













")








 medicine
medicineSimilar presentations:
")




")
")
")


Clinical Case Conference
1. Tuesday Clinical Case Conference
4/08Zae Kim, MD
2. Bartter-like salt losing tubulopathies History
• In 1962, Frederic Bartter– Reported two patients with
• Hypokalemic alkalosis
• normal blood pressure despite high aldosterone production
• Growth and mental retardation
• Muscle weakness and cramps
• Salt craving and constipation
• Polydipsia and polyuria
– Lab:
• K 2-2.2 meq/L, HCO3 30-34 mmol/L, sCl 75-66 meq/L
– Endocrinologist’s approach = adrenalectomy
• Hyperplasia of the zona glomerulos
• Renal bx: hyperplasia of the juxtaglomerular apparatus
3. Bartter-like salt losing tubulopathies History
• Works of McCredie, Fanconi, Dillion– Two quite distinct clinical presentations of BS
identified within the group of pediatric Bartter patient
• Neonatal variant of BS
– The most severe form
– Polyhydramnios, premature delivery
– Growth retardation
– marked hypercalciuria leading to nephrocalcinosis
• Classical Bartter syndrome
– Insidious onset in infancy
– Present with failure to thrive
– Nephrocalcinosis is typically absent (hypercalciuria to lesser extent)
4. Bartter-like salt losing tubulopathies History
• Gitelman syndrome– Reported in 1966
– “a new familial disorder characterized by hypokalemia and
hypomagnesemia” in two adult sisters
– Clinically:
• Often present in early adulthood
• Predominantly musculoskeletal symptom
– Carpopedal spasm and normal growth
– Biochemical
