










 electronics
electronicsSimilar presentations:








")

Organisation of dental clinics, departments. Equipment of the dental office. Dental installations. Turbine, micromotor, tips
1.
Тема № 2Organisation of dental clinics,
departments. Equipment of the
dental office. Dental installations.
Turbine, micromotor, tips. Cutting
and abrasive tools, their purpose.
Asepsis, antiseptics, disinfection and
sterilisation – prevention of
infectious and iatrogenic diseases.
Ergonomics in dentistry
Organization of the dentist's work and
equipment of the dental office
2.
Organization in dental clinic.Dental polyclinic is a medical and preventive institution whose activities
are aimed at the prevention of dental diseases, timely detection and
treatment of patients with diseases of the maxillofacial region. The dental
polyclinic is organised in accordance with the established procedure and
carries out its activities among the population, at industrial enterprises, in
higher and secondary educational institutions, construction and other
organisations, including, in appropriate cases, in children's groups..
3.
The main tasks of the polyclinic:• carrying out measures for the prevention of the maxillofacial region
diseases among the population and in organized collectives;
• organization and implementation of measures aimed at early detection of
patients with maxillofacial region diseases and their timely treatment;
• provision of qualified outpatient dental care to the population.
4.
The dental clinic may include:• departments of therapeutic and surgical dentistry (including, where
appropriate, children's departments);
• dental units;
• dental prosthetics departments;
• auxiliary units (X-ray, physiotherapy rooms);
• registry;
• administrative and economic part;
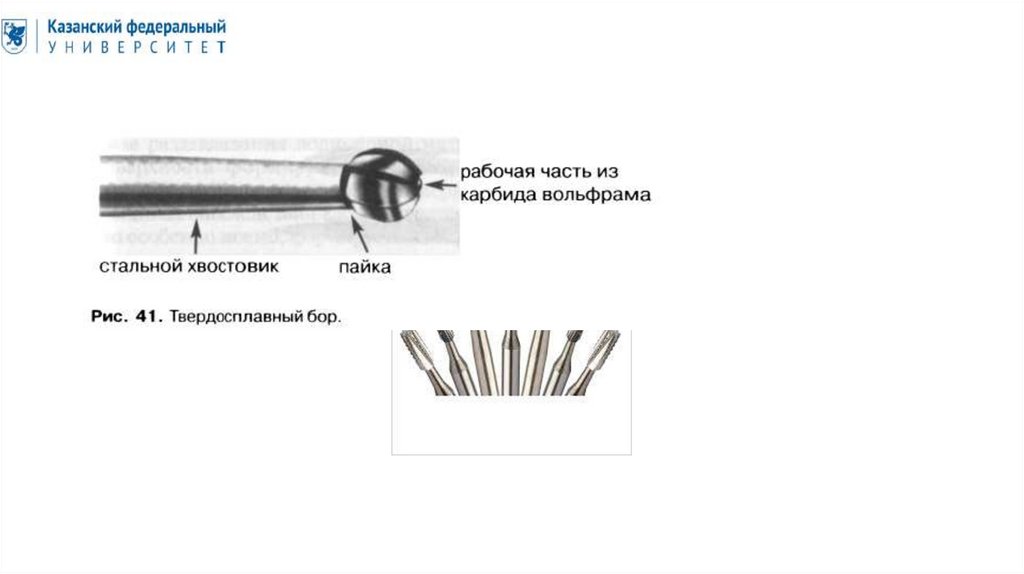
• accounting.
In addition, departments and offices for providing highly specialised dental care
to patients can be organised in the polyclinic. These include a periodontal office,
an office for the reception of patients with pathological changes of the mucose
layer of oral cavity, offices of anaesthesiology, orthodontics, prevention,
acupuncture, hirudotherapy, functional diagnostics. In large dental clinics
(regional, city), departments (offices) of implantology, anesthesiology and
resuscitation, restoration therapy, endodontics, clinical diagnostic laboratories,
central sterilization, pharmacy, etc. are being deployed.
