



















 medicine
medicine english
englishSimilar presentations:



")






Основы микрохирургии. Микрососудистый шов
1.
ОСНОВЫ МИКРОХИРУРГИИ.МИКРОСОСУДИСТЫЙ ШОВ.
FUNDAMENTALS OF MICROSURGERY.
MICROVASCULAR SUTURE.
2.
ПЛАН• 1 ОПТИЧЕСКИЕ СРЕДСТВА УВЕЛИЧЕНИЯ В
МИКРОХИРУРГИИ
• 2 МИКРОХИРУРГИЧЕСКИЕ ИНСТРУМЕНТЫ
• 3 ИГЛЫ И ШОВНЫЙ МАТЕРИАЛ
• 4 ОБЩИЕ ПРИНЦИПЫ МИКРОХИРУРГИЧЕСКОЙ
ТЕХНИКИ
• 5 МИКРОСОСУДИСТЫЙ ШОВ (АНАСТОМОЗ
«КОНЕЦ В КОНЕЦ», «КОНЕЦ В БОК», «БОК В БОК»)
3.
PLAN• 1 - Optical magnification in microsurgery
• 2 - Microsurgical instruments
• 3 - Needles and suture
• 4 - General principles of microsurgical technique
• 5 - Microvascular suture (end-to-end, end-to-side, side-toside anastomosis)
4.
ОПТИЧЕСКИЕ СРЕДСТВАУВЕЛИЧЕНИЯ В МИКРОХИРУРГИИ
ОСНОВНОЙ
ДИАПАЗОН
УВЕЛИЧЕНИЯ В
МИКРОХИРУРГИИ
СОСТАВЛЯЕТ ОТ 5
ДО 40 КРАТ.
ДЛЯ УВЕЛИЧЕНИЯ
ПРИМЕНЯЮТ
МИКРОСКОПЫ И
ОПЕРАЦИОННЫЕ
ЛУПЫ.
5.
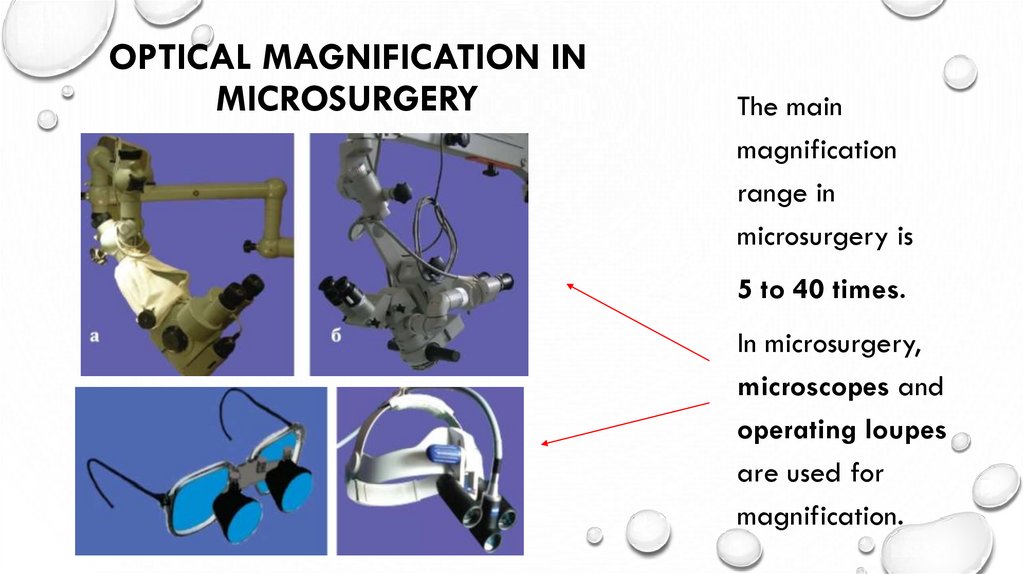
OPTICAL MAGNIFICATION INMICROSURGERY
The main
magnification
range in
microsurgery is
5 to 40 times.
In microsurgery,
microscopes and
operating loupes
are used for
magnification.
6.
ВИД ОПЕРАЦИОННОГО ПОЛЯ - ЭТОРЕЗУЛЬТАТ ОПРЕДЕЛЁННОГО СОЧЕТАНИЯ НАБОРА
ЛИНЗ ПРИ ПОДДЕРЖКЕ ИНДИВИДУАЛЬНОГО
ВЫСОКОИНТЕНСИВНОГО ИСТОЧНИКА ОСВЕЩЕНИЯ.
ДВА И БОЛЕЕ НАБОРА ЛИНЗ ПОЗВОЛЯЮТ ХИРУРГУ
И АССИСТЕНТУ ВИДЕТЬ ОПЕРАЦИОННОЕ ПОЛЕ И
НАСТРАИВАТЬ УВЕЛИЧЕНИЕ И ФОКУС НЕЗАВИСИМО
ДРУГ ОТ ДРУГА - ДИПЛОСКОП, ТРИПЛОСКОП.
ВИДЕОКАМЕРА ПОЗВОЛЯЕТ ОСТАЛЬНЫМ
УЧАСТНИКАМ ОПЕРАЦИИ НАБЛЮДАТЬ
ОПЕРАЦИОННОЕ ПОЛЕ НА ЭКРАНЕ ДИСПЛЕЯ.
РАБОТА С ОПЕРАЦИОННОЙ ЛУПОЙ
ХАРАКТЕРИЗУЕТСЯ МАЛЫМ УВЕЛИЧЕНИЕМ И
ТРЕБУЕТ ПОСТОЯННОГО КОНТРОЛЯ ПОЛОЖЕНИЯ
ГОЛОВЫ ДЛЯ СОХРАНЕНИЯ ФОКУСНОГО
РАССТОЯНИЯ.
7.
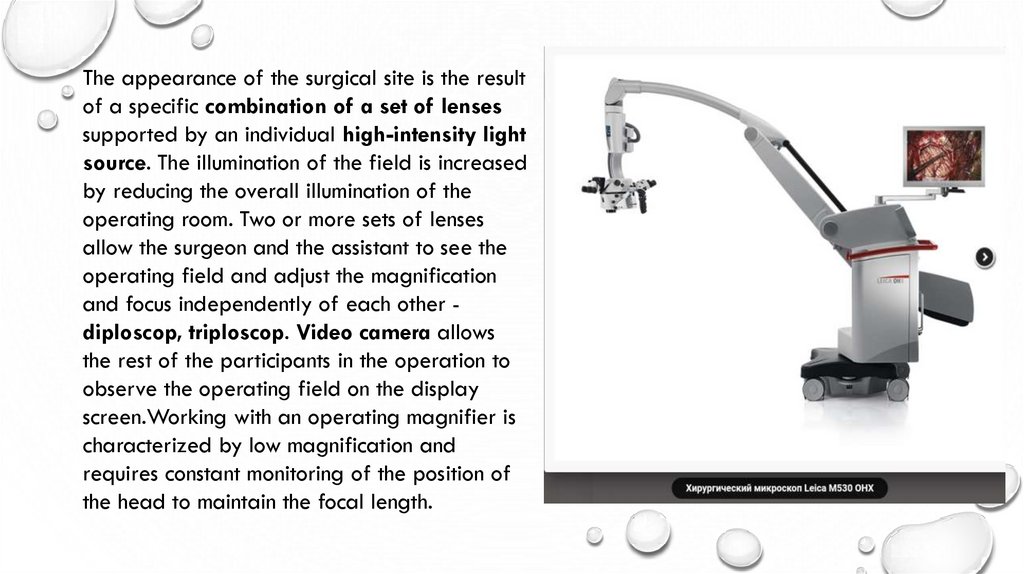
The appearance of the surgical site is the resultof a specific combination of a set of lenses
supported by an individual high-intensity light
source. The illumination of the field is increased
by reducing the overall illumination of the
operating room. Two or more sets of lenses
allow the surgeon and the assistant to see the
operating field and adjust the magnification
and focus independently of each other diploscop, triploscop. Video camera allows
the rest of the participants in the operation to
observe the operating field on the display
screen.Working with an operating magnifier is
characterized by low magnification and
requires constant monitoring of the position of
the head to maintain the focal length.
8.
МИКРОХИРУРГИЧЕСКИЕ ИНСТРУМЕНТЫМИКРОХИРУРГИЧЕСКИЕ ИНСТРУМЕНТЫ ИМЕЮТ РЯД ОТЛИЧИЙ ОТ
ТРАДИЦИОННЫХ ИНСТРУМЕНТОВ:
ВО-ПЕРВЫХ, ОНИ ДОЛЖНЫ БЫТЬ ПРИГОДНЫ ДЛЯ ТОНКИХ МАНИПУЛЯЦИЙ
НА ЕДВА ВИДИМЫХ НЕВООРУЖЁННЫМ ГЛАЗОМ СТРУКТУРАХ, ОДНАКО
ОБЛАДАТЬ ДОСТАТОЧНО БОЛЬШИМИ РУЧКАМИ, ДЛЯ ТОГО ЧТОБЫ УДОБНО И
НАДЁЖНО ИХ УДЕРЖИВАТЬ;
ВО-ВТОРЫХ, ИНСТРУМЕНТЫ ДОЛЖНЫ БЫТЬ СКОНСТРУИРОВАНЫ С
РАСЧЁТОМ НА ТРЕМОР РУК ХИРУРГА, ЗНАЧИТЕЛЬНО НАРАСТАЮЩИЙ ПОД
УВЕЛИЧЕНИЕМ.
9.
MICROSURGICAL INSTRUMENTSMicrosurgical instruments differ from traditional instruments in a number of ways:
Firstly, they must be suitable for delicate manipulations on structures barely
visible to the naked eye. However, they must have large enough handles in order
to comfortably and securely hold them;
Secondly, the instruments must be designed for the surgeon's hand tremor, which
increases significantly with magnification.
10.
