
















 medicine
medicineSimilar presentations:



")






Modes of ventilation
1.
Modes of VentilationDr. Eugenia Mahamid
Rambam Medical Center
1
2.
Modes of VentilationThe main indication for ventilatory support
is
Respiratory Failure
2
3.
Categories of Respiratory FailureHYPOXEMIC
ARDS
PULMONARY EDEMA
PULMONARY HEMORRHAGE
PNEUMONIA
Low compliance lung disease:
Low PO2, Low SaO2
3
4.
Categories of Respiratory FailureHYPERCARBIC
OBSTRUCTION TO AIRFLOW
NEUROMUSCULAR DISORDERS
DRUG OVERDOSE
ENDOCRINOPATHIES
Increase in PCO2
Respiratory acidosis
Decrease in pH
4
5.
Categories of Respiratory FailureE
CENTRAL
C
• DECREASED LEVEL OF
E CONSCIOUSNESS
ACUTE MEDICAL AND SURGICAL
CONDITIONS
• MECHANICAL VENTILATION IS USED TO
DECREASE WORK OF BREATHING
5
6.
A MECHANICAL VENTILATOR isa pump providing an external source of energy to push
gases into the lungs and allow for passive exhalation
(CO2 elimination).
Ventilator’s Changeable parameters
Vt
= Tidal Volume
FIO2
= Fraction of Inspired Oxygen
RR
= Respiratory Rate
I:E
= Inspiratory to Expiratory ratio
EEP
= End Expiratory Pressure
PIP
= Peak Inspiratory Pressure
Inspiratory Flow Rate
6
7.
OTHER MEANS AFFECTING VENTILATION• NO = Nitric Oxide
• Orientation of patient’s body in gravitational field
7
8.
GENERAL CLASSES OF VENTILATORSNegative pressure
application of negative pressure at the chest wall
and upper abdomen
Positive pressure
application of positive pressure at airway opening
8
9.
Negative Pressure VentilatorsPerithoracic pump for replacement failing patients’ muscles,
wide-spread use for polio epidemics
• Manually operated ventilator (Woillez, 1876)
• Tank respirator
“iron lung”, cuirass, body suits
(1930 - 1950)
Patient care problems:
airway obstruction, low efficacy in interstitial lung
diseases, patient’s discomfort
9
10.
Negative Pressure Ventilators1876
1960
1930-1950
10
11.
Positive pressure ventilatorsVolume-cycled
Delivers set Vt at specified RR and terminates
respiration when Vt is delivered.
Airway pressures are determined by
respiratory system impedance (risk of
barotrauma).
Pressure-cycled
Limits flow, when set pressure is
delivered (may decrease minute ventilation)
11
12.
Positive pressure ventilatorsEvita 2
Dragger Germany
12
13.
VENTILATOR SETTINGSOXYGEN THERAPY
O2 delivery = Qt (1.39 x SaO2 x Hb + 0.0031 x PaO2)
FIO2 1
0.4
Adjustment of oxygen percent to achieve
SaO2 > 90%
FIO2 > 0.6
13
potential oxygen toxicity
(pulmonary fibrosis)
14.
VENTILATOR SETTINGSMINUTE VENTILATION (VOLUME) = Vt x RR
Physiologic Vt
Mechanical Vt
5mL/kg
7 – 10mL/kg
Limitation of Vt in cases of:
• airway obstruction
• one lung patient
• PIP > 40 cm H2O
RESPIRATORY RATE
10-12 /min or more
to match metabolic needs of the patient
14
15.
VENTILATOR SETTINGSInspiratory Flow Rate and Inspiratory to Expiratory Ratio
IFR L/min: rapidity of airflow in airways
Ti
= Inspiratory Time: the time to complete inspiration
Ti = Vt / Flow Rate
TE = Expiratory Time: time to complete exhalation
Ti + TE = T total: respiratory cycle
15
16.
CONVENTIONAL VENTILATIONCMV : Controlled Mandatory Ventilation
Full mechanical support
Maintaining full V min.
Reduction of oxygen and energy consumption
Indications:
Following intubation
Respiratory muscle fatigue ( for muscle rest)
Poor cardiac output ( VO2 of respiratory muscles)
16
17.