5.
Dental office equipment.Main equipment:
► Dental unit.
► A chair for the patient.
► A chair for a doctor.
► A chair for an assistant.
► Dental table.
Auxiliary equipment :
► Devices for electronic data processing.
► Apexlocator.
► Polymerization lamp.
► Microscope.
6.
Equipment for a nurse:► Documentation desk.
► Computer.
► Chair.
► A safe for storing documents.
Equipment for the nurse:
► A table for sorting the used tools.
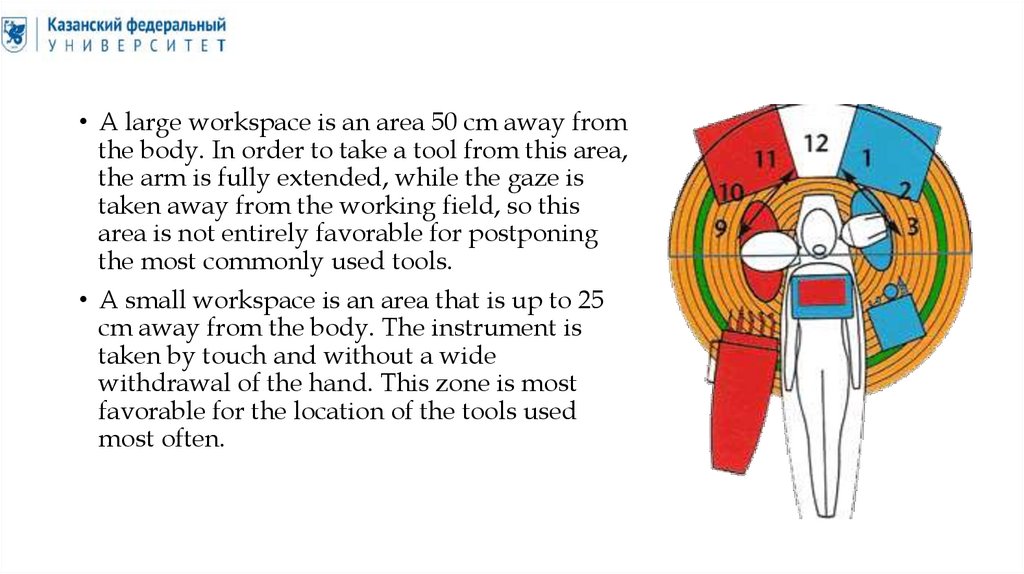
► Sink for washing tools.
Equipment for hand treatment and pre-sterilization cleaning:
► Hand washing sink.
► Sink for washing tools.
► Containers with disinfectant and cleaning solutions.
7.
Disinfection and sterilisation equipment:► Autoclave, dry-burning cabinet
► Glassperlene steriliser.
► Ultrasonic washing.
► Device for disinfection and lubrication of tips (Assistina, Terminator).
► Sterile table, UV shelf.
► Quartz lamp.
8.
Medical furniture:► Cabinet for storing medicines, dressings and filling materials.
► Cabinet for toxic substances (Class A).
► Cabinet for potent substances (Class B).
► Cabinet for first aid kit.
► Couch, chairs for patients.
► Cabinet for sanitary equipment.
9.
Dentist workplaceThe workplace of a dentist is a conditional
concept that assumes the presence of a
special room (or part of it) with specific
equipment, tools and materials necessary for
solving professional tasks.
10.
