.
It can be painful at palpation.
It afterwards breaks or encrusts, after falling off
of that scar forms.
Sometimes pustulas (pustules) appear on the
unchanged skin, for example small metastases of
staphylococcal infection. On occasion pustula is
initial element of development of ulcer, for
example at the skin form of anthrax.
24.
Bubble (Bи11аиla11а) is cavernous formation measuring a more than5-10 mm (up to 10 cm and more). The borders of bubble are
clear, outlines are round or oval, it is elevated above the level of
skin.
Usually − unicameral and decreases after a puncture.
At formation of bubble by confluence a few more small ones
multicamerate bubble can appear.
Cover of bubble can be tense and flabby.
Content is serosal or serosal-hemorragic.
It can be situated on a background the inflamed skin (bullous
form of erysipelas, anthrax, multiform exsudative erythema,
Stevens-Johnson syndrome and other).
Sometimes it appear and on the unchanged skin (traumatic and
other).
Bubbles are observed not only at infectious diseases, but can be
at burning, bites of snakes, at some skin diseases (pemphigus
and other).
25.
Hemorrhage is haemorrhagia different form and sizes asa result of exit of red corpuscles from blood vessels in
surrounding connecting tissue.
Because of damage (breaking) of vessel or increased
permeability of vascular wall.
Colour: red → blue → green → yellow → hazel → gray.
It disappear without trace, large in 2-3 weeks, small
quicker.
On a size and form hemorrhage is subdivided into next
elements:
petechia is dotted (1-2 mm) hemorrhage on a
background of normal skin (primary petechia at
meningococcal infection, sepsis) or on a background of
roseola (secondary petechia at spotted fever or other
rickettsiosises); brown pigmentation of skin forms at
regress.
26.
purple from 2 to 5 mm (dermatologists consider up to 2cm);
ecchymosis is large hemorrhages of incorrect figured
form by a diameter a more than 5 mm (up to 3-5 cm). It
characterizes severe duration of sepsis, meningococcal
infection. It can appear secondary at hemorragic necrosis
of skin, densible and sensible by touch, the surface is
erosive with formation of the ulcers covered by a crust,
after falling off of that scar forms.
Bruise - hemorrhage on the places of injections is not
kind of exanthema but has a diagnostic value as index of
increased fragility of vessels that is often marked at
development of hemorragic syndrome.
27.
Hemorragic transformation of rashe is hemorrhages in thepresent elements of rash (at a measles, pox, typhoid and
other).
At pressing on hemorragic elements the color does not
change.
The hemorragic elements of rash are very important for
differential diagnostics and for the detection of severity
of illness.
All exanthemas considered above behave to the primary
morphological elements of rash. However for differential
and retrospective diagnostics secondary morphological
elements have big value. It arises up, as a rule, as a result
of transformation, development of primary elements, i.e.
in later periods of disease.
28.
To secondary morphological elementsbehave
dyschromias,
scales,
crusts,
erosions,
ulcers,
scars.
29.
Erosions are defects of epidermis, appearing after broken ofcavernous primary elements (vesicles, pustula, bubbles).
The floor of erosion is or epidermis or partly papillary layer of
derma.
Size and form of erosions depends from the primary element.
Where are no proof changes of skin at healing of erosion.
Primary erosions of skin as a result of trauma do not have
diagnostic values)
Infectious diseases with erosions are same nosology with
vesicula or pustulas (chicken-pox, herpetic infection and
other).
Erosions in place of herpetic rash save a form and correspond
to the amount of vesicles.
At the syphilis erosion can appear in place of syphilitic papulae
or on a background of infiltration (hard chancre). For infectious
diseases such mechanism of origin of erosions is not
characteristic.
30.
Ulcer is deep defect of skin, epidermis, derma, and sometimesconnective tissue. Ulcers develop as a result of disintegration of
primary infiltration elements in the deep parts of derma −
tubercles, noduss, deep pustula. At the anthrax it is a result of
successive destruction of daughter's vesicula and pustula that is
formed on the edges of ulcer, so it grows on periphery.
A form and edges of ulcer are important for differential
diagnostics.
Edges of ulcer can be trenched, vertical, saucer-shaped, callous,
soft etc. Floor of ulcer can be smooth (chancre), crateriform
(syphilitic gumma), on its surface granulations (skin
leishmaniasis) can be expressed.
