
















 medicine
medicineSimilar presentations:






")



Diphtheria
1.
DIPHTHERIAIdentification – acute anthroponosis infectious disease
caused by the toxicogenic strains Corynobacterium
diphteriae, which is characterized by an inflammation in a
place of invasion with derivation of a fibrinous film and
toxic lesion both of cardiovascular and nervous systems.
Diphthera (greek) – means “membrane”
Historical reference:
1828 - the French doctor Bretanno in detail had described
the clinical forms of disease also had given to its
the name "«diphtherit".
1846 - Trusso А. had detected signs diphtheria as
infectious disease also had called to its the modern
name "diphtheria"
2.
1883 - Кlebs E.Т.- revealed of the infectious agent indiphtheritic film and has described its
1884 - Loffler Е. revealed of the infectious agent in pure
culture also has described its cultural of properties
1888 - Roux Е.P.P., Yersin А.E., Behrling E.А. selected
exotoxin in the pure state also received an antitoxin
(beginning of specific therapy diphtheria)
1923 - Glen and Ramon G. received an anatoxin
(beginning mass immnization against diphtheria)
3.
ETIOLOGYCorynobabacterium diphteriae (C.d.) Gram (+), thin rods
with rounded, widening ends which contein in them of a
clump of grains of a volutin.
C.d. have size from 1- 12 microns of length and to 0.3- 0.8
microns of width. Spores and capsules no have, but on a
surface have fimbrias, facilitating by them an adhesion.