ВЫДЕЛЯЮТ 3 ГРУППЫ ИНСТРУМЕНТОВ1- ДЛЯ
РАЗЪЕДИНЕНИЯ
НОЖНИЦЫ, СКАЛЬПЕЛИ
И ЛЕЗВИЕДЕРЖАТЕЛИ
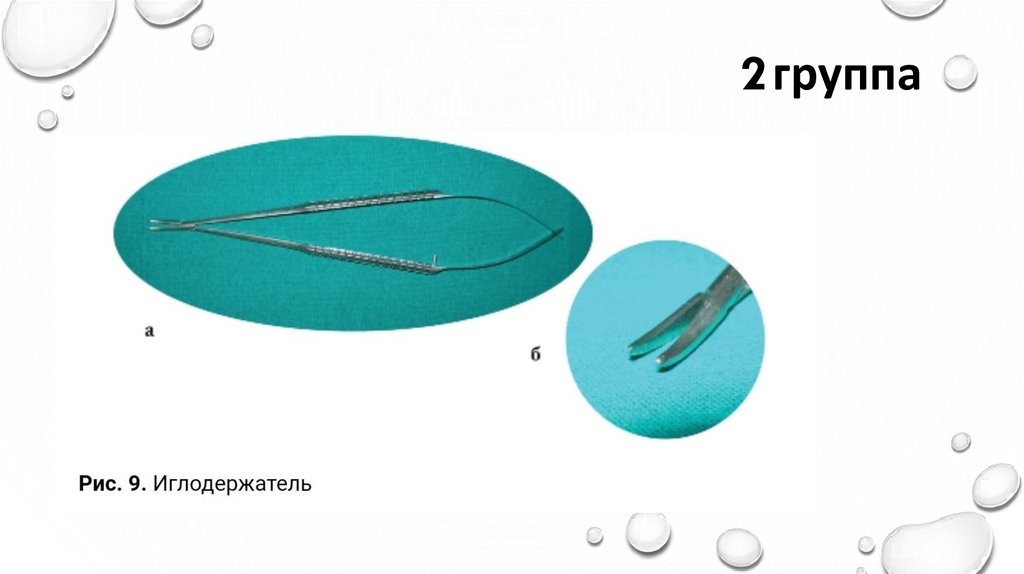
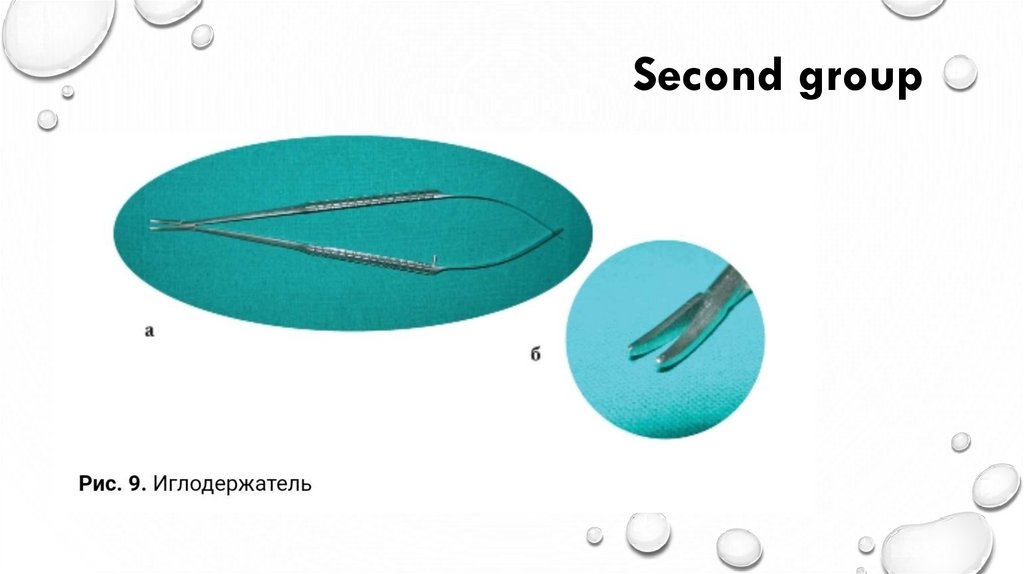
2- ДЛЯ
СОЕДИНЕНИЯ
ТКАНЕЙ
РАЗНООБРАЗНЫЕ
ИГЛОДЕРЖАТЕЛИ, А
ТАКЖЕ СПЕЦИАЛЬНЫЕ
ПРИСПОСОБЛЕНИЯ
ДЛЯ НАЛОЖЕНИЯ
МЕХАНИЧЕСКОЙ ШВА
3ВСПОМОГАТЕЛЬНЫЕ
ПИНЦЕТЫ, ДИЛАТАТОРЫ,
МИКРОКРЮЧКИ И
МИКРОВИЛКИ,
МИКРОИРРИГАТОРЫ,
МИКРООТСОСЫ,
СОСУДИСТЫЕ КЛИПСЫ,
АПРОКСИМАТОРЫ,
КЛИПСОДЕРЖАТЕЛИ.
11.
THERE ARE THREE GROUPS OF INSTRUMENTS1- To disconnect
2- For joining fabrics
3- Subsidiary
Scissors, scalpels and
blade holders
Various needle holders,
as well as special devices
for applying mechanical
seams
Forceps, dilators, micro
hooks and micro forks,
micro irrigators, micro
pumps, vascular clips,
approximators, clip
holders.
12.
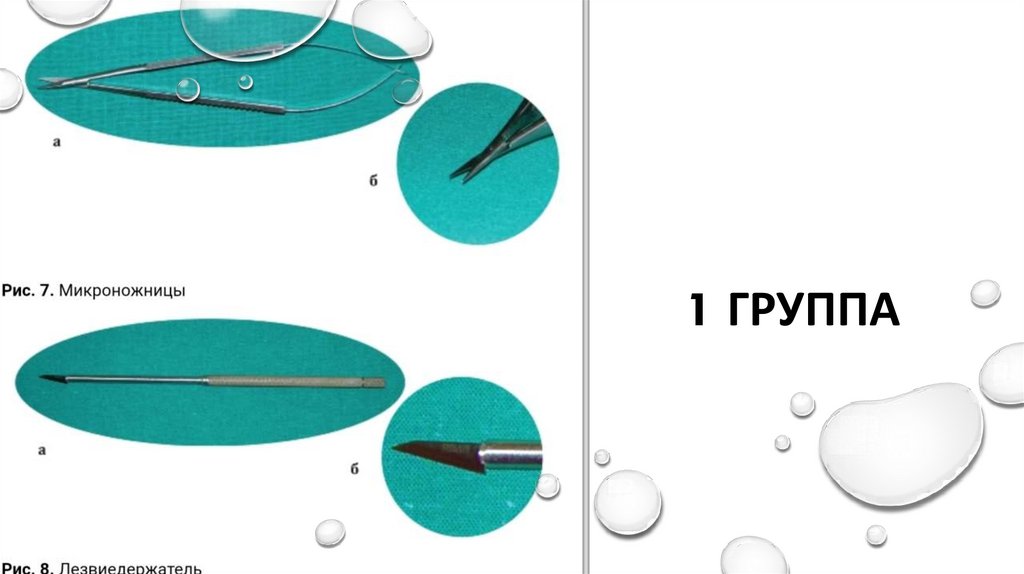
1 ГРУППА13.
First group14.
2 группа15.
Second group16.
3 группа17.
Third group18.
ИГЛЫ И ШОВНЫЙ МАТЕРИАЛ• ТРАДИЦИОННОЙ (ОБЩЕЙ) ХИРУРГИИ ДЛЯ
ДЕЛИКАТНЫХ МАНИПУЛЯЦИЙ ПРИМЕНЯЮТ
РАЗМЕРЫ ОТ 2-0 (3 ММ) ДО 6-0 (0,7 ММ).
• В МИКРОХИРУРГИИ ПРИМЕНЯЮТ НИТИ
ДИАМЕТРОМ ОТ 7-0, А ЧАЩЕ - ОТ 9-0 (0,4-0,3 ММ)
ДО 12-0 (МЕНЕЕ 0,1 ММ) (РИС. 23).
• ХИРУРГИЧЕСКИЕ НИТИ МОГУТ БЫТЬ
РАССАСЫВАЮЩИМИСЯ (РАЗРУШАЮТСЯ В
ОРГАНИЗМЕ ЧЕРЕЗ ОПРЕДЕЛЁННОЕ ВРЕМЯ) И
НЕРАССАСЫВАЮЩИМИСЯ (СОХРАНЯЮТ СВОЮ
ПРОЧНОСТЬ);
• ПРИРОДНЫМИ (ИЗ ШЁЛКА, СТЕНОК КИШЕЧНИКА
ЖИВОТНЫХ, ЛЬНА И ДРУГИХ ЕСТЕСТВЕННЫХ
МАТЕРИАЛОВ) И СИНТЕТИЧЕСКИМИ
(ПОЛИЭФИРНЫЕ, ПОЛИПРОПИЛЕНОВЫЕ НИТИ И
ДРУГИЕ ИСКУССТВЕННЫЕ МАТЕРИАЛЫ).
19.
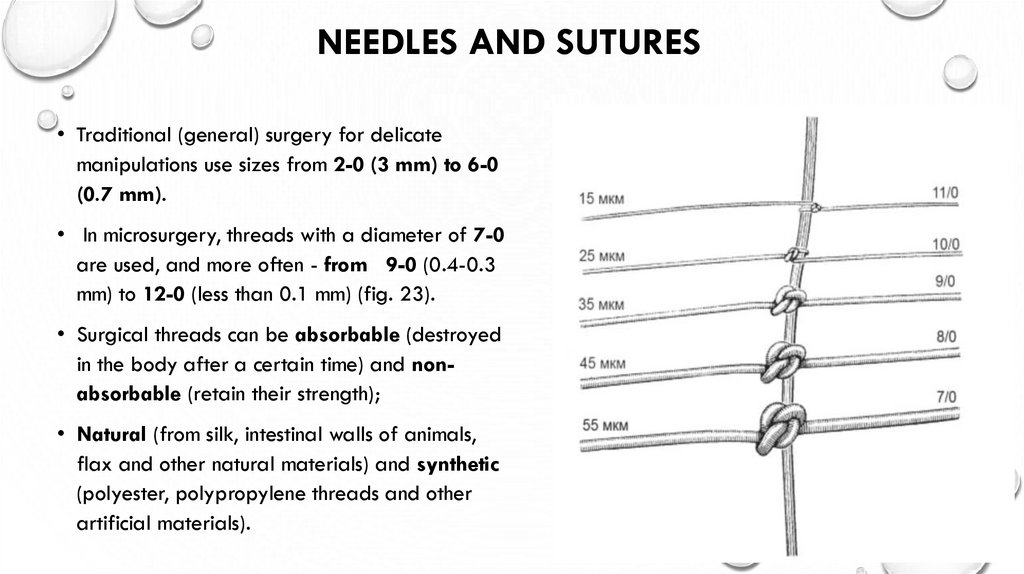
NEEDLES AND SUTURES• Traditional (general) surgery for delicate
manipulations use sizes from 2-0 (3 mm) to 6-0
(0.7 mm).