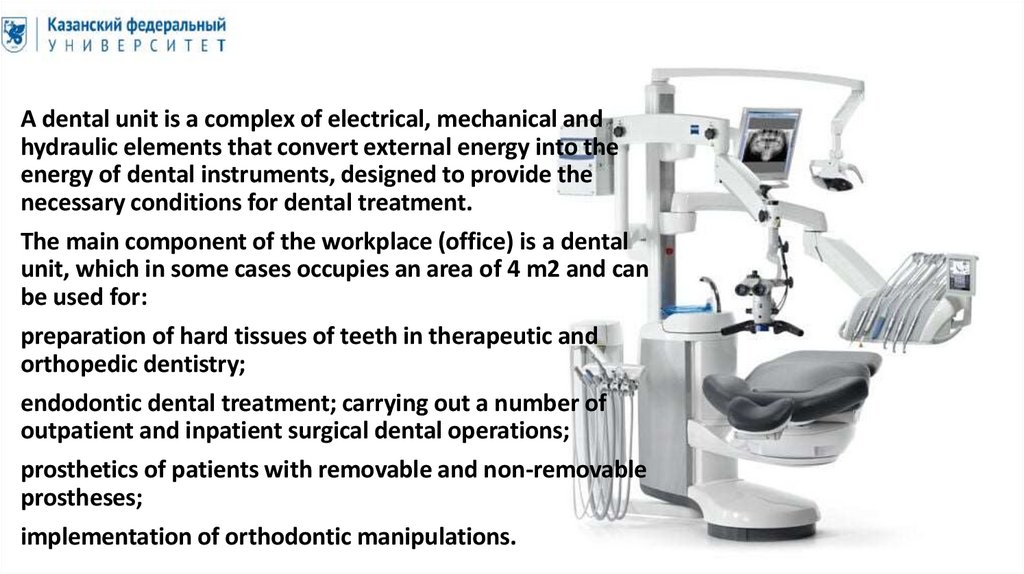
A dental unit is a complex of electrical, mechanical andhydraulic elements that convert external energy into the
energy of dental instruments, designed to provide the
necessary conditions for dental treatment.
The main component of the workplace (office) is a dental
unit, which in some cases occupies an area of 4 m2 and can
be used for:
preparation of hard tissues of teeth in therapeutic and
orthopedic dentistry;
endodontic dental treatment; carrying out a number of
outpatient and inpatient surgical dental operations;
prosthetics of patients with removable and non-removable
prostheses;
implementation of orthodontic manipulations.
11.
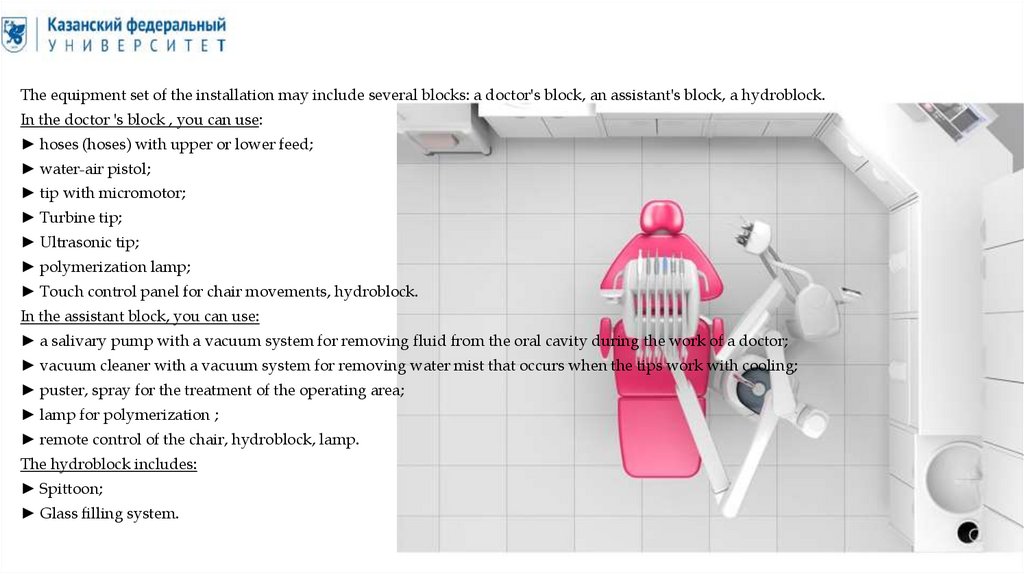
The equipment set of the installation may include several blocks: a doctor's block, an assistant's block, a hydroblock.In the doctor 's block , you can use:
► hoses (hoses) with upper or lower feed;
► water-air pistol;
► tip with micromotor;
► Turbine tip;
► Ultrasonic tip;
► polymerization lamp;
► Touch control panel for chair movements, hydroblock.