CONVENTIONAL VENTILATIONCMV
Airway pressure
Flow
inspirium
expirium
fixed rate
fixed Vt
Patient’s spontaneous effort
fixed flow rate
FIO2
Disadvantages:
• need for sedatives + relaxants
• unresponsiveness to the changing V min. of patient
• muscle atrophy
17
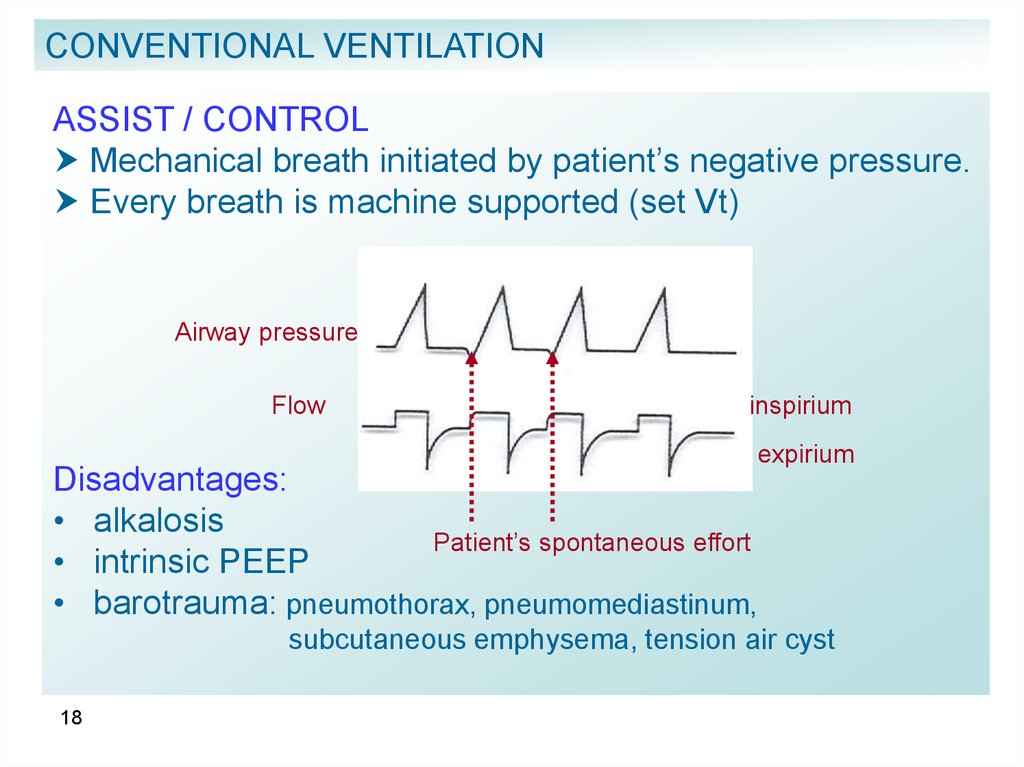
18.
CONVENTIONAL VENTILATIONASSIST / CONTROL
Mechanical breath initiated by patient’s negative pressure.
Every breath is machine supported (set Vt)
Airway pressure
Flow
inspirium
expirium
Disadvantages:
• alkalosis
Patient’s spontaneous effort
• intrinsic PEEP
• barotrauma: pneumothorax, pneumomediastinum,
subcutaneous emphysema, tension air cyst
18
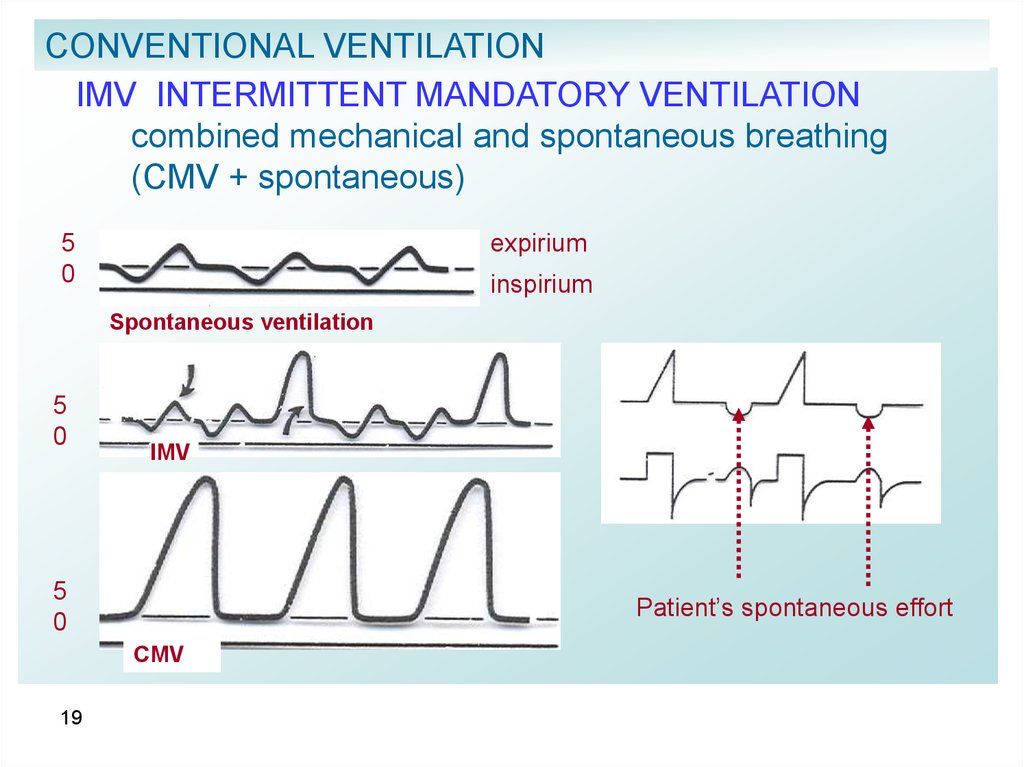
19.