Facultical anaerobes.
Optimum temperature for cultivation is 37 d. С.
They are polymorphic and on cultural and enzymatic
properties are divided into 3 biotypes:
GRAVIS, INTERMEDIUS, MITIS.
Are steady against low temperatures.
C.d. have survived in water, milk from 1 to 3 weeks at
room temperature ( 25 d. С. )
Desinfectants have inactivated С.d by 1 - 2 minutes
C.d. were destroyed immediatly at boiling.
4. C.d. - divided "«flicks" and consequently in growing culture 25 – 30% its allocate at angles to each other, probebly as a
C.d. - divided "«flicks" and consequently in growing culture 25 – 30% itsallocate at angles to each other, probebly as a result of incomplete
separation at the moment of division
5.
Ability to excrete toxin have only lysogenic strains С.d.infectious by a phage having a gene- tox which encodes
structure of a toxin
Any biotype can produce exotoxin, but generically most
often- gravis, the least - mitis. Excess iron in plasma
strengthens produce of toxin!!
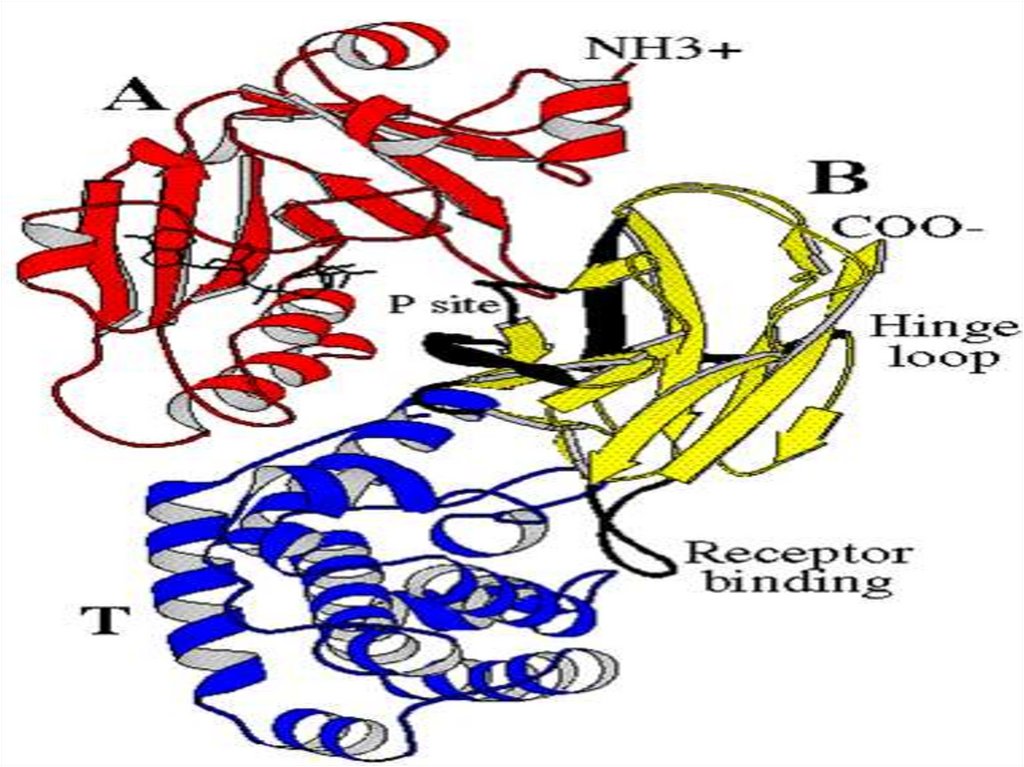
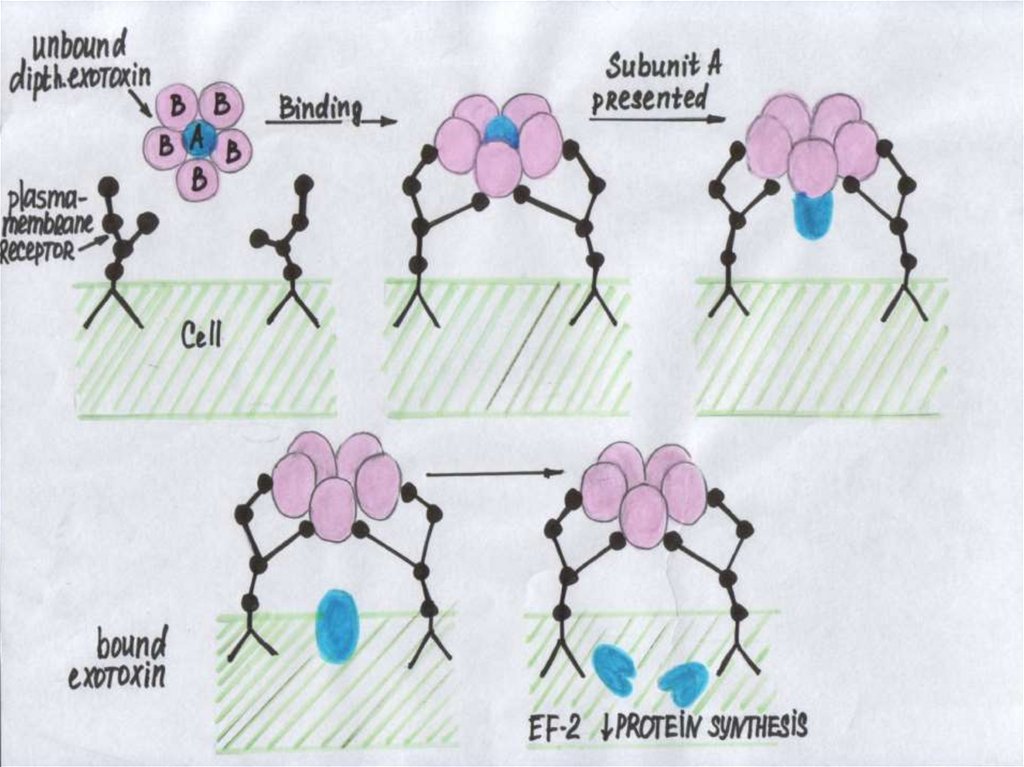
Exotoxin С.d. (polypeptide) consists of:
- a fraction A (purely toxin)
- and fraction B (recognizes cell - targets and fixes a
fraction A on its (adhesion).
The toxin in a cell inhibits the factor ELONGATION- 2 transferase responsible for grafting of a polypeptide chain
on ribosomes, that results in stopping of albuminous
synthesis in a cell and subsequent step-by-step
destruction its.
6.