• In microsurgery, threads with a diameter of 7-0
are used, and more often - from 9-0 (0.4-0.3
mm) to 12-0 (less than 0.1 mm) (fig. 23).
• Surgical threads can be absorbable (destroyed
in the body after a certain time) and nonabsorbable (retain their strength);
• Natural (from silk, intestinal walls of animals,
flax and other natural materials) and synthetic
(polyester, polypropylene threads and other
artificial materials).
20.
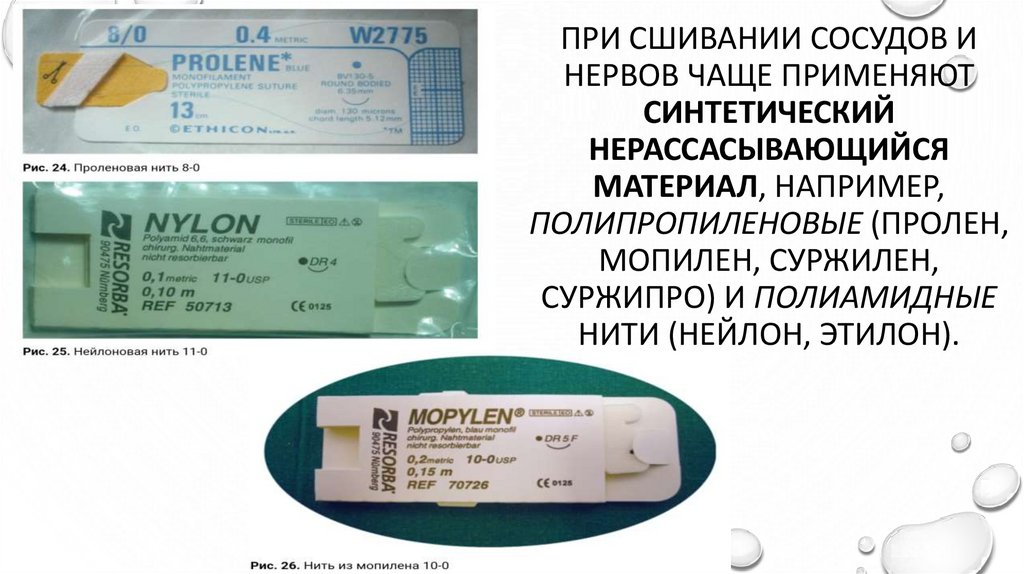
ПРИ СШИВАНИИ СОСУДОВ ИНЕРВОВ ЧАЩЕ ПРИМЕНЯЮТ
СИНТЕТИЧЕСКИЙ
НЕРАССАСЫВАЮЩИЙСЯ
МАТЕРИАЛ, НАПРИМЕР,
ПОЛИПРОПИЛЕНОВЫЕ (ПРОЛЕН,
МОПИЛЕН, СУРЖИЛЕН,
СУРЖИПРО) И ПОЛИАМИДНЫЕ
НИТИ (НЕЙЛОН, ЭТИЛОН).
21.
When suturing vessels and nerves,synthetic non-absorbable material
is often used, for example,
polypropylene (prolene, mopilen,
surzhilen, surzhipro) and
polyamide threads (nylon,
ethylone).
22.
• ХИРУРГИЧЕСКИЕ ИГЛЫ ВЫПУСКАЮТРАЗЛИЧНОГО РАЗМЕРА (ДИАМЕТРА И
ДЛИНЫ) И ФОРМЫ (ПРЯМЫЕ И
ИЗОГНУТЫЕ), А ТАКЖЕ С РАЗЛИЧНЫМ
ОСТРИЁМ (КОЛЮЩИЕ, РЕЖУЩИЕ И
ТУПЫЕ).
• В МИКРОХИРУРГИИ ПРИМЕНЯЮТ
ТОЛЬКО АТРАВМАТИЧЕСКИЕ ИГЛЫ,
КОТОРЫЕ ВЫПУСКАЮТ С ЗАЖАТОЙ
(ОБЖАТОЙ) С ОДНОГО КОНЦА
ХИРУРГИЧЕСКОЙ НИТЬЮ.
• ОТСУТСТВИЕ ДУПЛИКАТУРЫ НИТИ,
ВДЕТОЙ В УШКО ИГЛЫ, ЗНАЧИТЕЛЬНО
ОБЛЕГЧАЕТ ПРОХОЖДЕНИЕ
АТРАВМАТИЧЕСКОГО МАТЕРИАЛА
ЧЕРЕЗ ТКАНИ.
23.
• Surgical needles are available in differentsizes (diameter and length) and shapes
(straight and curved), as well as with
different points (piercing, cutting and
blunt).
• In microsurgery, only atraumatic needles
are used, which are attached to a clamped
(crimped) surgical thread from one end.
• The absence of duplication of the thread
threaded into needle greatly facilitates the
passage of atraumatic material through
the tissue.
24.
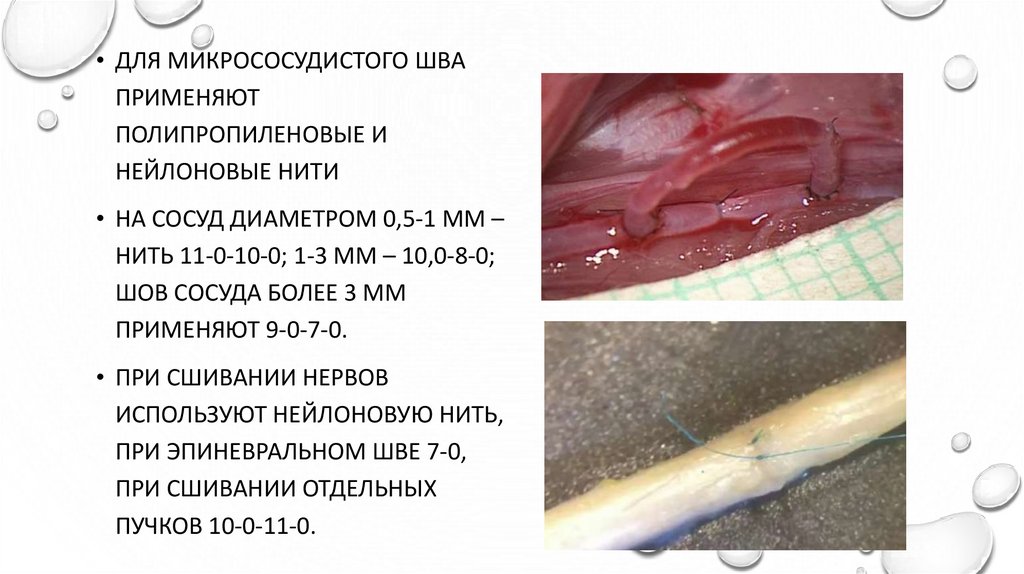
• ДЛЯ МИКРОСОСУДИСТОГО ШВАПРИМЕНЯЮТ
ПОЛИПРОПИЛЕНОВЫЕ И
НЕЙЛОНОВЫЕ НИТИ
• НА СОСУД ДИАМЕТРОМ 0,5-1 ММ –
НИТЬ 11-0-10-0; 1-3 ММ – 10,0-8-0;
ШОВ СОСУДА БОЛЕЕ 3 ММ
ПРИМЕНЯЮТ 9-0-7-0.
• ПРИ СШИВАНИИ НЕРВОВ
ИСПОЛЬЗУЮТ НЕЙЛОНОВУЮ НИТЬ,
ПРИ ЭПИНЕВРАЛЬНОМ ШВЕ 7-0,
ПРИ СШИВАНИИ ОТДЕЛЬНЫХ
ПУЧКОВ 10-0-11-0.
25.
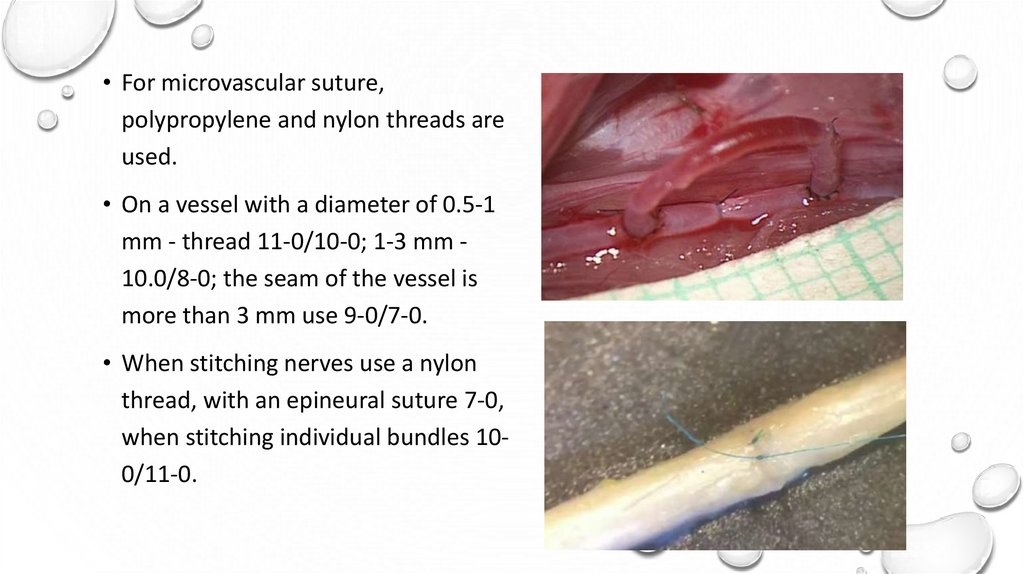
• For microvascular suture,polypropylene and nylon threads are
used.