Always it heals with scar sizes of that corresponds to the size of
ulcer and depth of necrotizing changes.
Ulcer observs both at infectious diseases (skin leishmaniasis,
anthrax, rabbit-fever) and at the illnesses related to the
competense of other specialists (syphilis, tuberculosis, trophic
ulcers).
31.
Dyschromia is disorder of pigmentations at place aftermorphological elements of skin rash.
Hyperpigmentation or pigmentation are characterized by
the increase of amount of pigment melanin and blood
pigment of hemosiderin in the cells of basale layer of
epidermis.
It appears secondary at place of primary elements and
also after some secondary ones (erosions, ulcers).
It has as a rule brown color.
The intensity and duration are different. Sometimes it is
intensive, for example after measles with a hemorragic
impregnation of rash; sometimes it is low intensive brown
spot (typhoid) disappears quickly and without trace.
32.
A squama is loosened cells of horny layer losingconnection with an epidermis. In a norm it takes place
constantly in a small amount and remains unnoticeable.
At illnesses with the damage of skin squamas appear in
great numbers in place of primary elements of rash.
The small lamellar branny desquamatетаion is
observed at a measles, scaly skin disease when a
skin is like sprinkled by a flour.
Large lamellar desquamatетаion is characterized by more
large size of squamas and can become separated from
whole layers (scarlatina, pseudotuberculosis, dermatitis).
Desquamation appears in the period of recovery at
infectious diseases.
33.
A crust is product of condensing and drying out ofdifferent sort of exsudates of other elements of rash
(pustula, vesicula, erosions, ulcers).
Types:
serosal crusts (semitransparent or grey),
purulent (yellow or sulphur),
hemorragic (brown or crimson).
The size of crusts corresponds to the size of the element
preceded to its. Crusts appear at a herpetic rash, chicken
and natural pox, zoster and other
Formation of crusts is characteristic for very many skin
illnesses (impetigo, vulgar ecthyma, pyoderma and other).
34.
A scar is rough fibrose connective-tissueformation substituting deep defects of skin.
Fresh scars have the pink-red colouring, its
surface glitters.
Old scars can be both hyperpigmentated and
depigmentated.
Flat scars are elevated above skin (keloid).
Atrophic scars are thin and placed below level of
skin correspond to substituted defect of skin.
At infectious pathology it meets at all illnesses
with ulcers, rarely small scars appear at place of
pox pustula (smallpox).
35.
For differential diagnostics of exanthemas atinfectious diseases the following is needed.
Accurate inspection of skin at good illumination
to find single elements of rash.
Exposure and exact determination of type of
elements of rash.
A term of appearance of rash is a very important
sign. In one cases an exanthema appears from the
first day of illness (scarlatina, rubella, infectious
erythema and other), at other cases - from a 3-4th
day (measles, Marseille fever and other), and,
finally, relatively late appearance of rash
(leptospirosis, typhoid fever) is possible.
36.
Predominant localization of elements of rash or place of«condensing» of exanthema. For example, at scarlatina
and pseudotuberculosis the elements of rash are more
thickly located in the natural folds of skin (ulnar bends,
inguinal folds), at infectious erythema of Rosenberg − in
area of large joints and in area of sacrum; at a measles
rash starts on face, at typhoid fever - on the skin of
stomach, at spotted fever − on the sides of trunk et cetera
At the exposure of rash stage of rashing and other
features specify. For example, at a measles in the 1th day
rash appears on face and neck, on 2th − on a trunk and
hands, on the 3th day − on feet. At other illnesses
(enteroviral exanthema, infectious mononucleosis,
medicamental rash) a «morbilliform rash» appears at the
same time instant on face, trunk and extremities.
37.
Duration of existence of elements of rash is alsoimportant. For example, at typhoid fever roseolas
saved only 2-4 days, and then without trace
disappear. At other illnesses roseola can be saved
considerably longer.
The repeated rashing has a differential-diagnostic
value also. At spotted fever roseolar (or roseolarpetechial) rash appears at the same time instant and
new elements do not appear, at typhoid fever new
roseolas can appear at next wave of fever.
Confluence of elements of rash can have a diagnostic
value. At a measles, infectious mononucleosis,
leptospirosis elements of rash often form
erythematous fields, but at the rubella such tendency
is absent.
38.