7.
8. Mode of action of the diphtheria toxin.
Mode of action of the diphtheria toxin.
9. Virulence intradermal tests in rabbit. Two days after inoculation a few positive reactions are shown on a rabbit`s skin but
most are negative10.
Facilitates infiltration and strengthens action of a toxin:hyaluronidase,
neuraminidase,
fibrinolysinum,
hemolysin,
necrotic and hydropic factors etc.
Toxin in a free state to a blood circulates 10 minutes and 30
- 40 minutes are on a surface of cell-targets.
After infiltration into a cell - antitoxin doesn`t neutralize
toxin
On force of action С.d. toxin borrows the 3th places among
biological poisons!!! (after a botulismus and tetanus)
11.
EPIDEMIOLOGYSources of an infection:
Epidemiological
danger
The sick
Convalescent
Bacteriocarrying
low
moderate
high
Danger
infection
high
moderate
low
Sanitation of convalescents are completed through 15 - 20
days , but about 90 days can be delayed.
The frequency of a carriage in a population makes 1-10 %
12.
Modes of transmission:- aerogenic mode
- contact and alimentary mode ( rare )
Enlargement of a case rate - in autumn-winter period
Periodicity of uprise of a case rate – 5 - 7 years.
Controlled infection.
The scheduled vaccination in children's age have given
increase of diseases among the adult now!!!
13.
PATHOGENY1. In a place of invasion (mucous or the skin) is marked
Intensive reproduction С.d. by production exotoxin,
that is accompanied by a hyperemia, edema, venous
stasis with intensifying of permeability of the shallow
blood vessels of submucous or hypodermic
2. Exit of fibrinogenum from capillaries, touch with
by thromboplastin of demaged cells mucous and
transformation in a fibrin, which densely retains fibrinous
membrane on a surface mucous. A thickening and
spreading of a membrane carry on doing up to 5 - 6 days
of illness!!!
14.
3. С.d. remain under membrane, but exotoxin will penetratein regional lymph nodi (lymphadenitis), hypodermic
fat (edema of a hypodermic fat) and blood with
by fixing it on cell - targets and subsequent them
by toxico-allergic injure :
- Heart - myocardium and carrying out system
- Nervous system - demyelination of nervous fibers
(both of paresis or paralyses and damage peripheral
sympathetic of ganglions)
- Adrenal glands- hemorrhage in them, necrosis of a tissue
- Kidneys - signs of a nephrosis
15. The organ- targets for diphtheria.
16.
4. Cord - factor С.d., breaking respiratory processes incells, plays particular role in a pathogeny diphtheria
5. The changes in the struck organs are converted and
disappear in periods from 4- 5 weeks up to the 6 of
months
6. After convalescence is shaped as antitoxical and antibacterial immunity, but not for life. The disease can
repeat !
17.
THE CLASSIFICATION DIPHTHERIA takes into account:1. Localization of the process:
- diphtheria of a stomatopharynx A 36.0
- diphtheria of a nasopharynx
A 36.1
- diphtheria of a larynx
A 36.2
- diphtheria of a skin
A 36.3
- diphtheria another localization
A 36 8
- diphtheria hypothetical
A 36.9
18.
2. Spreading of the process:- Localized
- Wide-spread
- Combined
3 Degree of
gravity:
- Mild
- Middle-severe
- Severe
- Hypertoxical
4. Character of a local inflammation:
- catarral
- insular ( «island»)
- membraneous
5. Complication of diphtheria (TIS. myocarditis, neuritis ets.)
Example of the diagnosis: Diphtheria of a stomatopharynx,
membraneous, middle-severe gravity (С.д. gravis, tox +)
early myocarditis
19.
CLINIC DIPHTHERIA( incubation is from 2 to 10 days )
Carriage С.d. is shaped after:
- the transferred disease (convalescent)
- or for the healthy persons ( 1 - 10 % in a population ).
The clinical manifestations have no. Antibody against С.d.
in a blood is not formed.
Proves to be true only bacteriological detection in smears
С.d.!