CONVENTIONAL VENTILATIONIMV INTERMITTENT MANDATORY VENTILATION
combined mechanical and spontaneous breathing
(CMV + spontaneous)
5
0
expirium
inspirium
Spontaneous ventilation
5
0
IMV
5
0
Patient’s spontaneous effort
CMV
19
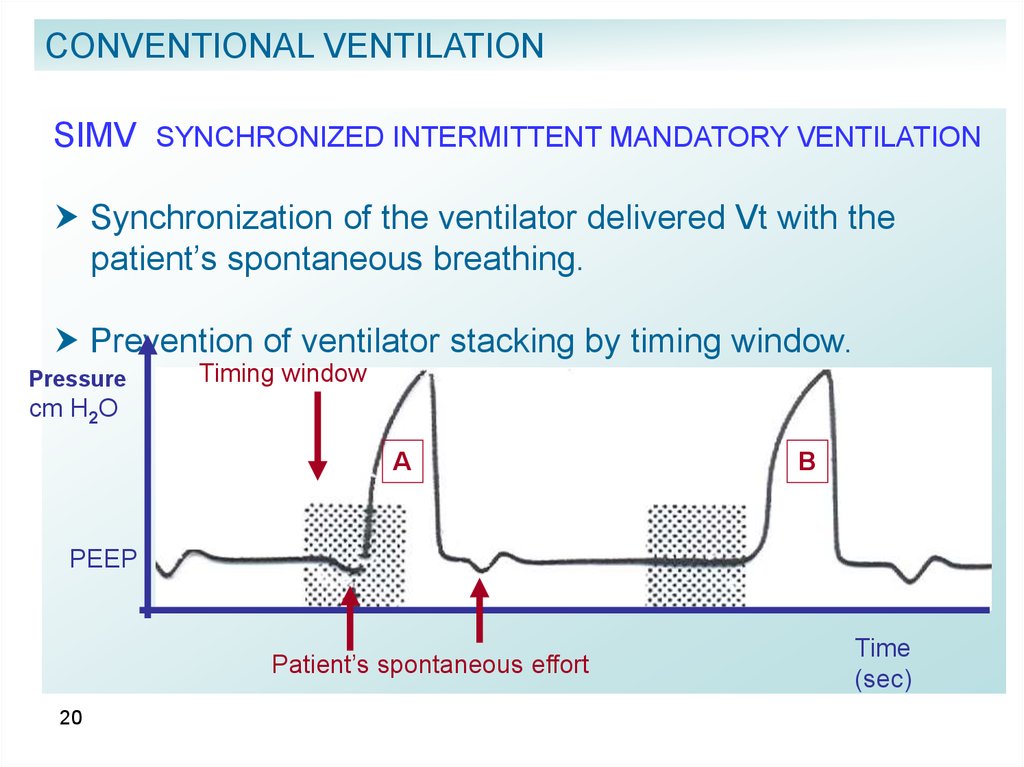
20.
CONVENTIONAL VENTILATIONSIMV SYNCHRONIZED INTERMITTENT MANDATORY VENTILATION
Synchronization of the ventilator delivered Vt with the
patient’s spontaneous breathing.
Prevention of ventilator stacking by timing window.
Pressure
Timing window
cm H2O
A
B
PEEP
Patient’s spontaneous effort
20
Time
(sec)
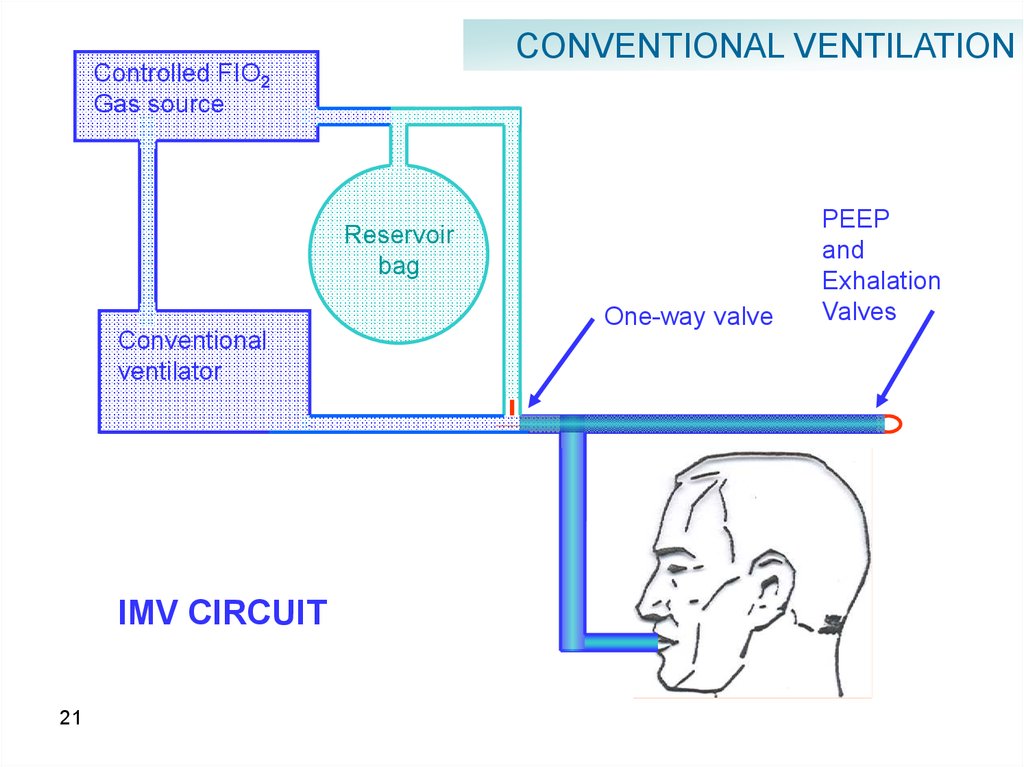
21.