• Hypokalemia, but less marked than BS
• Hypomagnesemia is constant finding
• Pronounced hypocalciuria, where as BS have nl-to-high
• BS with polyuria, 2/2 reduction of urinary concentrating ability, not
present in Gitelman patients
5. Bartter-like salt losing tubulopathies History
• Contribution by geneticists– 1996
• Simon et al
– Gitelman disease = mutation of gene on Chr 16 = NaCl
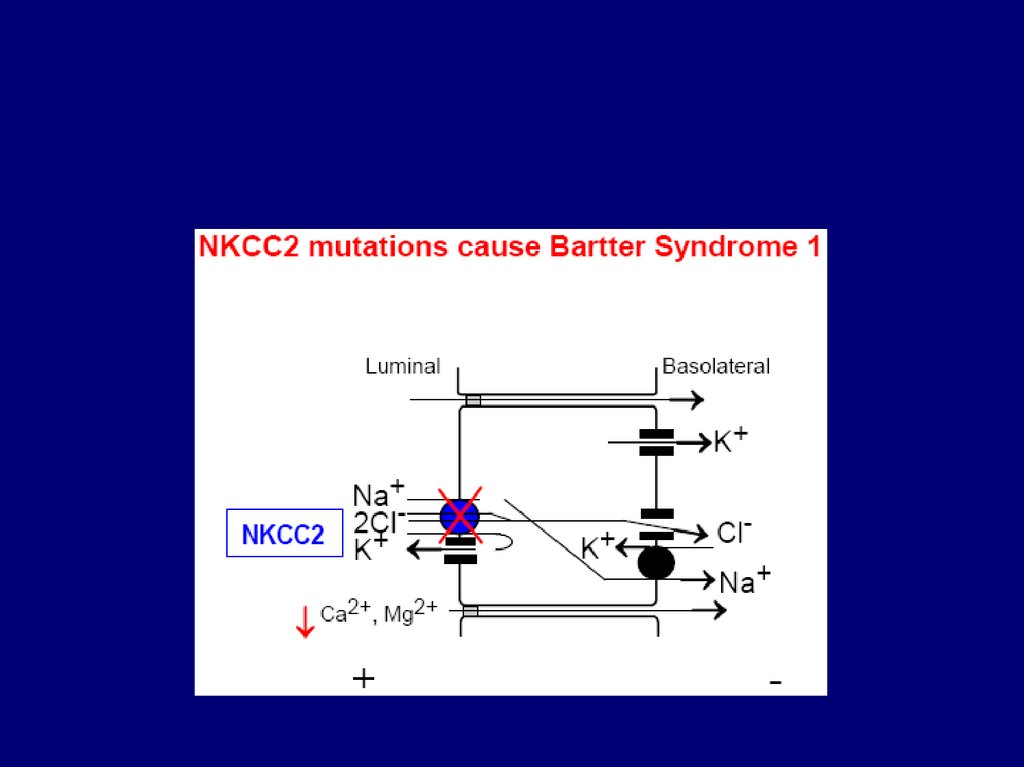
– neonatal variant of BS (BS I) = mutations of gene on on Chr 15 = NaK2Cl cotransporter
• Lifton
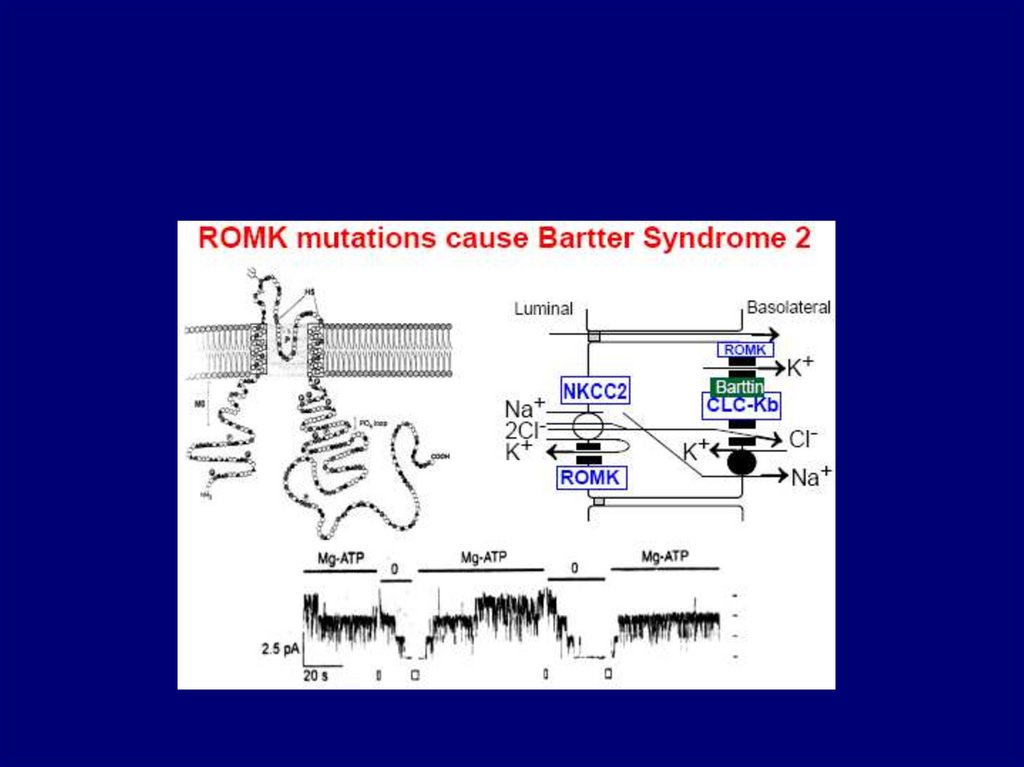
– BS II = ROMK channel
– 1997
• Lifton
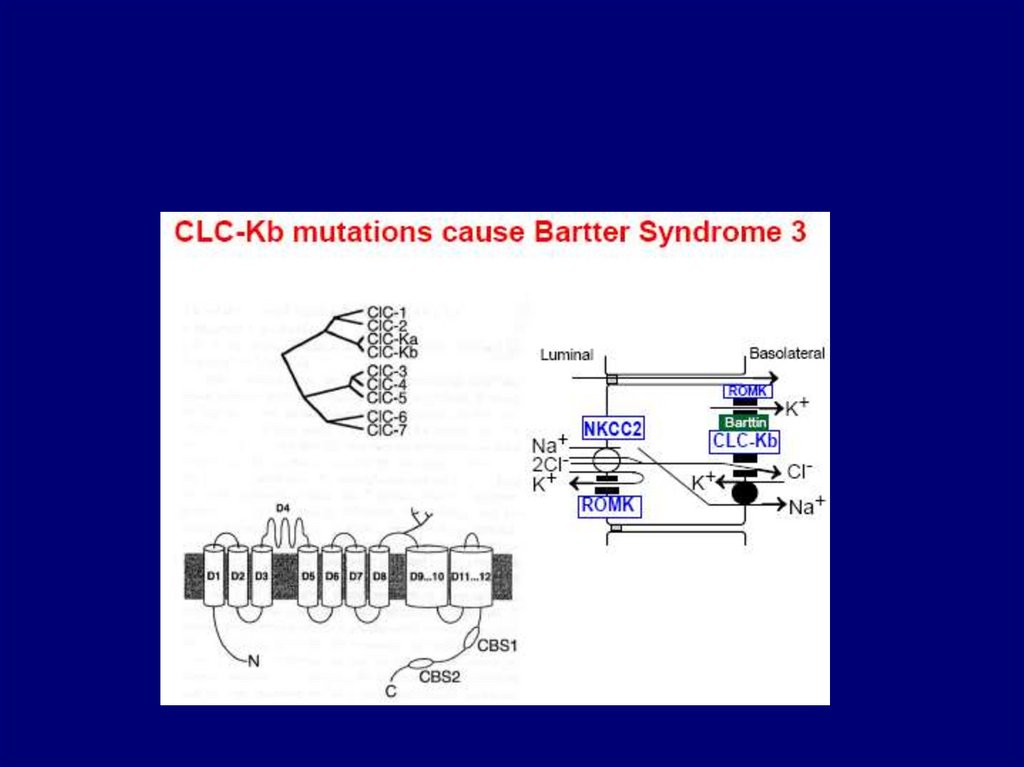
– BS III = mutation of gene on chr 1 = ClCNkb
– 2001
• Landau
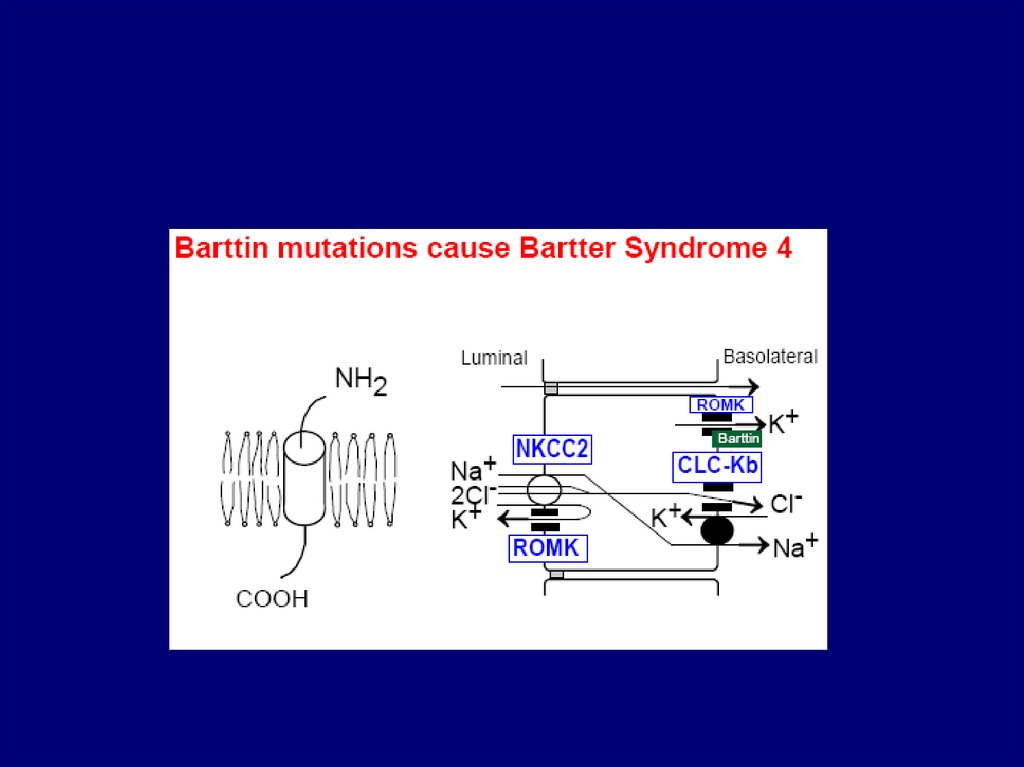