Carriage С.d. may be:
- Short-term
- about 2 weeks
- Average duration - 2 - 4 weeks
- Lingering
- more than 4 weeks
- Chronic
- more than 6 months
20.
the SUBCLINICAL FORM of DIPHTHERIAThe complaints for the patient are not present:
- hyperemia and inappreciable edema of tonsils and
mucous stomatopharynx is (rare).
- diagnosis bacteriological- detection С.д. in smears and
appearance of antibodies against С.д. in a blood.
- Can be revealed by late complications from the side
the cardiovascular system (myocarditis)
21.
DIPHTHERIA of TONSILS and PHARYNXThe mild form of disease:
- moderate weakness at a normal hemodynamics, normal or
subfebrile temperature of a body inappreciable pharyngalgia.
- hyperemia and edema of tonsils and mucous pharynx
- presence on tonsils of shallow films or small solid film
- increase and moderate morbidity at a palpation
submandibular lymph nodes
- to clinical signs by the doctors of common practice
diagnoses as a tonsillitis, pharyngitis , ARVD
22.
The middle-severe form diphtheria of a stomatopharynx:- acute beginning, fever up to 38 - 38,5 гр.C, weakness
- pain in muscles and joints, headache, thirst, lowering
appetites, paleness of skin, sometimes cyanotic
- moderate pharyngalgia at a swallowing
- edema of tonsils and mucous stomatopharynx, detection
fibrinous film with predilection to distribution (sometimes
combined form)
- increase and painful submandibular lymph nodes
- an edema of a hypodermic fat of a neck (up to a clavicle)
Relative tachycardia, predilection to a hypotonia and
to lowering BP, systolic murmur on an apex of the heart
It`s complicated by a myocarditis, by a mononeuritis (is
more often paresis of the soft palate)
23.
24.
25. an edema of the hypodermic fat
26. an edema of the hypodermic fat
27.
The severe form diphtheria of a stomatopharynx:- acute beginning and high fever, strong headache, myalgia
and arthralgia, vomiting, alarming dream
- the pharyngalgia (can be strong), but the patients are more
often feel a lump in a throat and labored respiration
- paleness of a skin in a combination with cyanosis
dull cardiac sounds, tachycardia, then - bradycardia
(poor sign)
- dyspnea at an inappreciable exercise stress
- increase and painful submandibular lymph nodes,
- the edema of a hypodermic fat of a neck (is lower than a
clavicle)
28.
- fibrinous film on tonsils with an exit for them limits (widespread or combined the form diphtheria)- then dyspnea in period of calm , paradoxic the type of
respiration (paresis of muscles of a diaphragm) lowering
BP, bradycardia, intensifying of a hypoxia ( heart failure
and congestion of a blood in lungs)
- appearance of a hemorrhagic syndrome
- damage of kidneys with development acute renal
unsufficiency
-development of polyneurites by end first week with
violation impellent and touch functions and serious
myocarditis
29.
THE HYPERTOXICAL FORM DIPHTHERIA:- arises at infection massive dose С.д. having
excessive toxic-production by possibilities
- starts as the severe form diphtheria, but toxicosis always
prevails above by local inflammatory manifestations
- fast development TIS and DIC more often results to
death of the patient on the 2 - 3 days from a beginning
of illness
- Fibrinous film on a surface mucous not has time to be
generated!!!
- The diagnosis more often is installed postmortal on the
fact detections С.д. with bacteriological methods!!!
30.