CONVENTIONAL VENTILATIONControlled FIO2
Gas source
Reservoir
bag
One-way valve
Conventional
ventilator
IMV CIRCUIT
21
PEEP
and
Exhalation
Valves
22.
CONVENTIONAL VENTILATIONIMV / SIMV
Advantages
decreased need in sedatives
prevention of muscle atrophy
lower airway pressure and
intrathoracic pressure
hemodynamic stability
reduction in alkalosis
patient’s ability to regulate his rate and
Vt according to metabolic requirements
22
23.
CONVENTIONAL VENTILATIONIMV / SIMV
Disadvantages
respiratory muscle fatigue
increased work of breathing due to highly
resistant respiratory circuit, small diameter (ETT)
possibility of respiratory acidosis
risk of cardiac decompensation
in patient with heart disease
23
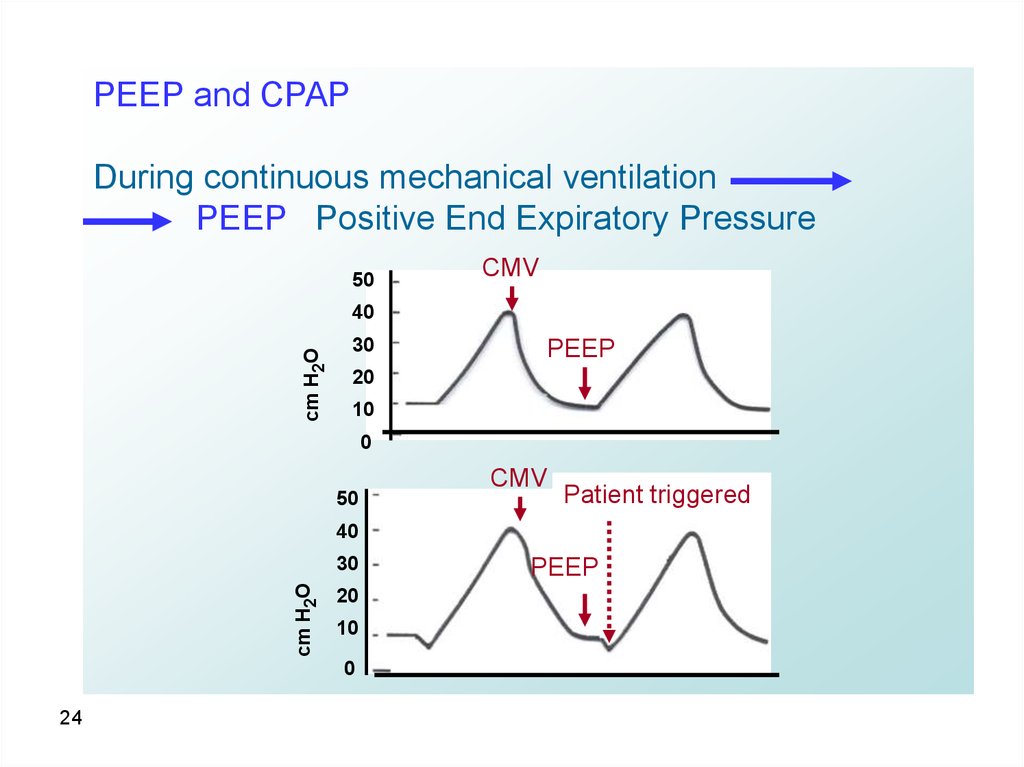
24.