– BSND = mutation of gene on ch 1 = “Barttin”
– Knock-out animal model exist for Gitelman and Bartter type I and II
– Genetic testing – hampered by…
• Large gene dimensions, lack of hot-spot mutations, heavy workup time,
and costs
6. Clinical and biochemical features of Gitelman's syndrome and the various types of Bartter's syndrome
Clinical and biochemical features of Gitelman'ssyndrome and the various types of Bartter's syndrome
Phillips DR et al. (2006) A serum potassium level above 10 mmol/l in a patient predisposed to hypokalemia
Nat Clin Pract Neprol 2: 340–346 doi:10.1038/ncpneph201
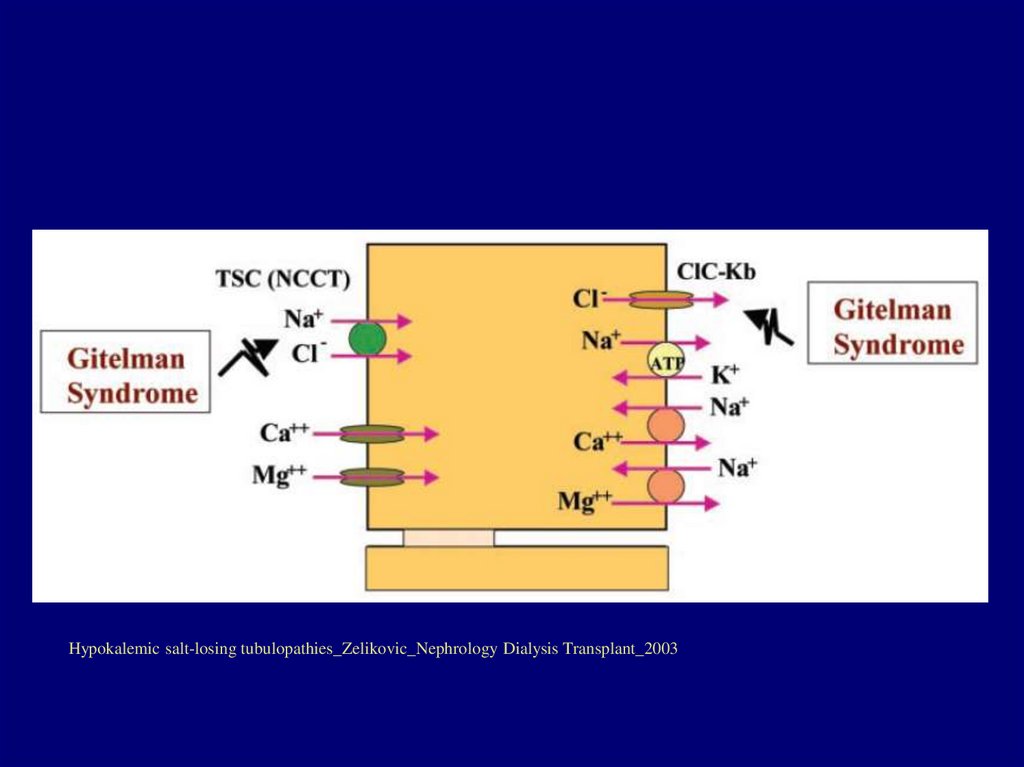
7. Pathyphysiology
8. Pathophysiology
Hypokalemic salt-losing tubulopathies_Zelikovic_Nephrology Dialysis Transplant_20039.