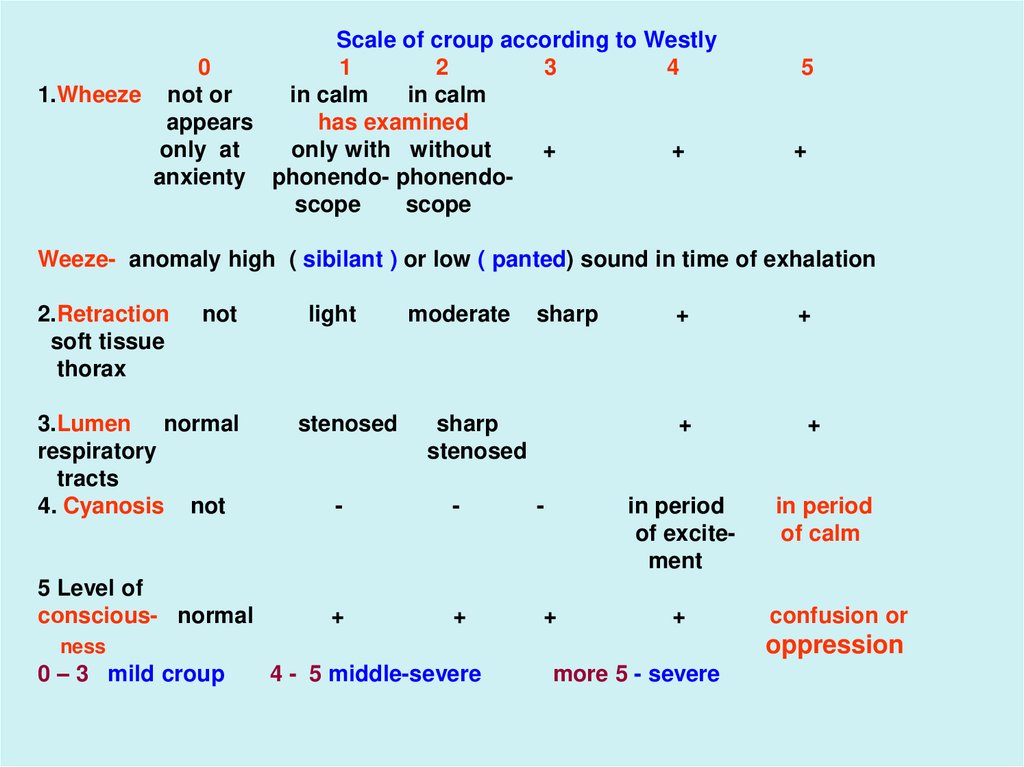
Scale of croup according to Westly0
1
2
3
4
1.Wheeze not or
in calm
in calm
appears
has examined
only at
only with without
+
+
anxienty phonendo- phonendoscope
scope
5
+
Weeze- anomaly high ( sibilant ) or low ( panted) sound in time of exhalation
2.Retraction
soft tissue
thorax
not
3.Lumen normal
respiratory
tracts
4. Cyanosis not
5 Level of
cоnscious- normal
light
stenosed
moderate
sharp
sharp
stenosed
+
+
-
-
-
in period
of excitement
+
+
+
+
+
in period
of calm
confusion or
oppression
ness
0 – 3 mild croup
+
4 - 5 middle-severe
more 5 - severe
31.
DIPHTHERIA of a LARYNX And TRACHEA:Toxic of manifestation minimum and HYPOXIA - carrying on
syndrome at this form of disease because of violation of
permeability of upper respiratory paths down to a croup,
which in the development passes 3 stages:
Catarrhal: (duration of a stage 1 - 2 days)
- complaints to weekness, malaise, subfebrile temperature
- onset of cough with a sputum, which fast is replaced on
"barked"
- hoarse of a voice is saved and outside of attacks of
cough
- at laringoscopy - hyperemia and edema of mucous larynx,
vocal cords, trachea (the films on mucous still are not
present!!)
32.
laringostenosis:(iS MORE OFTEN ON 2 - 3 DAY of ILLNESS - duration of this stage - 2 - 3 days)
- appearance of laboured and noisy respiration
- retraction at an inspiration supraclavicular and intercostal
intervals
- aphonia and silent cough
- the patients are restless, are frightened, occupy
forced a position in bed leaning on hands
- the tachycardia, tachypnea, is reduced BP, dull of
cardiac sounds, occurs cyanosis of a skin and mucous
- at laryngoscopy - edema, hyperemia with cyanosis and
croupous of a film frequently on a major extent
33.
34. forced a position in bed
35.
36.