PEEP and CPAPDuring continuous mechanical ventilation
PEEP Positive End Expiratory Pressure
50
CMV
cm H2O
40
30
PEEP
20
10
0
50
CMV
Patient triggered
40
cm H2O
30
20
10
0
24
PEEP
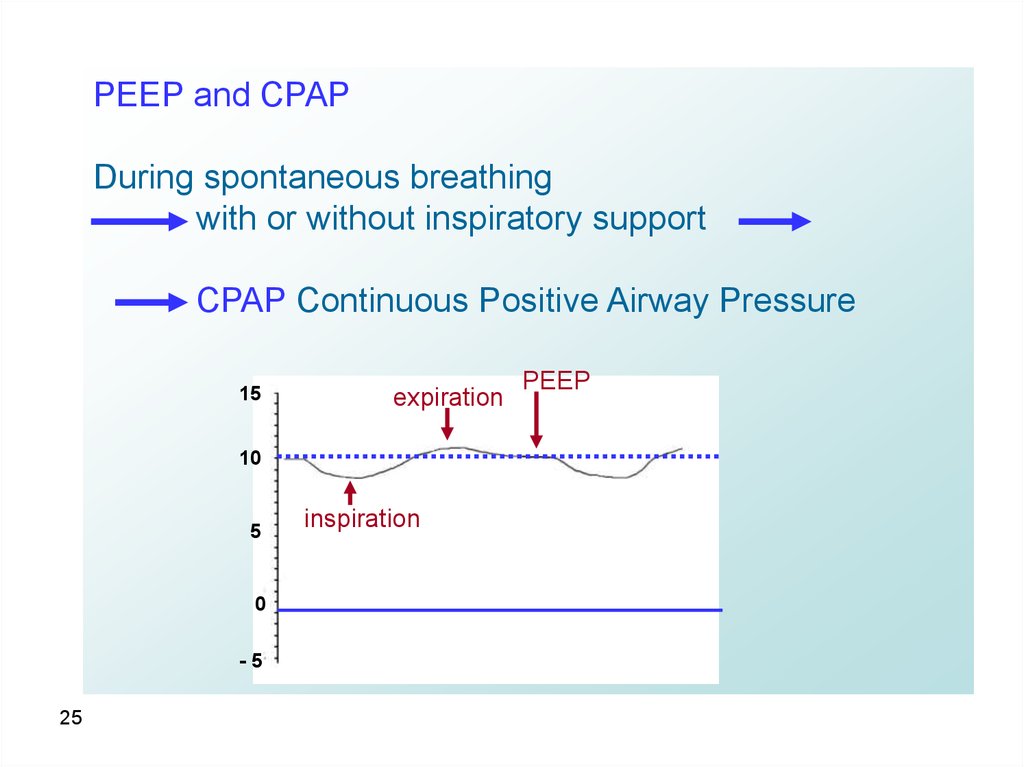
25.
PEEP and CPAPDuring spontaneous breathing
with or without inspiratory support
CPAP Continuous Positive Airway Pressure
15
expiration
10
5
0
-5
25
inspiration
PEEP
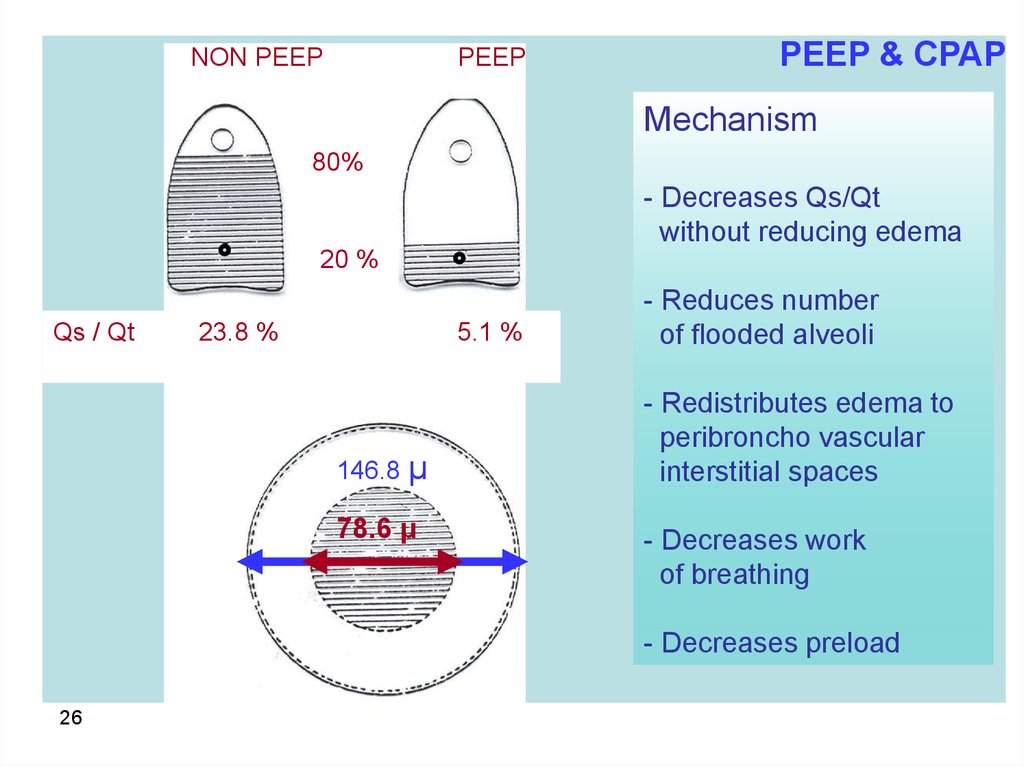
26.
NON PEEPPEEP
PEEP & CPAP
Mechanism
80%
- Decreases Qs/Qt
without reducing edema
20 %
Qs / Qt
23.8 %
5.1 %
146.8 μ
78.6 μ
- Reduces number
of flooded alveoli
- Redistributes edema to
peribroncho vascular
interstitial spaces
- Decreases work
of breathing
- Decreases preload
26
27.
PEEP and CPAPGoals
Reduction of shunt
recruitment of previously collapsed alveoli
ventilation of non-ventilated zones
continuous gas exchange (during expiration)
Prevention of atelectasis
prevention of brisk alveolar inflation and deflation
> protection of surfactant and pulmonary parenchyma
27
28.
