








 medicine
medicineSimilar presentations:










Objective physical examination in cardiovascular diseases: visual examination
1. Theme: objective physical examination in cardiovascular diseases: visual examination
2.
3.
4. Measurement of Vital Signs
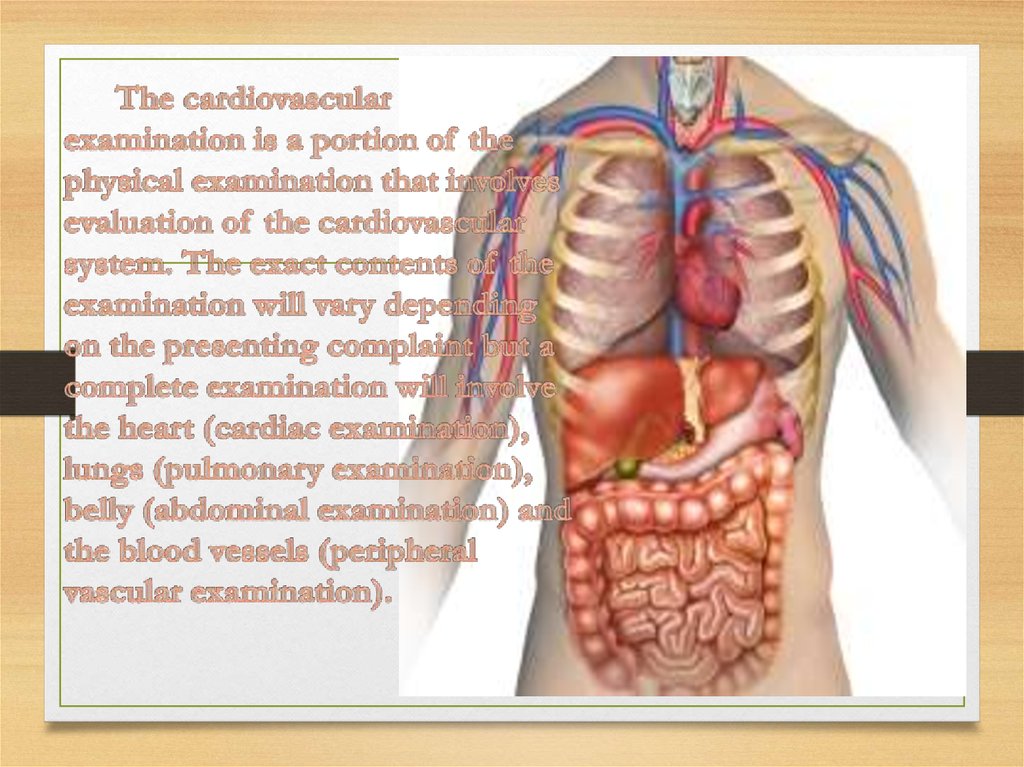
A good cardiac examination starts as soon you can lay eyes on the patient.Doctors will observe the color of skin, rate of breathing, and emotional state of
their patients at a distance before the examination begins. An accurate blood
pressure and heart rate should be measured, as these are direct measurements of
how well the heart is working. An automatic blood pressure cuff can be used,
but a healthcare professional can also use a manual blood pressure cuff and
stethoscope. The bell of the stethoscope should be placed over the brachial
artery when taking a blood pressure manually: the pressure meter when the first
two heart beats are heard will show the systolic blood pressure; when the sounds
disappear, the meter will show the diastolic blood pressure. A normal systolic
blood pressure will be less than 120 mm Hg, and a normal diastolic blood
pressure will be less than 80 mm Hg. A blood pressure that is more than 15 mm
Hg different between the right and left arm may indicate a problem with the
patient's blood vessels.A normal heart rate is between 60 and 100 beats per
minute. This can be measured wherever a pulse can be felt, but is usually
measured from the radial artery. Vital signs should be measured at least twice
during each patient encounter, with as much time as possible between
measurements (e.g. once at the beginning and once at the end of the
appointment). A heart rate and rhythm that is normal may be written down as
"RRR".
5.
6.