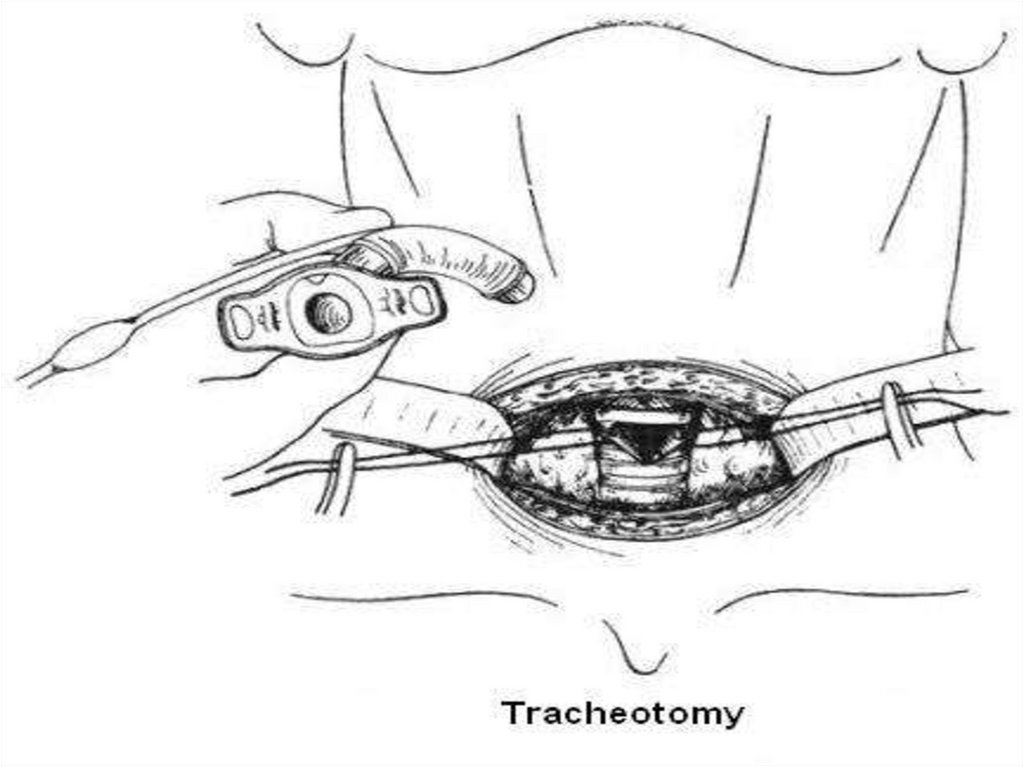
•Asphyxia (duration about 8 minutes!!)- fast intensifying of respiratory unsufficiency
- frequent, surface, noisy, respiratory arrhythmia
on a background total cyanosis, forced position
- loss of the forced position, confusion and then
loss of consciousness, cramps and death (without
immediate tracheostomies!!)
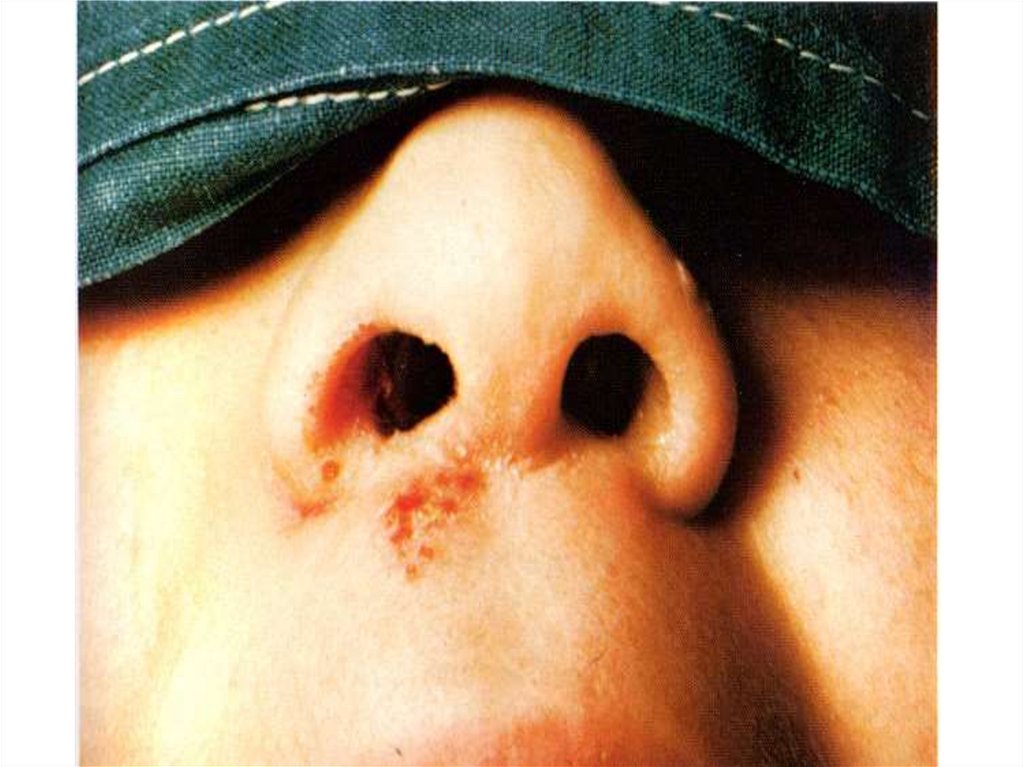
DIPHTHERIA of a NOSE:
- can be localized and wide-spread.
- rhinoscopy signs - edema and hyperemia mucous
or presence of films on it
- the intoxication is always expressed unsignificantly
- it is always stuffiness of the nose with serous or
by serous-hemorrhagic secretion from it with fragments of
films in them.
37.
- edema the eye`s orbit of a hypodermic fat (at transition ofthe process in maxilary sinus of a nose)
- rhinoscopy and positive bacteriological test allow to
install the exact diagnosis
- late complications at this form of disease rare.
DIPHTHERIA of OTHER LOCALIZATION
(eyes, skin, the sexual organs etc.) - are almost always
secondary and the gravity of current is stipulated an
expressiveness primary the center.
Diagnose visually (injure of a skin or mucous with
presence of a fibrinous film on it ) and bacteriologycal
(detection in them С.д.)
38.
39.
COMPLICATIONS - toxico-infectious shock, DIC, myocardites(early and late), neuritis (early and late), toxic nephrosonephritis, hepatitis (only at the serious forms), activation by
secondary bacterial flora, asphyxia with a film etc.
LABORATORY DIAGNOSTICS:
- microscopy smears from under a film - Gram(+) bacteria