PEEP and CPAPComplications
increased intrathoracic pressure
decrease of venous returns
decrease of cardiac output
EFFECT of PEEP
venous
28
compression
29.
PEEP and CPAPComplications
Increased ADH secretion, decrease of renal artery
perfusion pressure
decrease of urinary output and creatinine
clearance
decreased venous return from brain
increased ICP
decrease of CPP
barotrauma – induced by PEEP ≈ 20%
29
30.
PEEP / CPAP TherapyTitrate EEP until:
PO2 ≈ 60 mmHg (Sat O2 ≈ 90%) on FIO2 < 60%
Qs / Qt < 15%
Best PEEP on
volume-pressure
loop
Volume (mL)
provided cardiac output is maintained
D
C
500
B
250
A
0
30
Upper deflection point
Lower inflection point
15
30
Pressure cmH20
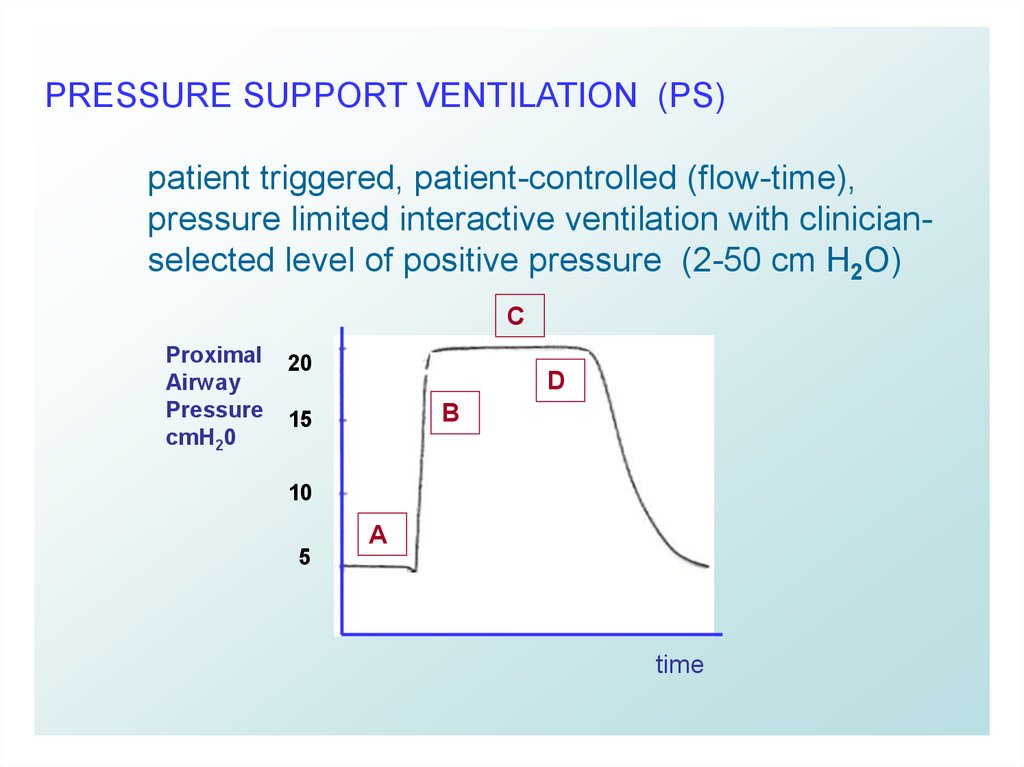
31.
PRESSURE SUPPORT VENTILATION (PS)patient triggered, patient-controlled (flow-time),
pressure limited interactive ventilation with clinicianselected level of positive pressure (2-50 cm H2O)
C
Proximal
Airway
Pressure
cmH20
20
D
B
15
10
5
A
time
31
32.
PRESSURE SUPPORT VENTILATION (PS)Synchrony
PS interaction with ventilatory muscles
PS adds to the patient’s effort to deliver Vt
Overload of ventilatory muscles
tachypnea, small Vt
PS
Vt,
Vt mL/kg
12
RR
8
4
Muscle tension
32
Ventilator pressure
33.
PRESSURE SUPPORT VENTILATION (PS)Synchrony
Patient interaction with ventilator:
Trigger
(prompt breath initiation, ventilator
sensitivity and responsiveness)
Flow
adjustment of the gas delivery to the patient’s
effort
Cycling
ventilator breath termination with the end of
patient’s effort 25-30% of peak flow
33
34.