• On a vessel with a diameter of 0.5-1
mm - thread 11-0/10-0; 1-3 mm 10.0/8-0; the seam of the vessel is
more than 3 mm use 9-0/7-0.
• When stitching nerves use a nylon
thread, with an epineural suture 7-0,
when stitching individual bundles 100/11-0.
26.
ОБЩИЕ ПРИНЦИПЫ
МИКРОХИРУРГИЧЕСКОЙ ТЕХНИКИ
МИКРОХИРУРГИЧЕСКАЯ ОПЕРАЦИЯ ПРЕДСТАВЛЯЕТ
СОБОЙ ДЛИТЕЛЬНУЮ НАПРЯЖЁННУЮ РАБОТУ В
ВЫНУЖДЕННОМ ПОЛОЖЕНИИ, ТРЕБУЮЩУЮ
МАКСИМАЛЬНОЙ ТОЧНОСТИ ДВИЖЕНИЙ.
• ДЛЯ УДОБСТВА ЗА ОПЕРАЦИОННЫМ СТОЛОМ БЫЛИ
РАЗРАБОТАНЫ СПЕЦИАЛЬНЫЕ КРЕСЛА С ВЫСОКОЙ
ПОДДЕРЖКОЙ ДЛЯ СПИНЫ И С ПОДЛОКОТНИКАМИ. В
КРЕСЛЕ ХИРУРГ НАХОДИТСЯ В ПОЗЕ «КУЧЕРА»,
РАСПОЛАГАЯ ПРЕДПЛЕЧЬЯ И ЗАПЯСТЬЯ НА
ПОДЛОКОТНИКАХ. ПОДЛОКОТНИКИ ПОЗВОЛЯЮТ
СНЯТЬ МЫШЕЧНОЕ НАПРЯЖЕНИЕ РУК ХИРУРГА И
УМЕНЬШИТЬ ТРЕМОР КИСТЕЙ И ПАЛЬЦЕВ.
27.
GENERAL PRINCIPLES OFMICROSURGICAL TECHNIQUE
• Microsurgical operation is a long-term strenuous
work in a forced position, requiring maximum
precision of movements. For the convenience of the
operating table, special chairs with high back
support and armrests have been developed. In the
chair, the surgeon is in the "coachman" position,
placing the forearms and wrists on the armrests.
The armrests relieve muscle tension in the surgeon's
arms and reduce hand and finger tremors.
28.
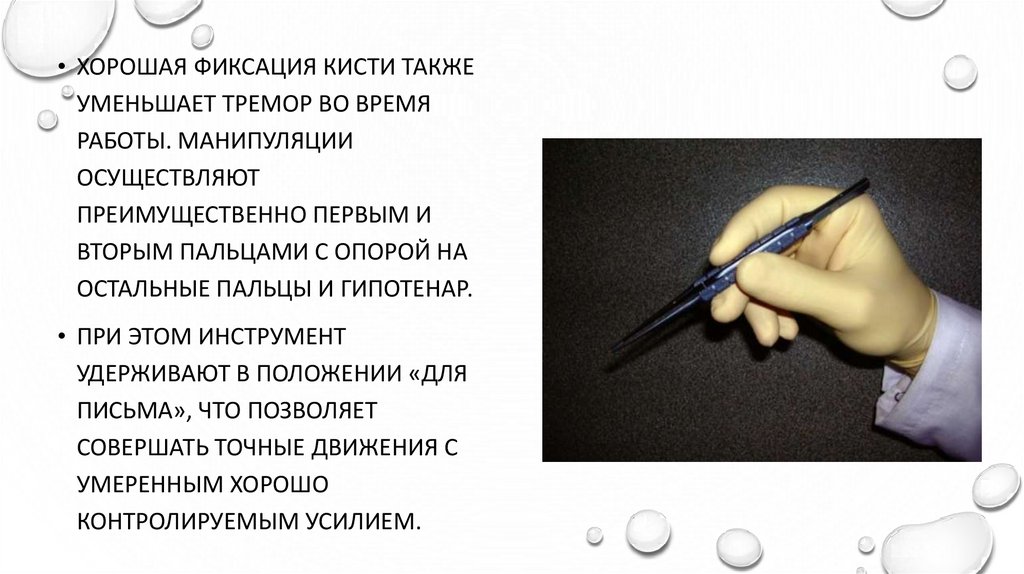
• ХОРОШАЯ ФИКСАЦИЯ КИСТИ ТАКЖЕУМЕНЬШАЕТ ТРЕМОР ВО ВРЕМЯ
РАБОТЫ. МАНИПУЛЯЦИИ
ОСУЩЕСТВЛЯЮТ
ПРЕИМУЩЕСТВЕННО ПЕРВЫМ И
ВТОРЫМ ПАЛЬЦАМИ С ОПОРОЙ НА
ОСТАЛЬНЫЕ ПАЛЬЦЫ И ГИПОТЕНАР.
• ПРИ ЭТОМ ИНСТРУМЕНТ
УДЕРЖИВАЮТ В ПОЛОЖЕНИИ «ДЛЯ
ПИСЬМА», ЧТО ПОЗВОЛЯЕТ
СОВЕРШАТЬ ТОЧНЫЕ ДВИЖЕНИЯ С
УМЕРЕННЫМ ХОРОШО
КОНТРОЛИРУЕМЫМ УСИЛИЕМ.
29.
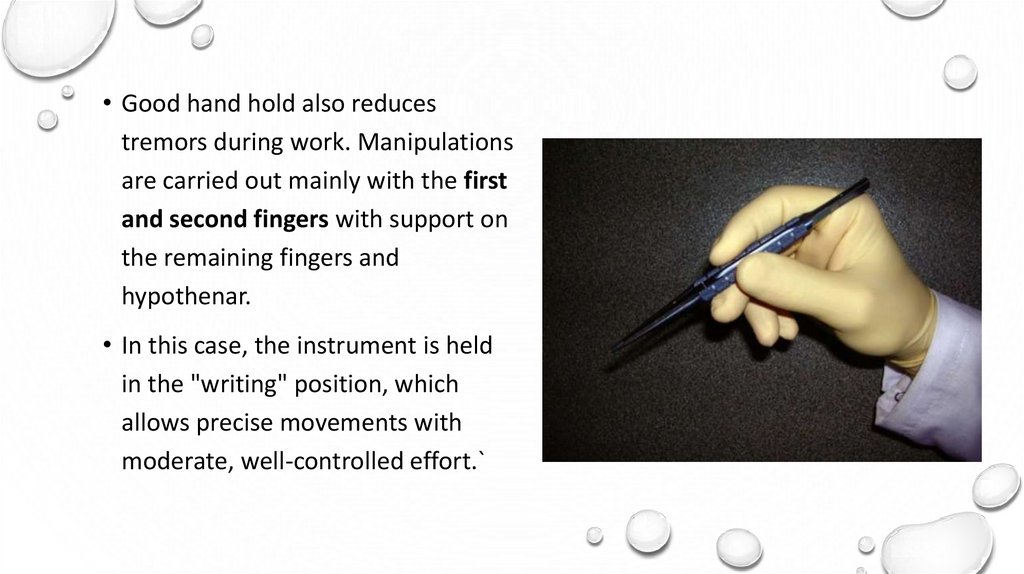
• Good hand hold also reducestremors during work. Manipulations
are carried out mainly with the first
and second fingers with support on
the remaining fingers and
hypothenar.
• In this case, the instrument is held
in the "writing" position, which
allows precise movements with
moderate, well-controlled effort.`
30.
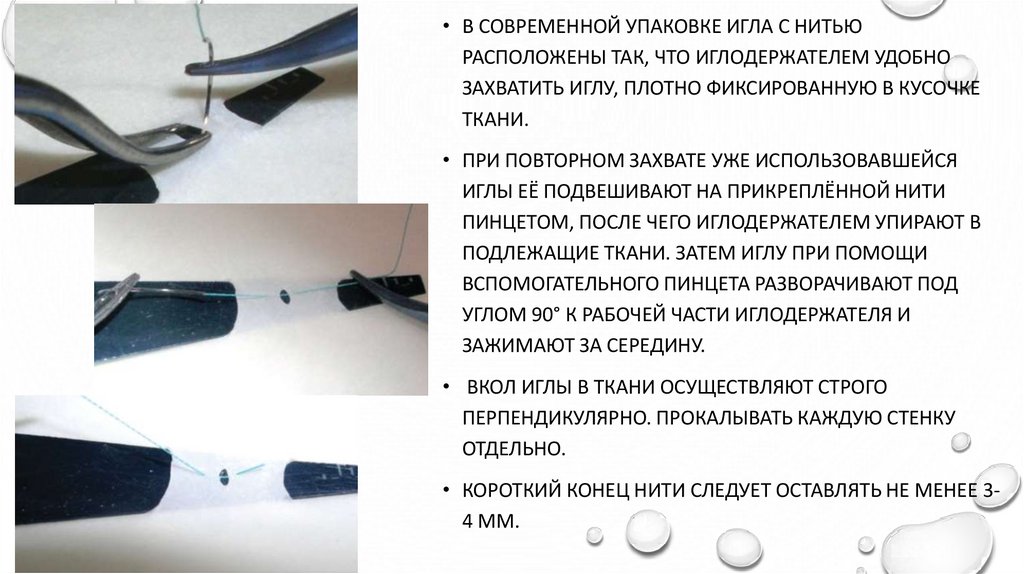
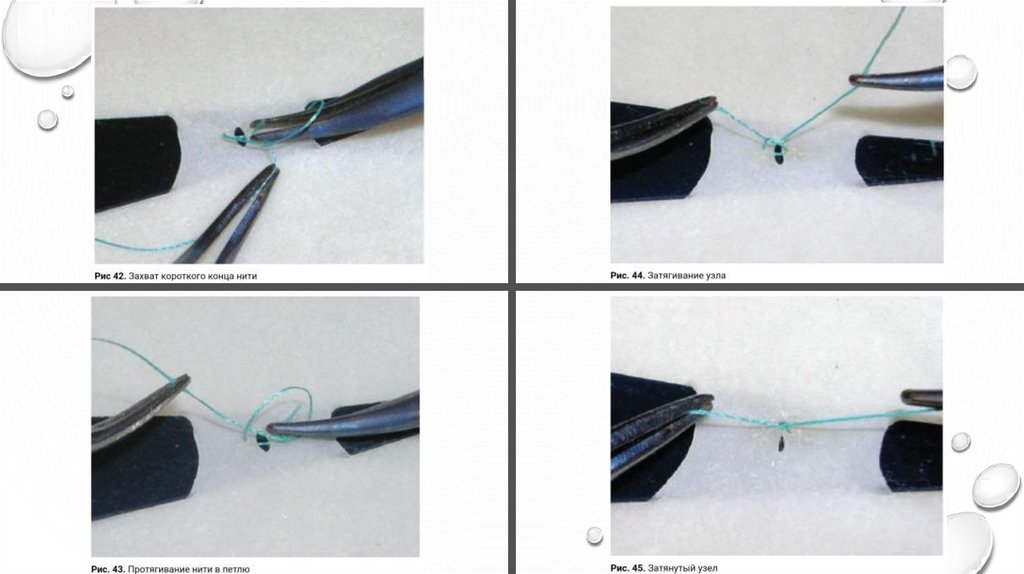
• В СОВРЕМЕННОЙ УПАКОВКЕ ИГЛА С НИТЬЮРАСПОЛОЖЕНЫ ТАК, ЧТО ИГЛОДЕРЖАТЕЛЕМ УДОБНО
ЗАХВАТИТЬ ИГЛУ, ПЛОТНО ФИКСИРОВАННУЮ В КУСОЧКЕ
ТКАНИ.