In the assistant block, you can use:
► a salivary pump with a vacuum system for removing fluid from the oral cavity during the work of a doctor;
► vacuum cleaner with a vacuum system for removing water mist that occurs when the tips work with cooling;
► puster, spray for the treatment of the operating area;
► lamp for polymerization ;
► remote control of the chair, hydroblock, lamp.
The hydroblock includes:
► Spittoon;
► Glass filling system.
12.
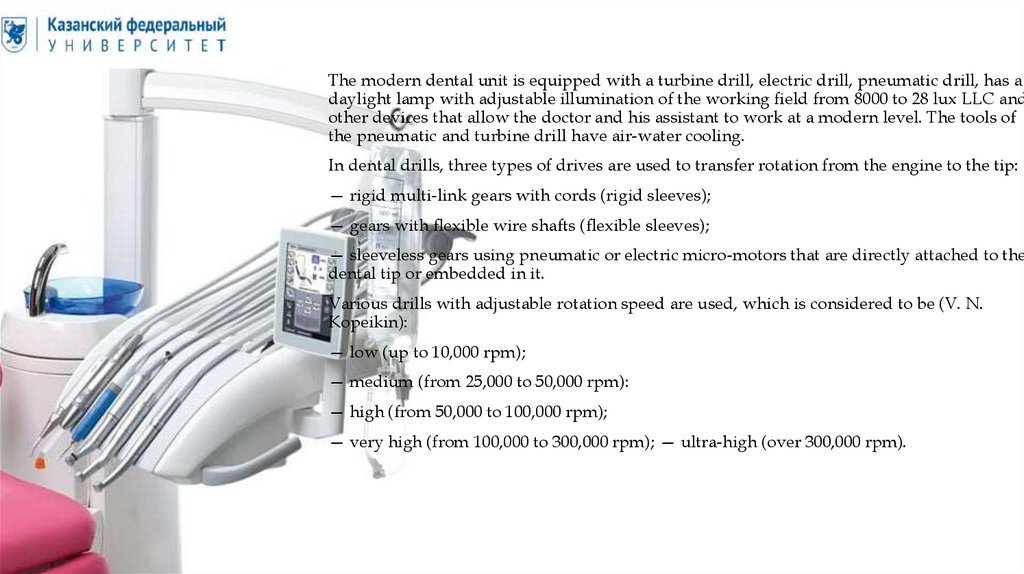
The modern dental unit is equipped with a turbine drill, electric drill, pneumatic drill, has adaylight lamp with adjustable illumination of the working field from 8000 to 28 lux LLC and
other devices that allow the doctor and his assistant to work at a modern level. The tools of
the pneumatic and turbine drill have air-water cooling.
In dental drills, three types of drives are used to transfer rotation from the engine to the tip:
— rigid multi-link gears with cords (rigid sleeves);
— gears with flexible wire shafts (flexible sleeves);
— sleeveless gears using pneumatic or electric micro-motors that are directly attached to the
dental tip or embedded in it.
Various drills with adjustable rotation speed are used, which is considered to be (V. N.
Kopeikin):
— low (up to 10,000 rpm);
— medium (from 25,000 to 50,000 rpm):
— high (from 50,000 to 100,000 rpm);
— very high (from 100,000 to 300,000 rpm); — ultra-high (over 300,000 rpm).
13.
• The adjustment of the seat and back of the chair is carried out by meansof a hydraulic or electromechanical drive.