- inoculaition of the smears of medium taking from under a
film three times before assignment antibiotics!
- definition of quantity antibodies in a blood before
introduction of an antitoxin and after 7-10 days PHA test
( increase titer not less than in 4 times-is positive) etc.
- toxin in a blood reveals - PCR
- WBC - moderate neutrocytosis with toxic granularity,
acceleration ESR, lowering of eosinocytes
40.
- UA- leucocytes, erythrocytes, cylinders, high RDU( of protein up to 10 g\l.)
- the biochemical tests - АSТ, LDG, ABC, electrolytes
blood, coagulogram, renal and hepatic enzymes
- at initial all - ECG, medical consultations of the
neurologist, the cardiologist and the otolaringologist
DIFFERENTIAL DIAGNOSTICS:
1.Diphtheria of a stomatopharynx:
- Streptococcal and staphylococcal angina
- Angina Vensana
- Infectious mononucleosis
- Scarlet fever
- Paratonsillitis infiltrate or аbscess
- Candidiasis of a stomatopharynx
41. Streptococcal and staphylococcal angina
42. Angina Vensana
43. The infectious agent of angina Vensana
44. Infectious mononucleosis
45. Infectious mononucleosis
46. Candidiasis of a stomatopharynx
47.
- Angina Ludviga- Аnginal-bubonic form of a tularemia
- Secondary angina at a typhoid, lues, tuberculosis, neoplasm, leukosis, agranulocytosis, combustions of a
mucous stomatopharynx (acid and alkali)
2. Diphtheria a nasopharyngitis:
- Meningococcal nasopharyngitis
- Streptococcal pharyngitis
- Adenoviral pharyngitis
3 At diphtheria of a larynx:
- False croup (ARVD. parainfluenza, measles etc.)