• ПРИ ПОВТОРНОМ ЗАХВАТЕ УЖЕ ИСПОЛЬЗОВАВШЕЙСЯ
ИГЛЫ ЕЁ ПОДВЕШИВАЮТ НА ПРИКРЕПЛЁННОЙ НИТИ
ПИНЦЕТОМ, ПОСЛЕ ЧЕГО ИГЛОДЕРЖАТЕЛЕМ УПИРАЮТ В
ПОДЛЕЖАЩИЕ ТКАНИ. ЗАТЕМ ИГЛУ ПРИ ПОМОЩИ
ВСПОМОГАТЕЛЬНОГО ПИНЦЕТА РАЗВОРАЧИВАЮТ ПОД
УГЛОМ 90° К РАБОЧЕЙ ЧАСТИ ИГЛОДЕРЖАТЕЛЯ И
ЗАЖИМАЮТ ЗА СЕРЕДИНУ.
• ВКОЛ ИГЛЫ В ТКАНИ ОСУЩЕСТВЛЯЮТ СТРОГО
ПЕРПЕНДИКУЛЯРНО. ПРОКАЛЫВАТЬ КАЖДУЮ СТЕНКУ
ОТДЕЛЬНО.
• КОРОТКИЙ КОНЕЦ НИТИ СЛЕДУЕТ ОСТАВЛЯТЬ НЕ МЕНЕЕ 34 ММ.
31.
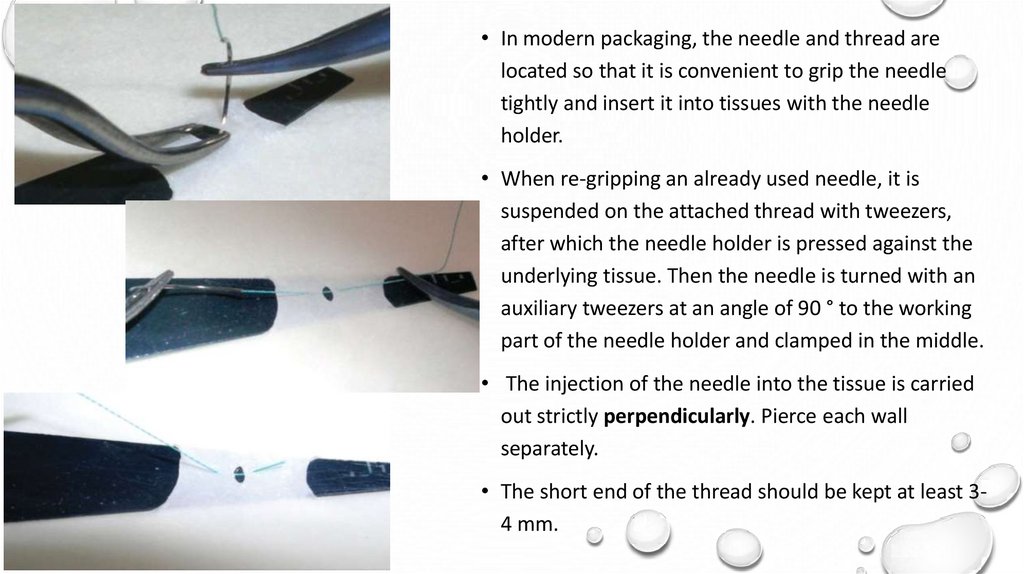
• In modern packaging, the needle and thread arelocated so that it is convenient to grip the needle
tightly and insert it into tissues with the needle
holder.
• When re-gripping an already used needle, it is
suspended on the attached thread with tweezers,
after which the needle holder is pressed against the
underlying tissue. Then the needle is turned with an
auxiliary tweezers at an angle of 90 ° to the working
part of the needle holder and clamped in the middle.
• The injection of the needle into the tissue is carried
out strictly perpendicularly. Pierce each wall
separately.
• The short end of the thread should be kept at least 34 mm.
32.
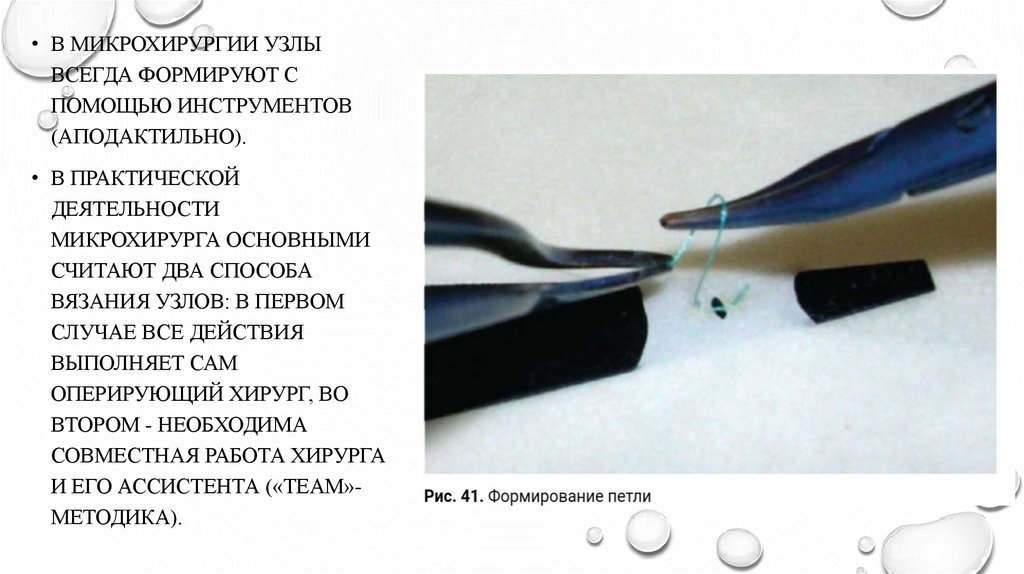
• В МИКРОХИРУРГИИ УЗЛЫВСЕГДА ФОРМИРУЮТ С
ПОМОЩЬЮ ИНСТРУМЕНТОВ
(АПОДАКТИЛЬНО).
• В ПРАКТИЧЕСКОЙ
ДЕЯТЕЛЬНОСТИ
МИКРОХИРУРГА ОСНОВНЫМИ
СЧИТАЮТ ДВА СПОСОБА
ВЯЗАНИЯ УЗЛОВ: В ПЕРВОМ
СЛУЧАЕ ВСЕ ДЕЙСТВИЯ
ВЫПОЛНЯЕТ САМ
ОПЕРИРУЮЩИЙ ХИРУРГ, ВО
ВТОРОМ - НЕОБХОДИМА
СОВМЕСТНАЯ РАБОТА ХИРУРГА
И ЕГО АССИСТЕНТА («TEAM»МЕТОДИКА).
33.
• IN MICROSURGERY nodes arealways formed with the help of tools
(apodactically).
• In the practical activities of a
microsurgeon, two methods of knitting
are considered to be the main ones: in
the first case, all actions are performed
by the operating surgeon himself, in the
second, the joint work of the surgeon
and his assistant is necessary (“team”
method).
34.
35.
МИКРОСОСУДИСТЫЙ ШОВ.• СОСУДИСТЫЙ АНАСТОМОЗ ПРЕДСТАВЛЯЕТ СОБОЙ СОЕДИНЕНИЕ ДВУХ
КОНЦОВ СОСУДА ИЛИ ДВУХ ОТДЕЛЬНЫХ СОСУДОВ С ФОРМИРОВАНИЕМ
НЕПРЕРЫВНОГО КАНАЛА. АНАСТОМОЗЫ ПОДРАЗДЕЛЯЮТСЯ НА ТИПЫ:
• «КОНЕЦ-В-КОНЕЦ» (МЕЖДУ ДВУМЯ РАССЕЧЁННЫМИ КОНЦАМИ
СОСУДА/ОВ),
• «КОНЕЦ-В-БОК» (СОЕДИНЕНИЕ ОДНОГО КОНЦА КРОВЕНОСНОГО СОСУДА
СО СТЕНКОЙ ДРУГОГО) И
• «БОК-В-БОК» (МЕЖДУ СТЕНКАМИ ДВУХ СОСУДОВ).
36.
MICROVASCULAR SUTURE.• Vascular anastomosis is the connection of two ends of a vessel or
two separate vessels to form a continuous channel.
Anastomoses are divided into types:
"End-to-end" (between the two dissected ends of the vessel / s),
End-to-side (connecting one end of a blood vessel to the wall of the
other) and
"side-to-side" (between the walls of two vessels).
37.