PRESSURE SUPPORT VENTILATION (PS)Titration of PS
to overcome endotracheal tube resistance
(6-10 cmH2O)
to achieve effective Vt and V min without
causing respiratory overload
non-invasive application
BIPAP* = CPAP + Pressure Support
*Bi-level Positive Airway Pressure
34
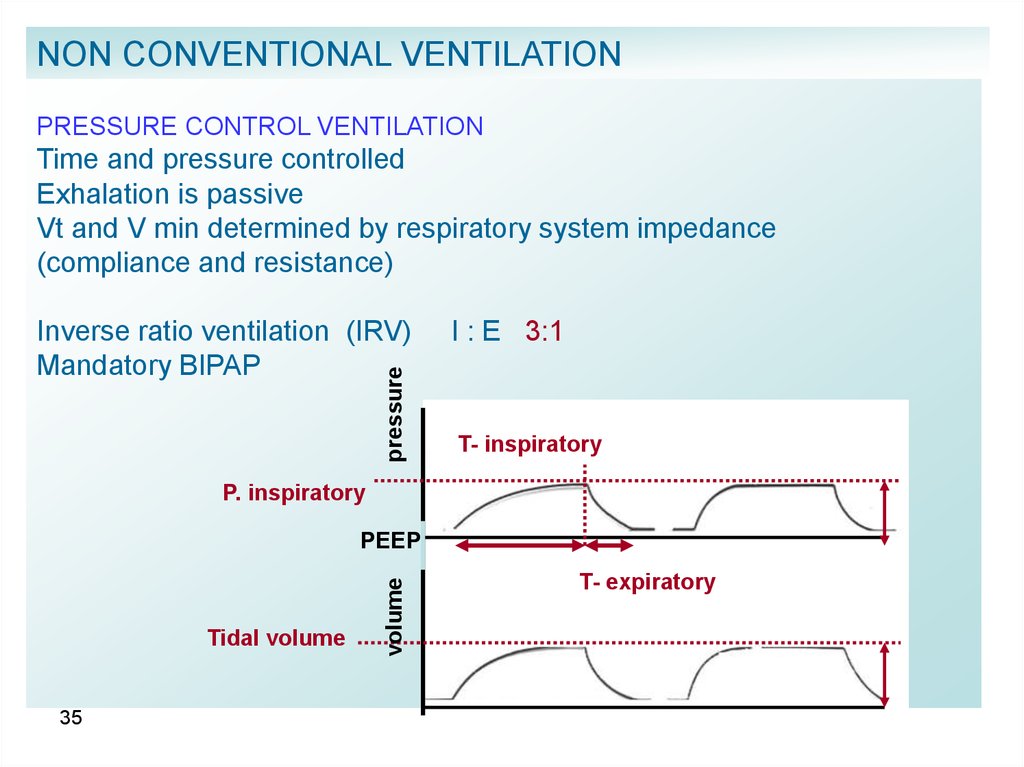
35.
NON CONVENTIONAL VENTILATIONPRESSURE CONTROL VENTILATION
Time and pressure controlled
Exhalation is passive
Vt and V min determined by respiratory system impedance
(compliance and resistance)
pressure
Inverse ratio ventilation (IRV)
Mandatory BIPAP
I : E 3:1
T- inspiratory
P. inspiratory
Tidal volume
35
volume
PEEP
T- expiratory
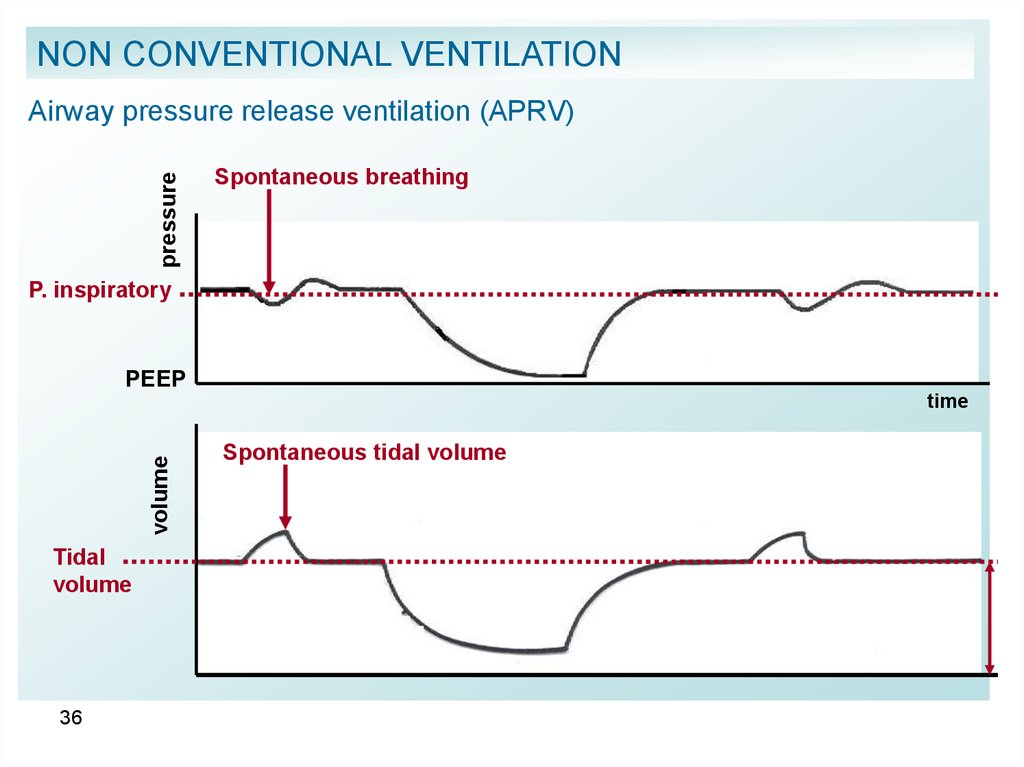
36.