10.
11.
12.
13. BSND – a model of K+ secretion in the inner ear
Bartter syndrome_Herbert_CurrOpinHTNNeph_200314.
Hypokalemic salt-losing tubulopathies_Zelikovic_Nephrology Dialysis Transplant_200315. Cascade of events
Salt lossVolume depletion
Renin/aldosterone secretion / JGA hyperplasia
autonomous hyperreninemic hyperaldosteronism
Enhanced K and H secertion at the collecting tubule
Hypokalemia and metabolic alkalosis result
16. Diagnosis
• Clinical history and biochemical workup may not allowdefinite diagnosis
– Especially concerning the different types of tubular disorders
• Genetic diagnosis
– Costly, cumbersome, and time-consuming because
• Great dimension of most genes
– Five exonic regions for ROMK to 26 exons for SLC12A1 and SLC12A3
• Lack of hot-spot mutations
– Recognized mutations evenly distributed along the whole gene
• And very large number of mutations
• Test with diuretic?
17. A Thiazide Test for the Diagnosis of Renal Tubular Hypokalemic Disorders Colussi, et. Al, CJASN, 2007
• In cohort of patients with genetically proven GS or BSdiagnosis, sensitivity and specificity of diuretic test with
oral HCTZ was evaluated
– GS, n=41
• 19 pediatric and 22 adult patients
– BS, n=7
• five type I, two type III
– “pseudo-BS”, n=3
• two from surreptitious diuretic intake and one from vomiting
• TEST: administration of HCTZ and measurement of the
maximal diuretic-induced increase over basal in the
subsequent 3h of chloride fractional clearance
18. Blood and urine biochemical data in patient groups
19. Group results of HCT test
20. Individual hydrochlorothiazide test results (as maximal increase in fractional chloride clearance)
21.
• Traditional parameters– Age, plasma Mg and urine Ca excretion lack
specificity
• Blunted natriuretic and chloruretic response to
HCT correctly recognizes GS from BS and from
PB
• Small number of BS and PB in the study
22. Treatment
• Antenatal BS / Classic– Replacement therapy
• Fluid loss may surpass 50cc/kg/d with very large loss of Na
(~45meq/kg/day)
• K supplement
– Rx
• Prostaglandin synthetase inhibitors (indomethacin)
• Gitelman
– Mg / K supplement
– Spironolactone or amiloride
23.
24.
25. Pathophysiology
NameNumber
Assoicated
gene mutation
Neonatal Bartter’s syndrome
Type 1-2
NKCC2 (Chr 15)
or ROMK (Chr
11)
Classic Bartter’s syndrome
Type 3
CLCNKB
Bartter’s syndrome with
sensorineural deafness
Type 4
BSND
Gitelman’s syndrome
NCCT (SLC12A3)
26. Gitelman syndrome
• Reported by Gitelman few years after Bartter– Similar syndrome characterized by
• Hyperreninemia, metabolic alkalosis, and impaired renal
conservation of Mg and K
– In contrast
• Often diagnosed in adolescence or early adulthood
• Asymptomatic finding on routine lab test
• Predominant muscular symptoms
• Mutation
– Inherited as autosomal recessive
– Inactivating mutations in the SLC12A3 gene
• Loss of function of NCCT in DCT
• chr 16q13
27. Age at manifestation and primary symptoms of genetically defined salt-wasting kidney disorders
Mechanism of disease the kidney-specific chloride channesl_Kramer_NatureClinicPractNeph_200728. Bartter Syndrome – clinical manifestation
• typically manifests early in life with– polyhydramnios, failure to thrive, growth retardation, polydipsia,
dehydration, salt craving, and marked muscle weakness.