- Asphyxia by a foreign body
- Streptococcal pharyngitis (severe)
48.
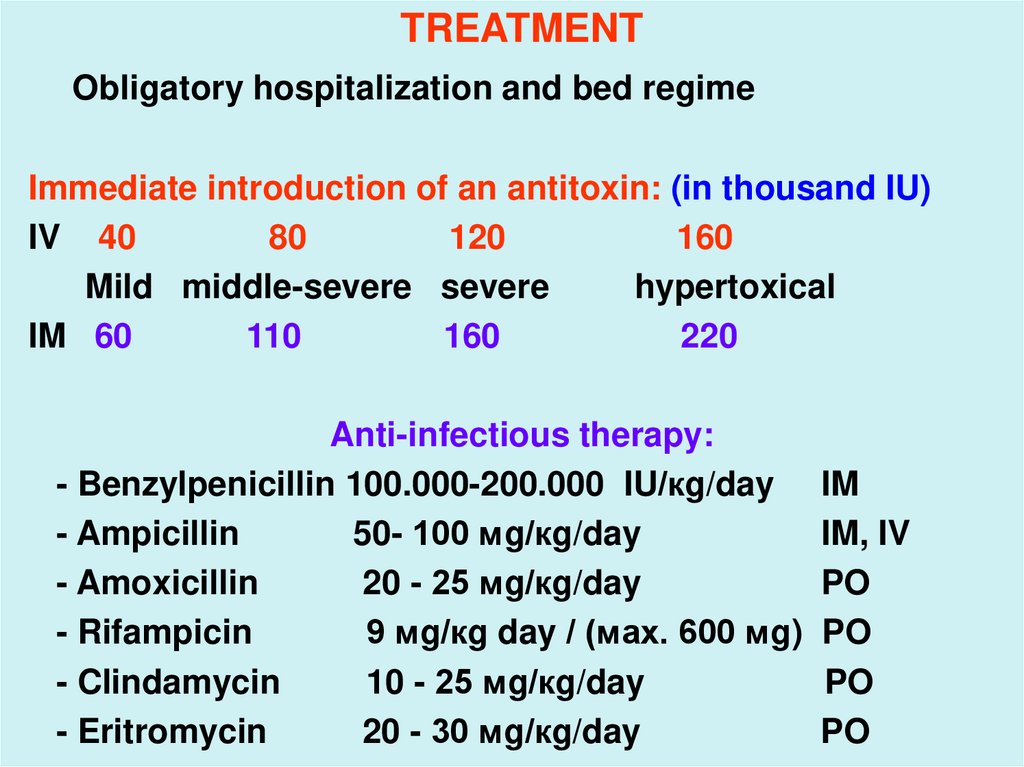
TREATMENTObligatory hospitalization and bed regime
Immediate introduction of an antitoxin: (in thousand IU)
IV 40
80
120
160
Mild middle-severe severe
hypertoxical
IM 60
110
160
220
Anti-infectious therapy:
- Benzylpenicillin 100.000-200.000 IU/кg/day
- Ampicillin
50- 100 мg/кg/day
- Amoxicillin
20 - 25 мg/кg/day
- Rifampicin
9 мg/кg day / (мах. 600 мg)
- Clindamycin
10 - 25 мg/кg/day
- Eritromycin
20 - 30 мg/кg/day
IM
IM, IV
PO
PO
PO
PO
49.
-MAINTENANCE THERAPY
desintocation and sufficient hydration
inhibitors of proteases
antioxidants.
diuretics
glucocorticoids
nonsteroids antiinflammatory drugs
antihistamine drugs
treatment of myocardites, neuritises etc.
PROPHYLAXIS (common and special)
- Common: inspection of the contact persons,
- Closing disinfection in the center,
- Installation in the center of quarantine for 7 days
50.
Special:- introductions of a diphtherial anatoxin.- primary immunization on the 3,4,5 th months of life
- revaccination per 18 months, and then in 6, 11, 14, 18
years
- the adult population is subject to a revaccination
everyone 10 years