NON CONVENTIONAL VENTILATIONpressure
Airway pressure release ventilation (APRV)
Spontaneous breathing
P. inspiratory
PEEP
volume
time
Tidal
volume
36
Spontaneous tidal volume
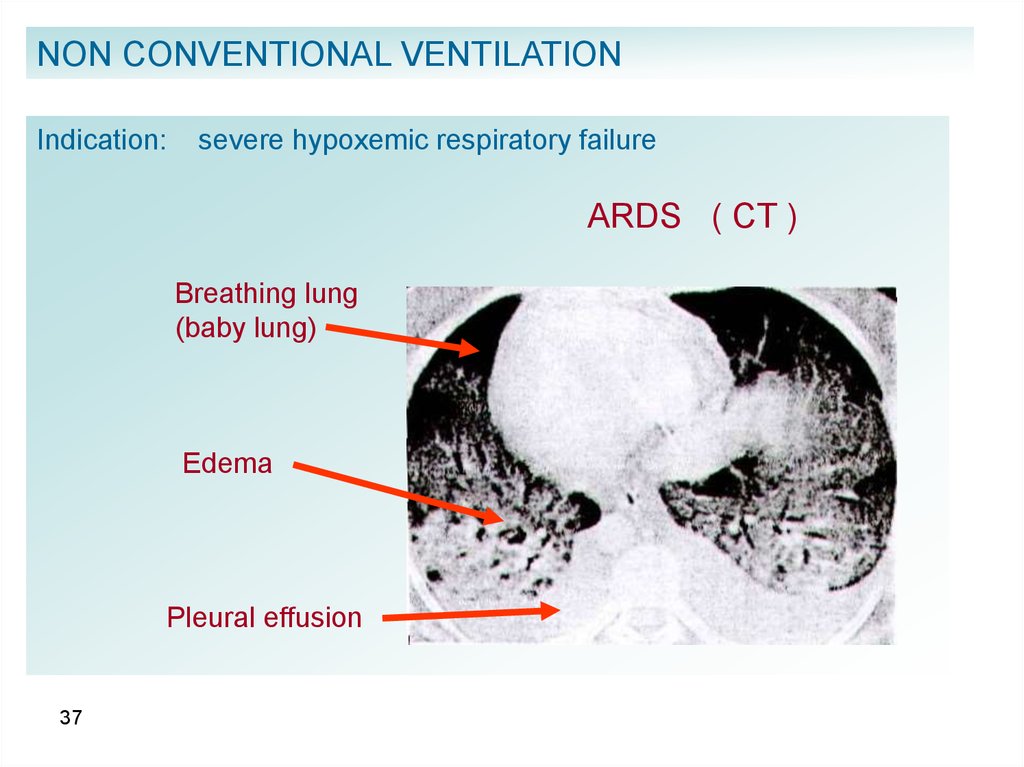
37.
NON CONVENTIONAL VENTILATIONIndication:
severe hypoxemic respiratory failure
ARDS ( CT )
Breathing lung
(baby lung)
Edema
Pleural effusion
37
38.
NON CONVENTIONAL VENTILATIONOpen Lung Conception
Pressure controlled, Inverse ratio ventilation with permissive
hypercapnia:
Permissive hypercapnia = increase of PCO2 until pH reaches 7.2
at pH < 7.2 give bicarbonate
Prone position
Nitric Oxide
Selective pulmonary vasodilator
38
Gravitational
force
39.
NON CONVENTIONAL VENTILATIONProportional assist ventilation for spontaneously breathing patients
gives maximal Vt with minimal inspiratory pressure, by measuring
lung compliance and resistance
Perflubron liquid ventilation
injection of perfluorocarbon into the trachea aiming to recruiting
collapsed alveoli.
ECMO Extra Corporeal Membrane Oxygenator
IVOX
39
IntraVenous Oxygenator (membrane “lung” inserted in inferior
vena cava
40.
NON CONVENTIONAL VENTILATIONHIGH FREQUENCY VENTILATION
RR 60 – 3600 / min
CONVECTION
DIFFUSION
TYPES
I.
HFPPV high frequency positive pressure ventilation
II.
III.
HFO
HFJT
high frequency oscillation
high frequency jet ventilation
INDICATIONS
I.
II.
40
Broncho-pleural fistula
Hypoxemic respiratory failure
41.
VEANING FROM MECHANICAL VENTILATIONNecessary conditions for considering discontinuation from
Mechanical Ventilation:
Stable circulation and absence of myocardial ischemia,
sepsis and uncontrolled acidosis
Adequate pulmonary O2 exchange as evidenced by
SaO2 > 90% with FIO2 < 0.4 and PEEP < 7.5 cm H2O
Adequate ability to ventilate spontaneously (Vt > 5 mL/Kg,
VC = 3 x Vt, NIF > 30 cmH2O, and f < 36 /min)
41
42.
VEANING FROM MECHANICAL VENTILATIONCMV > SIMV
+ PS (15 cmH2O)
CPAP
+ PS (15 cmH2O)
CPAP
+ PS (8 cm H2O)
Disconnection + T Tube
42
Extubation + O2 mask