ОСОБЕННОСТИ РАБОТЫВЕНА
• - СТЕНКА ЗНАЧИТЕЛЬНО ТОНЬШЕ, ХРУПКАЯ
АРТЕРИЯ
• - СКОРОСТЬ ТОКА КРОВИ МЕДЛЕННАЯ
• - СТЕНКА ТОЛЩЕ, ВЫРАЖЕННЫЙ
МЫШЕЧНЫЙ СЛОЙ
• - НАЛИЧИЕ КЛАПАНОВ
• - СКОРОСТЬ ТОКА КРОВИ ВЫШЕ
• - БОЛЕЕ ПЛОТНАЯ ФИКСАЦИЯ
ПЕРИАДВЕНТИЦИАЛЬНЫХ ТКАНЕЙ К ВЕНЕ, ЧЕМ
К АРТЕРИИ
• - ОТСУТСТВИЕ КЛАПАНОВ
• - ЦЕЛЕСООБРАЗНО НАКЛАДЫВАТЬ
НЕПРЕРЫВНЫЙ ШОВ, ЧЕМ УЗЛОВОЙ
• - НАКЛАДЫВАЮТ УЗЛОВЫЕ ШВЫ
38.
FEATURES OF WORKARTERY
VEIN
• The wall is thicker, pronounced muscle
layer
• The wall is much thinner, fragile
• The blood flow rate is higher
• The presence of valves
• lack of valves
• Tighter fixation of periaventic tissues to the
vein than to the artery
• interrupted sutures are applied
• the blood flow rate is slow
• It is advisable to apply a continuous suture
than a nodal
39.
ВЫДЕЛЕНИЕ СОСУДОВ• АРТЕРИЯ И ВЕНА ЛЕЖАТ В ЕДИНОМ ПУЧКЕ, ПЕРЕД ВЫДЕЛЕНИЕМ
ФУТЛЯР ПОДВЕШИВАЮТ ИЛИ СМЕЩАЮТ ПИНЦЕТОМ,
РАССЕКАЮТ НА НЕБОЛЬШОМ УЧАСТКЕ.
• В ОБРАЗОВАВШЕЕ ОТВЕРСТИЕ, ПАРАЛЛЕЛЬНО СОСУДАМ ВВОДЯТ
БРАНШУ МИКРОНОЖНИЦ И РАССЕКАЮТ.
• СОСУДЫ МОБИЛИЗИРУЮТ, МЕЛКИЕ ВЕТВИ КОАГУЛИРУЮТ
• РАССЕЧЕНИЕ В ОКОЛОСОСУДИСТОЙ ЗОНЕ СТРОГО ПАРАЛЛЕЛЬНО
СОСУДИСТОЙ СТЕНКЕ.
40.
ISOLATION OF VESSELS• The artery and vein lie in a single bundle, before isolation, it is
separated with tweezers, dissected in a small area.
• A branch of microscissors is inserted into the hole formed, parallel to
the vessels, and dissected.
• Vessels are mobilized, and small branches are coagulated.
• Dissection in the perivascular zone is strictly parallel to the vascular
wall.
41.
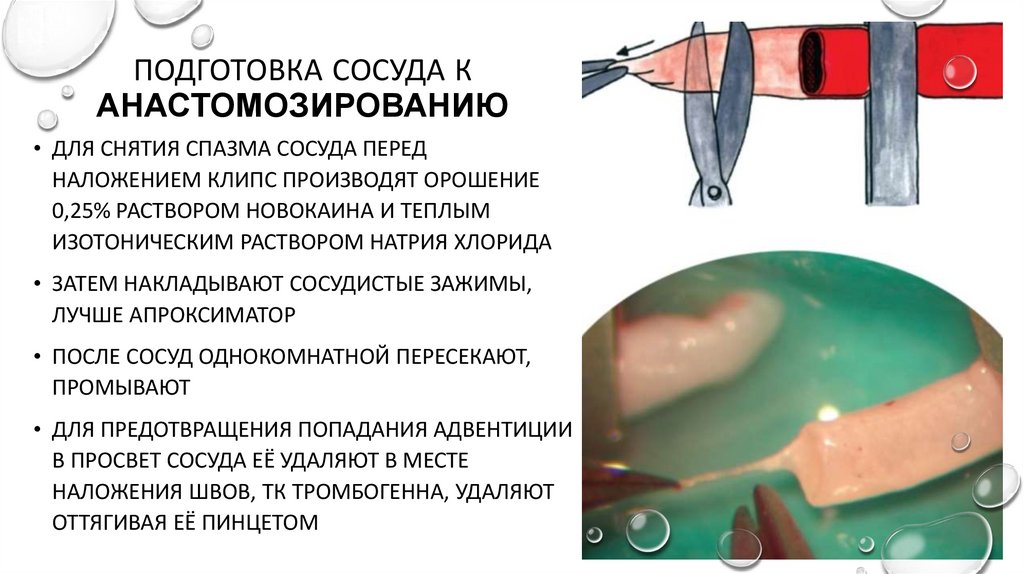
ПОДГОТОВКА СОСУДА КАНАСТОМОЗИРОВАНИЮ
• ДЛЯ СНЯТИЯ СПАЗМА СОСУДА ПЕРЕД
НАЛОЖЕНИЕМ КЛИПС ПРОИЗВОДЯТ ОРОШЕНИЕ
0,25% РАСТВОРОМ НОВОКАИНА И ТЕПЛЫМ
ИЗОТОНИЧЕСКИМ РАСТВОРОМ НАТРИЯ ХЛОРИДА
• ЗАТЕМ НАКЛАДЫВАЮТ СОСУДИСТЫЕ ЗАЖИМЫ,
ЛУЧШЕ АПРОКСИМАТОР
• ПОСЛЕ СОСУД ОДНОКОМНАТНОЙ ПЕРЕСЕКАЮТ,
ПРОМЫВАЮТ
• ДЛЯ ПРЕДОТВРАЩЕНИЯ ПОПАДАНИЯ АДВЕНТИЦИИ
В ПРОСВЕТ СОСУДА ЕЁ УДАЛЯЮТ В МЕСТЕ
НАЛОЖЕНИЯ ШВОВ, ТК ТРОМБОГЕННА, УДАЛЯЮТ
ОТТЯГИВАЯ ЕЁ ПИНЦЕТОМ
42.
PREPARING A VESSEL FORANASTOMOSIS
• To relieve the spasm of the vessel, before applying
the clips, irrigation is performed with a 0.25%
solution of novocaine and a warm isotonic solution
of sodium chloride
• Then vascular clamps are applied, preferably an
approximator
• The vessel is washed after being cut
• To prevent the ingress of adventitia into the lumen
of the vessel, it is removed at the suture site, since
it is thrombogenic, it is removed by pulling it off
with tweezers
43.
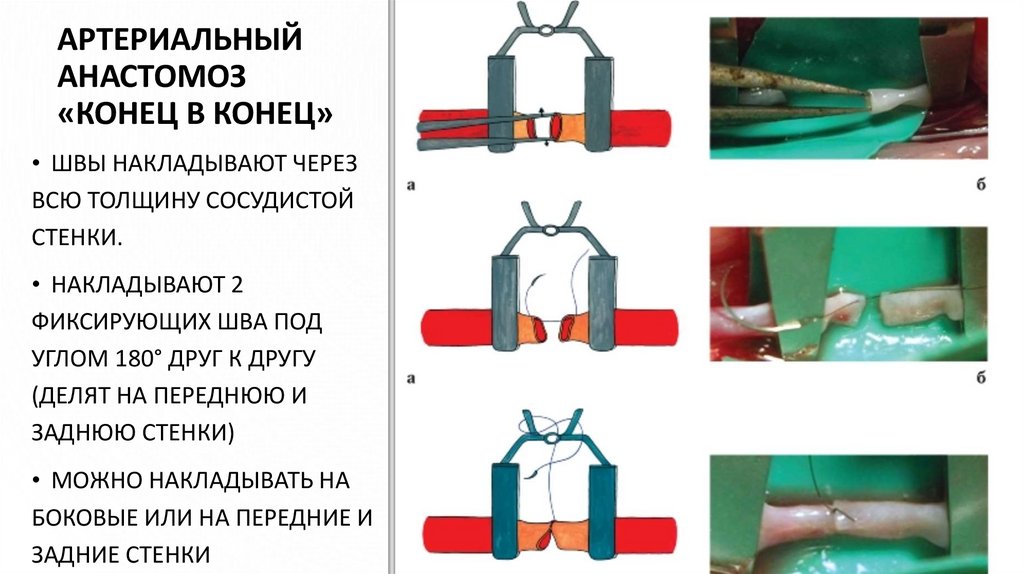
АРТЕРИАЛЬНЫЙАНАСТОМОЗ
«КОНЕЦ В КОНЕЦ»
• ШВЫ НАКЛАДЫВАЮТ ЧЕРЕЗ
ВСЮ ТОЛЩИНУ СОСУДИСТОЙ
СТЕНКИ.
• НАКЛАДЫВАЮТ 2
ФИКСИРУЮЩИХ ШВА ПОД
УГЛОМ 180° ДРУГ К ДРУГУ
(ДЕЛЯТ НА ПЕРЕДНЮЮ И
ЗАДНЮЮ СТЕНКИ)
• МОЖНО НАКЛАДЫВАТЬ НА
БОКОВЫЕ ИЛИ НА ПЕРЕДНИЕ И
ЗАДНИЕ СТЕНКИ
44.
END-TO-ENDARTERIAL
ANASTOMOSIS
• Sutures are applied through
the entire thickness of the
vascular wall.
• Apply 2 fixing seams at an
angle of 180 ° to each other
(divided into front and back
walls)
• Can be applied to side or
front and back walls
45.
