





 medicine
medicineSimilar presentations:










Internal medicine. Cerebrovascular accident
1.
INTERNAL MEDICINECEREBROVASCULAR
ACCIDENT.
By Dr. KANDA P.R
2.
BRIEF ANATOMICAL SUMMARYThe brain has three layer covering which allows it to be
suspended in CSF.
The brain is divided anatomically into many different
areas.
The functional parts
1. The forebrain
2. The midbrain
3. The hindbrain
• The circle of Willis ensures a high arterial blood supply
with the possibility of compensatory blood supply in
CVA.
3.
DEFINITION• STROKE
• A stroke is an acute neurological deficit lasting
longer than 24hrs
• TIA (TRANSIENT ISCHAEMIC ATTACK)
• An acute neurological deficit lasting less than
24hrs
4.
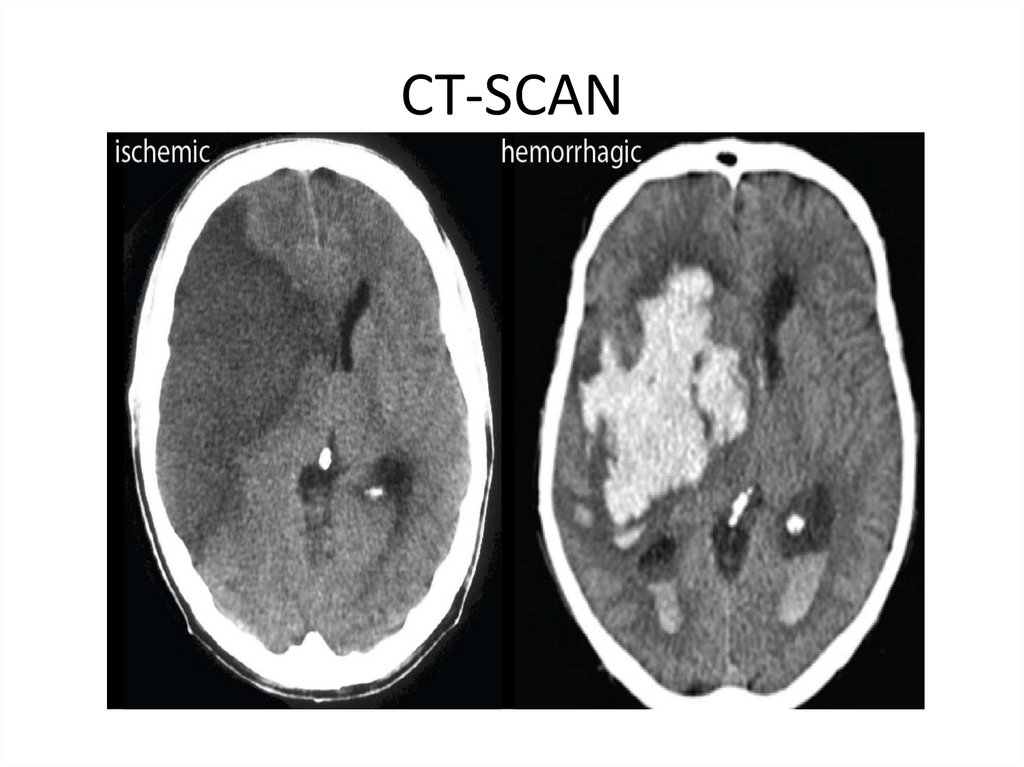
Types Of CVA• Ischaemic stroke/ Infarction (80-90 %)
• Haemorrhagic (10-20%)
• TIA
5.
CAUSES1.
2.
3.
4.
1.
2.
1.
2.
3.
4.
PRIMARY
Thrombosis
Atherothromboembolism
Heart emboli
CNS bleed (High BP, Trauma, Aneurysm rupture)
Rare Causes
Vasculitis
Venus sinus thrombosis
Young Patients
Thrombophilia
Vasculitis subarachnoid haemorrhage
Venus-sinus thrombosis
Carotid artery dissection
6.
PRESENTATION• CEREBRAL HEMISPHERE INFARCTS: Initially
flaccid then spastic contra-lateral sensory loss,
heminopia, dysphagia
• BRAIN STEM INFARCTION: Quadriplegia
(paralysis affecting all four limbs),
disturbances of gaze & vision, locked-in
syndrome
• LACUNAR INFARCTS: Poor motor/sensory
signs, ataxia, intact cognition/consciousness
7.
• Most commonly in our set up, CVA’s are usually as a resultof a CNS bleed.
• C/F may include;
1. Sudden severe headache
2. Projectile vomiting
3. Sudden loss of consciousness
4. In and out of lucid states
5. Coma within hours
6. Meningism
7. Carotid bruit
8. Atrial Fibrillation
9. Past TIA
10. Ischaemic Heart Disease
11. Loss of coordination/ difficulty with balance/ clumsiness
• Symptoms typically occur on one side of the body
8.
INVESTIGATIONSNeeds to be prompt
Confirm your clinical Dx (Exclude other causes e,g Tumor)
GCS
Cranial nerve examination
Neurological Examination
Baseline (FBC/ U&Es/Clotting time/ESR)
RBS
Lipid Profile
Hyperviscosity
R/O Infection
Prothrombotic states (Blood clotting disorders – thrombophilia)
CT SCAN
9.
• Non Contrast CT is the gold standard forhaemorrhagic stroke
• MRI
• Other: CXR/ ECG/ECHO
10.
CT-SCAN11.
MANAGEMENT• Non Pharmacological Rx : Physiotherapy remains
the main stay of treatment.
• Other: Psychological support, Nutritional support.
• Pharmacological Rx : May depend upon the cause
and type of infarction, ( Altepase, Anticoagulants,
Antihypertensives and Anticonvulsants when
needed)
• Intracerebral bleeds secondary to Haemorrhage
is managed with surgical intervention.
• Key component is to maintain perfusion to the
brain tissue , keepn pt well hydrated and fed.
12.
PROGNOSIS• All depends on the extent of the CVA and if
Haemorrhagic the locatioa/area of the bleed.
• Early diagnosis and iniktiation of care however
proves beneficial.
13.
THE ENDTHANK YOU