It should be remembered that an exanthema appears notonly at infectious diseases, diagnostic errors are possible.
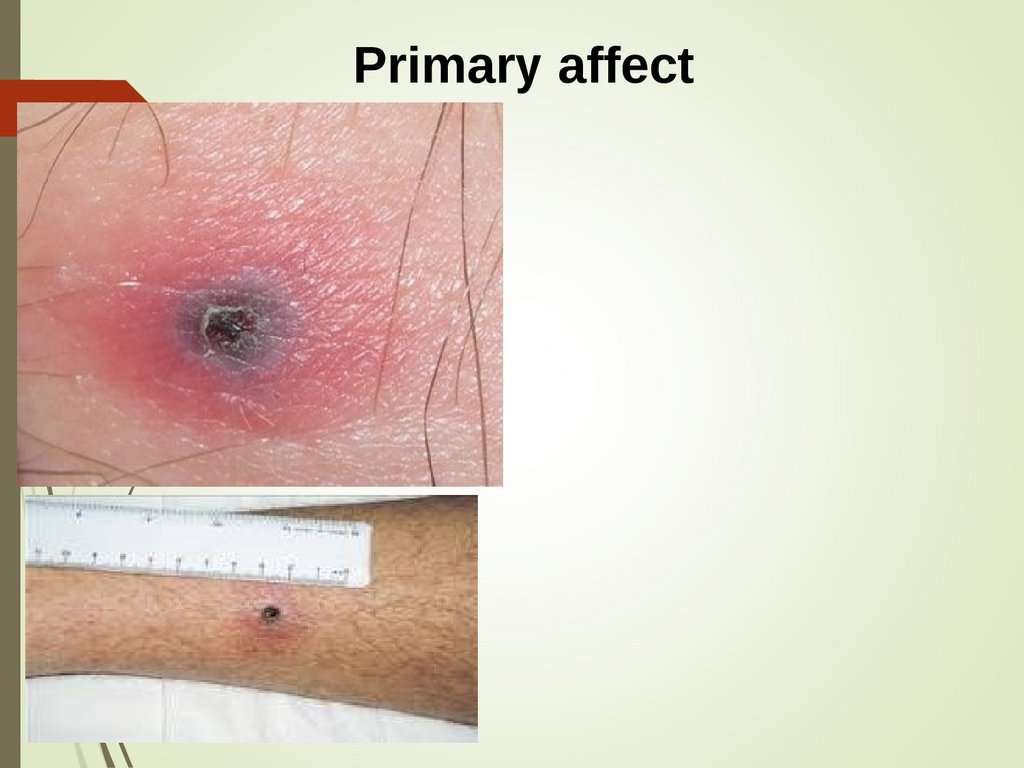
Primary affect is specific damage of skin in the place of
introduction of causative agent, frequently with regional
lymphadenitis. It presents at infectious diseases with the
transmissive or (rarer) contact mechanism of
transmission of causative agent. Appearance of primary
affect, as a rule, is preceded to other symptoms of illness
and serves as an important diagnostic symptom.
Enanthema is local discrete damage of mucous
membrane, analogical to the skin rash. It has important
clinical and diagnostic value.
39.
Disseminated intravascular coagulation (DIC)DIC can develop practically for any patient at:
febricity;
thrombocytopenia,
decrease of coagulant factors at blood
Gram-negative bacteriaemia.
Stages of DIC:
а) hemorragic diathesis;
б) sedimentations of fibrinogenum in small
vessels with subsequent ischemic damage of
tissues;
в) haemolytic anaemia at haemolysis at blocked
by fibrin small blood vessels.
40.
For diagnosis DIC next analyses areused:
CBC and amount of thrombocytes,
time of coagulation, prothrombine time,
level
of
fibrinogenum,
fibrinolytic
activity,
if it is possible, measuring of coagulant
factors V and VIII.
41.