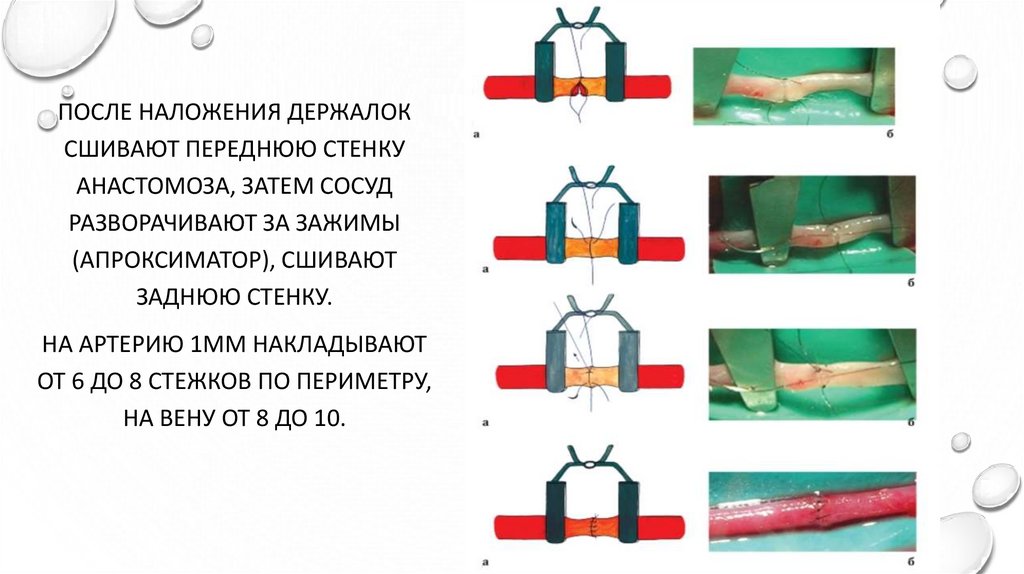
ПОСЛЕ НАЛОЖЕНИЯ ДЕРЖАЛОКСШИВАЮТ ПЕРЕДНЮЮ СТЕНКУ
АНАСТОМОЗА, ЗАТЕМ СОСУД
РАЗВОРАЧИВАЮТ ЗА ЗАЖИМЫ
(АПРОКСИМАТОР), СШИВАЮТ
ЗАДНЮЮ СТЕНКУ.
НА АРТЕРИЮ 1ММ НАКЛАДЫВАЮТ
ОТ 6 ДО 8 СТЕЖКОВ ПО ПЕРИМЕТРУ,
НА ВЕНУ ОТ 8 ДО 10.
46.
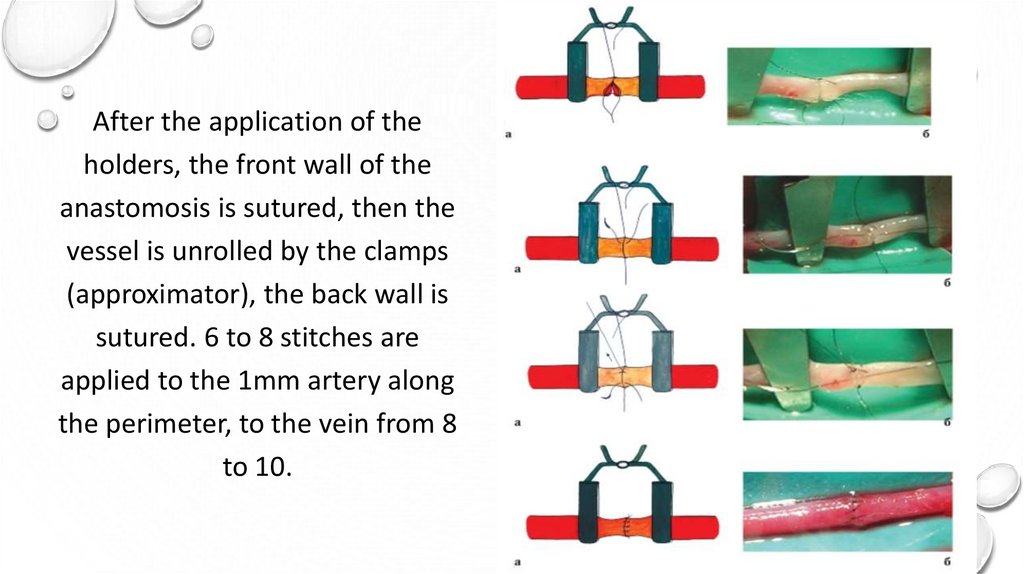
After the application of theholders, the front wall of the
anastomosis is sutured, then the
vessel is unrolled by the clamps
(approximator), the back wall is
sutured. 6 to 8 stitches are
applied to the 1mm artery along
the perimeter, to the vein from 8
to 10.
47.
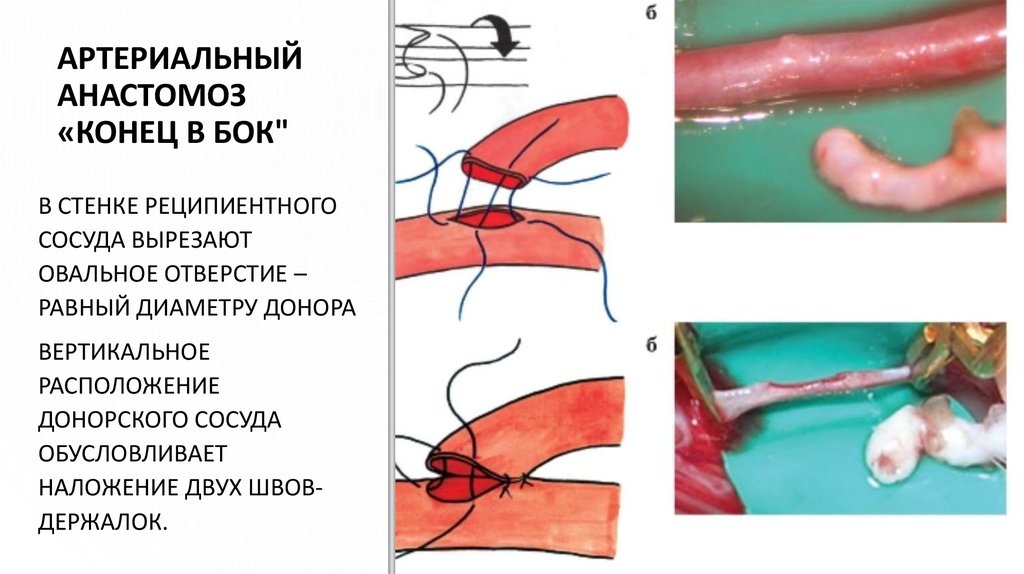
АРТЕРИАЛЬНЫЙАНАСТОМОЗ
«КОНЕЦ В БОК"
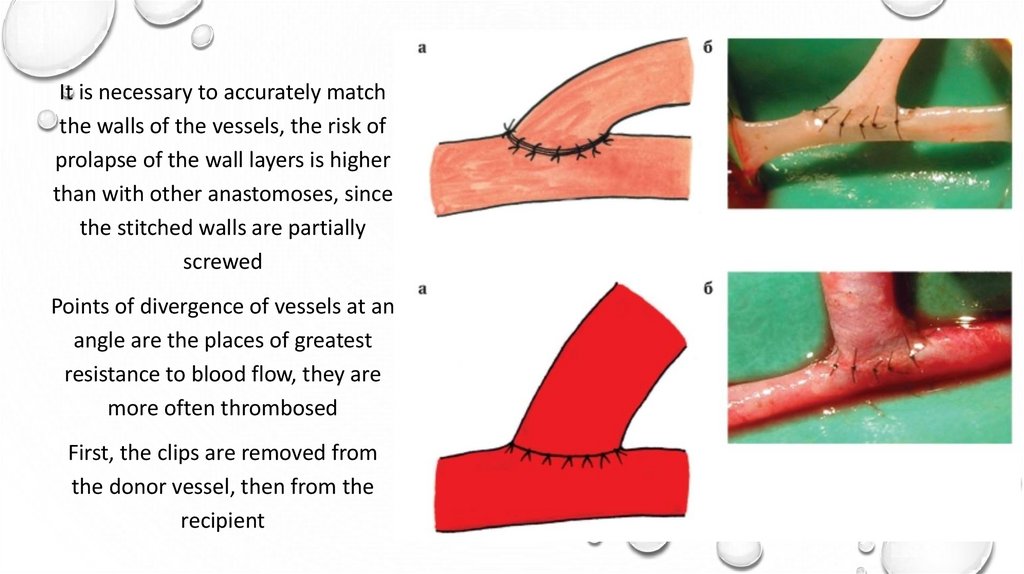
В СТЕНКЕ РЕЦИПИЕНТНОГО
СОСУДА ВЫРЕЗАЮТ
ОВАЛЬНОЕ ОТВЕРСТИЕ –
РАВНЫЙ ДИАМЕТРУ ДОНОРА
ВЕРТИКАЛЬНОЕ
РАСПОЛОЖЕНИЕ
ДОНОРСКОГО СОСУДА
ОБУСЛОВЛИВАЕТ
НАЛОЖЕНИЕ ДВУХ ШВОВДЕРЖАЛОК.
48.
END-TO-SIDEARTERIAL
ANASTOMOSIS
• An oval hole is cut in
the wall of the recipient
vessel - equal to the
donor diameter. The
vertical position of the
donor vessel leads to
the imposition of two
retainer sutures.
49.
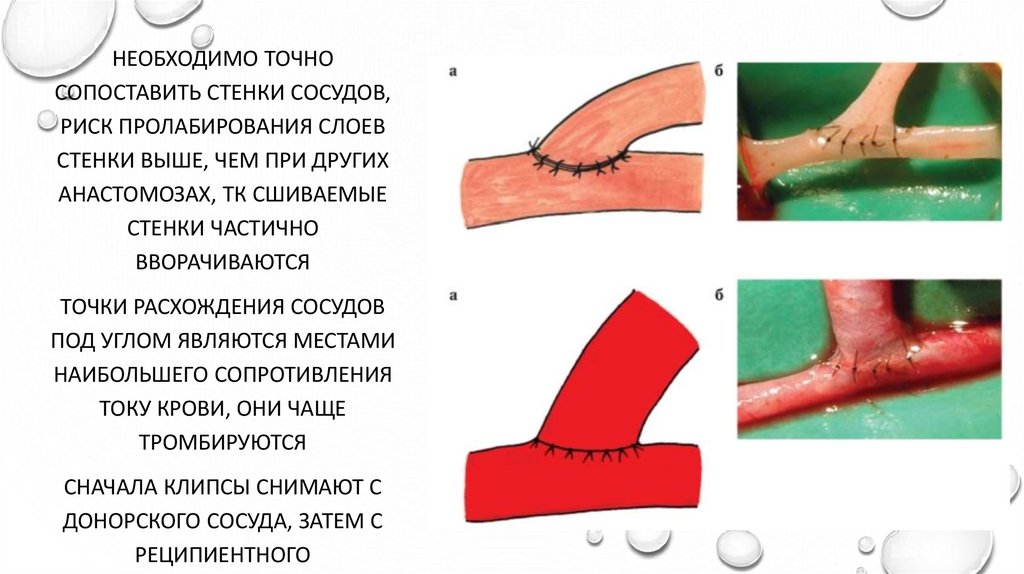
НЕОБХОДИМО ТОЧНОСОПОСТАВИТЬ СТЕНКИ СОСУДОВ,
РИСК ПРОЛАБИРОВАНИЯ СЛОЕВ
СТЕНКИ ВЫШЕ, ЧЕМ ПРИ ДРУГИХ
АНАСТОМОЗАХ, ТК СШИВАЕМЫЕ
СТЕНКИ ЧАСТИЧНО
ВВОРАЧИВАЮТСЯ
ТОЧКИ РАСХОЖДЕНИЯ СОСУДОВ
ПОД УГЛОМ ЯВЛЯЮТСЯ МЕСТАМИ
НАИБОЛЬШЕГО СОПРОТИВЛЕНИЯ
ТОКУ КРОВИ, ОНИ ЧАЩЕ
ТРОМБИРУЮТСЯ
СНАЧАЛА КЛИПСЫ СНИМАЮТ С
ДОНОРСКОГО СОСУДА, ЗАТЕМ С
РЕЦИПИЕНТНОГО
50.