• Many clues to the cardiac condition can be detectedwith a simple visual inspection. In the acutely unwell
patient, cyanosis, pallor, and sweatiness can all be
signs of impending danger – does the patient "look"
ill? In nonacute patients, cachexia is perhaps the most
important feature to note on general inspection since
it is an important prognostic sign in heart failure.
Palpation is essential to confirm that girth is excess
fluid (pitting edema) Certain physical appearances
should always prompt an awareness of cardiac
abnormalities. Facial signs for which there is evidence
of an association with cardiac conditions are shown
in.Finally, it is important to document the condition
of a potential cardiac patient's teeth.
7.
• Complete examination of all systems is essential to detectperipheral and systemic effects of cardiac disorders and evidence
of noncardiac disorders that might affect the heart. Examination
includes the following:
• Vital sign measurement
• Pulse palpation and auscultation
• Vein observation
• Chest inspection, and palpation
• Cardiac percussion, palpation, and auscultation Lung
examination, including percussion, palpation, and auscultation
• Extremity and abdomen examination
• Cardiac auscultation is discussed in a separate topic. Despite the
ever-increasing use of cardiac imaging, bedside auscultation
remains useful as it is always available and can be repeated as
often as desired without cost.
8.
Palpation• Before auscultation, inspection of the precordium can be a useful
indicator of previous surgery – eg, midline sternotomy suggests
previous bypass, lateral thoracotomy suggests previous mitral valve
or minimally invasive bypass surgery (left internal mammary artery
to left anterior descending coronary artery). Locate the apex beat –
the furthest point laterally and inferioraly where you can clearly feel
the apex (usually the fifth intercostal space in the midclavicular line).
There are many different descriptions for abnormal apex beats. One
scheme distinguishes heaving (high afterload, eg, aortic stenosis)
from thrusting (high preload, eg, aortic regurgitation). The apex may
also be "tapping", but this reflects a loud first heart sound. In
addition, you should place your left hand over the sternum and feel
for any significant ventricular heave (right ventricular hypertrophy)
or thrill (tight aortic stenosis, ventricular septal defect).
9.
• Auscultation• Held by many as the key to physical examination, the
importance of auscultation remains, but is diminished in an
age of increasingly portable echocardiography.Listen over the
aortic (second right intercostal space) and pulmonary (second
left intercostal space) areas and at the left lower sternal edge
with the diaphragm of your stethoscope (better for higher
pitches), then use the bell for the apex (better for lower pitches).
If in doubt, use both. Press lightly with the bell. If you hear an
abnormality over the aortic or pulmonary areas, you should
listen over the carotids. If you hear an abnormality at the apex,
listen in the axilla. Listen systematically. Start with the heart
sounds – ignore everything else
10.
• Percussion• There was a time when cardiac percussion was considered a useful
addition in the clinical evaluation of the patient with heart disease.
This skill has been largely lost with the advent of new imaging
techniques such as X-ray and echocardiography, both of which are
more accurate in defining cardiac size and borders and detecting the
presence and extent of pericardial fluid.
• In the fast-paced world of modern medicine, do cardiologists spend
time percussing the chest, trying to sort out if there is cardiomegaly
or fluid in the pericardium, when in minutes they could have a more
accurate and definitive diagnosis with echocardiography? The honest
answer is no. However, cardiac percussion skill as well as knowledge
of its implication might provide quick information at the bedside,
most especially in significant pericardial effusion, pending
confirmation with echocardiography
11.
Triglycerides
Lower blood triglycerides by:
Not overeating
Limiting alcohol and simple sugars
Spreading meals throughout the day
Including fatty fish in the diet
Controlling diabetes if present
Performing regular physical activity
Not smoking
12.
• Further reading:• 1. Bickley LS, Hoekelman RA, editors. Bates' Pocket
Guide to Physical Examination and History Taking, 3rd
edn. Lippincott Williams & Wilkins, 2000.
• 2.Gleadle J. History and Examination at a Glance.
Blackwell Science, 2003.
• 3.Perloff JK. Physical Examination of the Heart and
Circulation, 3rd edn. WB Saunders, 2000.
• 4.Turner RC, Blackwood RA. Lecture Notes on Clinical
Skills, 3rd edn. Blackwell Science, 1997.