– Blood pressure is characteristically low or normal.
– The GFR is normal, but there is inadequate urinary acid
excretion after NH4Cl challenge.
– Nephrogenic diabetes insipidus also may be seen.
– Sodium transport in erythrocytes and salivary glands is
impaired
– As early as 1975 Kurtzman and Gutierrez (281) postulated that
Bartter syndrome resembled one of inhibited function of the
thick ascending limb
• most recent genetic studies seem to confirm this proposal.
• Renal biopsy demonstrates hyperplasia and hypertrophy of the
juxtaglomerular cells as well as of the medullary interstitial cells,
the site of prostaglandin E2 synthesis.
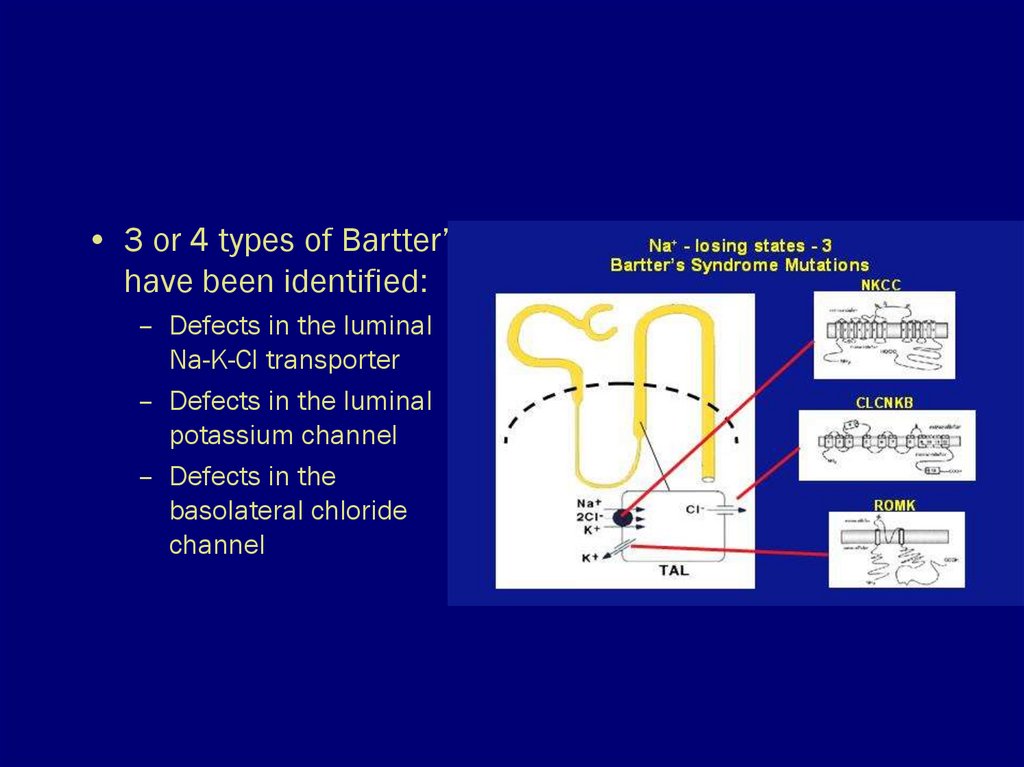
29.
• 3 or 4 types of Bartter’shave been identified:
– Defects in the luminal
Na-K-Cl transporter
– Defects in the luminal
potassium channel
– Defects in the
basolateral chloride
channel
30. Gitelman’s syndrome
• Like Bartter’s an autosomal recessive disorder,but not usually diagnosed early in life.
• Findings mimic administration of a thiazide
diuretic: the defect is in the Na-Cl transporter.
• Patients may complain of polyuria, cramps.
• They do not have hypercalciuria, but typically
have low serum magnesium levels.