It is necessary to accurately matchthe walls of the vessels, the risk of
prolapse of the wall layers is higher
than with other anastomoses, since
the stitched walls are partially
screwed
Points of divergence of vessels at an
angle are the places of greatest
resistance to blood flow, they are
more often thrombosed
First, the clips are removed from
the donor vessel, then from the
recipient
51.
СОСУДИСТЫЙАНАСТОМОЗ
«БОК В БОК"
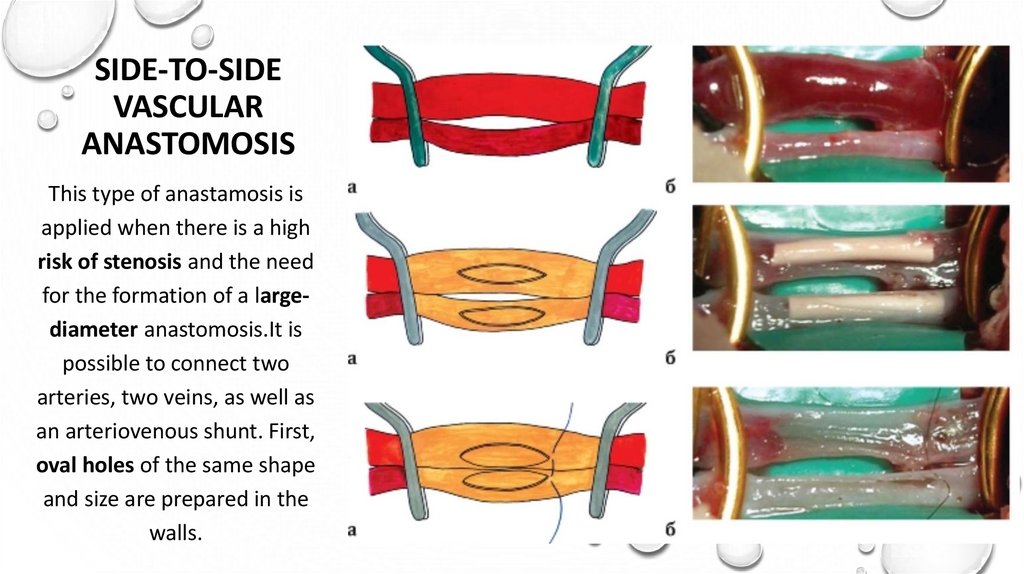
ДАННЫЙ ТИП АНАСТОМОЗА
НАКЛАДЫВАЮТ ПРИ ВЫСОКОМ
РИСКЕ СТЕНОЗИРОВАНИЯ И
НЕОБХОДИМОСТИ ОБРАЗОВАНИЯ
СОУСТЬЯ БОЛЬШОГО ДИАМЕТРА
ВОЗМОЖНО СОЕДИНЕНИЕ ДВУХ
АРТЕРИЙ, ДВУХ ВЕН, А ТАКЖЕ
АРТЕРИОВЕНОЗНОГО ШУНТА
ВНАЧАЛЕ В СТЕНКАХ
ПОДГОТАВЛИВАЮТ ОВАЛЬНЫЕ
ОТВЕРСТИЯ ОДИНАКОВОЙ
ФОРМЫ И РАЗМЕРА
52.
SIDE-TO-SIDEVASCULAR
ANASTOMOSIS
This type of anastamosis is
applied when there is a high
risk of stenosis and the need
for the formation of a largediameter anastomosis.It is
possible to connect two
arteries, two veins, as well as
an arteriovenous shunt. First,
oval holes of the same shape
and size are prepared in the
walls.
53.
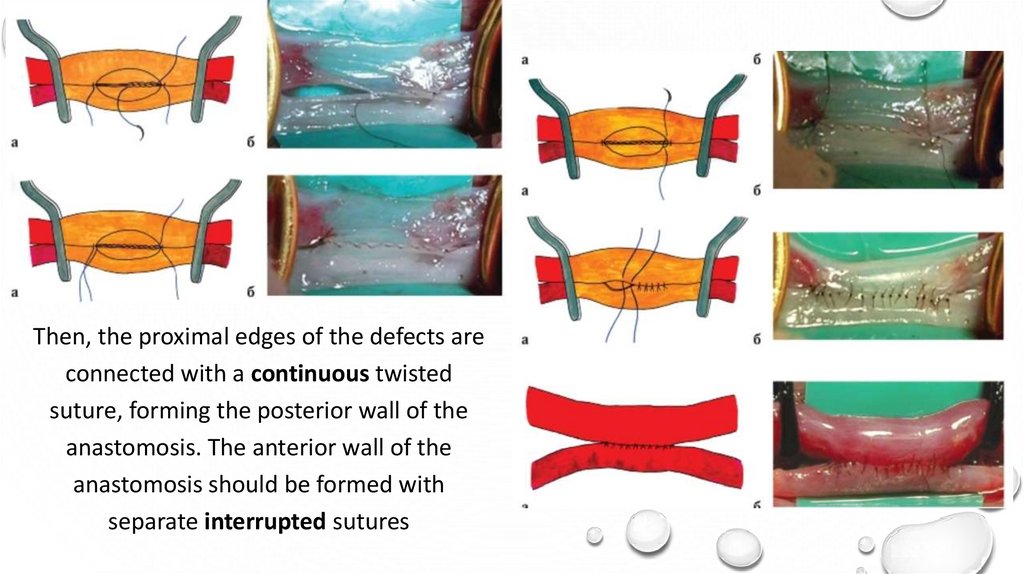
ЗАТЕМ НЕПРЕРЫВНЫМ ОБВИВНЫМШВОМ СОЕДИНЯЮТ БЛИЖНИЕ КРАЯ
ДЕФЕКТОВ, ФОРМИРУЯ ЗАДНЮЮ
СТЕНКУ АНАСТОМОЗА
ПЕРЕДНЮЮ СТЕНКУ АНАСТОМОЗА
СЛЕДУЕТ ФОРМИРОВАТЬ
ОТДЕЛЬНЫМИ УЗЛОВЫМИ ШВАМИ
54.
Then, the proximal edges of the defects areconnected with a continuous twisted
suture, forming the posterior wall of the
anastomosis. The anterior wall of the
anastomosis should be formed with
separate interrupted sutures
55.
ВЕНОЗНЫЙ АНАСТОМОЗ «КОНЕЦ ВКОНЕЦ»
ВЕНОЗНЫЙ АНАСТОМОЗ
«КОНЕЦ В БОК»
ТАКОЙ ВАРИАНТ РЕДКО
ПРИМЕНЯЕТСЯ, ТЕХНИКА
ТАКАЯ КАК ПРИ
АРТЕРИАЛЬНОМ
ТЕХНИКА СХОДНА С АРТЕРИАЛЬНЫМ,
НЕОБХОДИМО СТРОГО
ПЕРПЕНДИКУЛЯРНО ПРОКАЛЫВАТЬ
СТЕНКУ, НАКЛАДЫВАЮТ 3 ШВЫДЕРЖАЛКИ ПОД УГЛОМ 120°,
ЦЕЛЕСООБРАЗНО НАКЛАДЫВАТЬ
НЕПРЕРЫВНЫЙ ШОВ
56.
END-TO-END VENOUS ANASTOMOSISEND-TO-SIDE VENOUS
ANASTOMOSIS
This option is rarely used, a
technique such as for arterial
The technique is like the arterial one, it is
necessary to pierce the wall strictly
perpendicularly, apply 3 stitch sutures at
an angle of 120 °, it is advisable to apply
a continuous suture
57.
ВИДЕОМАТЕРИАЛМИКРОСОСУДИСТЫЙ
ШОВ
• HTTPS://YOUTU.BE/U2B8GIX8FNQ
• HTTPS://YOUTU.BE/SEKY_AWLQ_G
• HTTPS://YOUTU.BE/QNOITMBFYO8
VIDEO FOOTAGE OF
MICROVASCULAR
SUTURE
58.
https://aliexpress.ru/item/32920033300.html?spm=a2g0s.11045068.rcmd404.5.35f856a4LASz03&pvid=0541c4bc-f9384b4a-be75-8356bc0e607e&gpsid=detail404&scm=1007.16891.96945.0&scmurl=1007.16891.96945.0&scm_id=1007.16891.96945.0
https://aliexpress.ru/item/10000010316086.html?srcSns=sns_V
K&spreadType=socialShare&bizType=ProductDetail&social_par
ams=40100112601&aff_fcid=8779609251584bc293e33a7d
578183a0-1633379598579-03266_982crQ&tt=MG&aff_fsk=_982crQ&aff_platform=default&sk
=_982crQ&aff_trace_key=8779609251584bc293e33a7d578
183a0-1633379598579-03266_982crQ&shareId=40100112601&businessType=ProductDetail
&platform=AE&terminal_id=0361000c9375425eba54ed1ee7
cae7c1