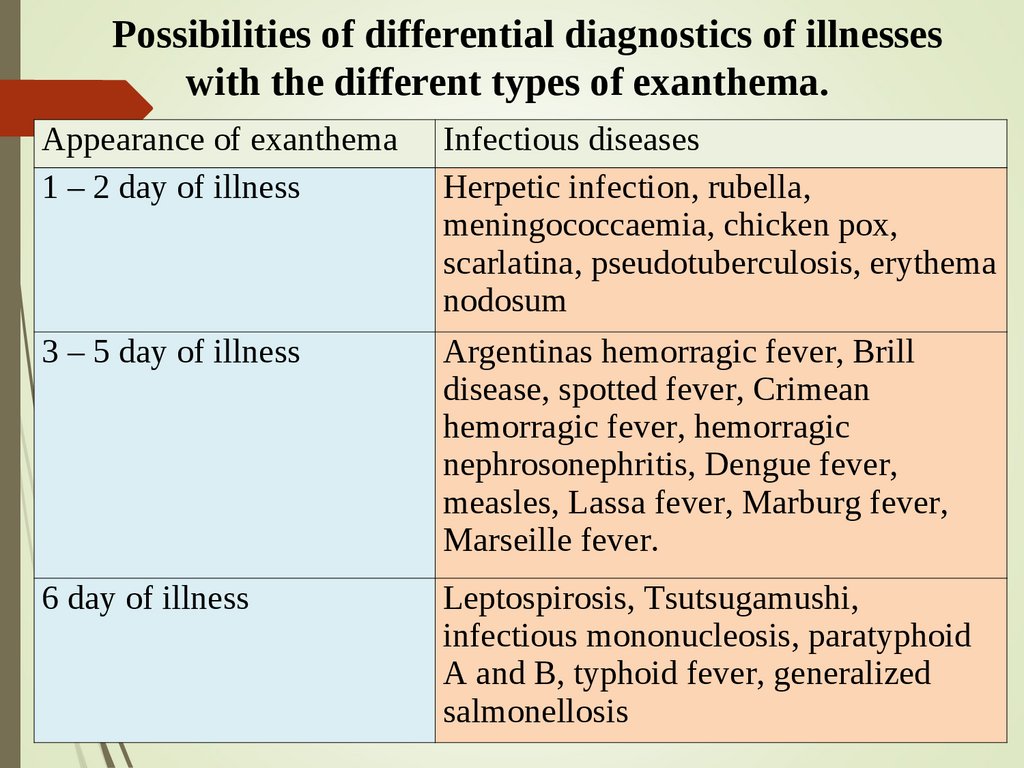
Possibilities of differential diagnostics of illnesseswith the different types of exanthema.
Appearance of exanthema
1 – 2 day of illness
3 – 5 day of illness
6 day of illness
Infectious diseases
Herpetic infection, rubella,
meningococcaemia, chicken pox,
scarlatina, pseudotuberculosis, erythema
nodosum
Argentinas hemorragic fever, Brill
disease, spotted fever, Crimean
hemorragic fever, hemorragic
nephrosonephritis, Dengue fever,
measles, Lassa fever, Marburg fever,
Marseille fever.
Leptospirosis, Tsutsugamushi,
infectious mononucleosis, paratyphoid
A and B, typhoid fever, generalized
salmonellosis
42.
Possibilities of differential diagnostics of illnesseswith the different types of exanthema.
Enanthema: measles, rubella, chicken-pox, herpangina.
Hyperemia of face : Brill disease, hemorragic nephrosonephritis,
influentza, Dengue fever, yellow fever, Q-fever, Marburg fever,
Pappatachi, Tsutsugamushi, leptospirosis, spotted fever.
Icterus: viral hepatitis, malaria, yellow fever.
Hemorragic syndrome: hemorragic fevers, meningococcemia, hepatic
coma.
Inflammation of mucous membranes of upper respiratory tract:
adenoviral infection, flu, herpetic infection, Dengue fever, yellow fever,
measles, rubella, Pappatachi.
Pneumonia: psittacosis, illness of legionariess, CMV-infection,
leptospirosis, meningococcal pneumonia, typhoid fever, rickettsiosises,
influentza, measles, anthrax, rabbit-fever, plague.
Tonsillitis: diphtheria of pharynx, rabbit-fever, infectious
mononucleosis, scarlatina, typhoid fever.
Diarrhea: shigellosis, cholera, salmonellosis, yersiniosis,
pseudotuberculosis.
43.
Measles44.
Measles45.
46.
Typhoidfever
47.
Riccetsiosises48.
Pseudotuberculosis49.
Primary affect50.
Primary affect51.
Enanthema52. Meningococcaemia
53.
Small-pox54.
55.
Herpes Zoster.56. Skin leishmaniasis
57.
58.
Lyell'ssyndrome