14.
• A dental tip is a tool that converts the energy transmitted from the dentalunit into the corresponding movements of the working tool (boron,
polishing head, etc.).
• Used:
• When preparing hard tissues of teeth;
• Endodontic treatment;
• Professional oral hygiene.
15.
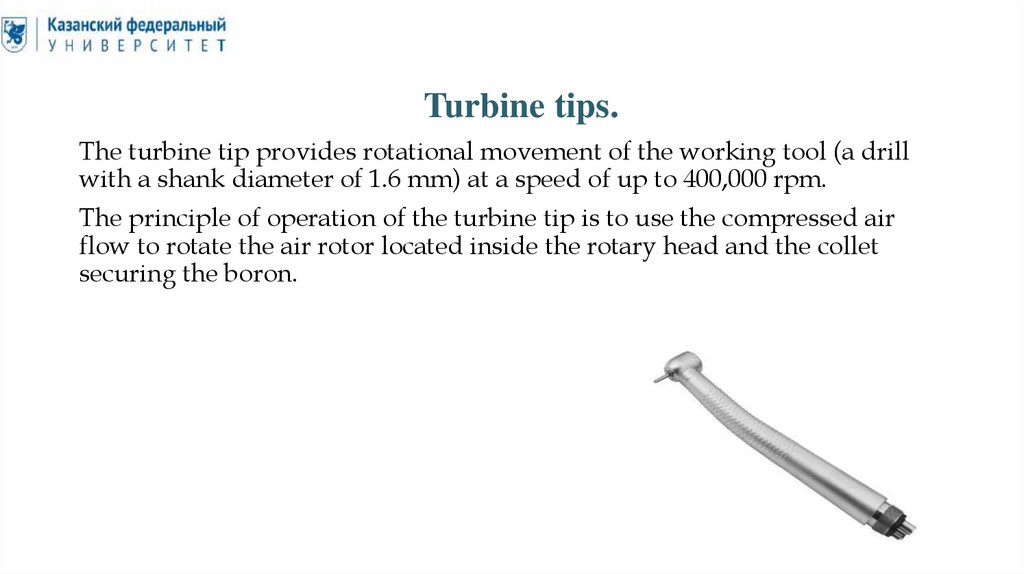
Turbine tips.The turbine tip provides rotational movement of the working tool (a drill
with a shank diameter of 1.6 mm) at a speed of up to 400,000 rpm.
The principle of operation of the turbine tip is to use the compressed air
flow to rotate the air rotor located inside the rotary head and the collet
securing the boron.
16.
The following specifications are used to classify turbine tips.► Type of bearing:
• tips with ball metal bearings;
• tips with ceramic ball bearings (have greater durability compared to
metal bearings and better noise characteristics);
• tips with "air" bearings (provide the maximum speed of rotation of the
tool, are not sufficiently resistant to lateral loads on the boron).
► Return air extraction system:
• tips having a channel for diverting return air to the dental unit
(MIDWEST);
• handpieces that do not have a channel for diverting back air into the
dental unit (BORDEN; the disadvantage is blowing the hand through the
connection of the tip with the sleeve).
17.
► Cooling spray supply system:• tips with separate water and air supply (MIDWEST, BORDEN, 3 holes);
• tips with joint supply of water and air (BORDEN).
► Irrigation system of the working area:
• single-channel spray supply;
• two-channel spray supply;
• three-channel spray supply;
• four-channel spray supply.
18.
► Backlight design:• the light source is located in the tip;
• the light source is located in the sleeve of the dental unit, hard and fiber
light guides are located in the body of the tip.
► Tip collet design:
• push-button collet (provides quick replacement of the working tool,
reliable during long-term operation of the tip);
• screw collet (the clamping device requires the use of a special key, which
increases the time spent on tool replacement);
• friction collet (tool replacement is performed using a pusher).
19.
Micromotors.Micromotors are used to convert the energy of the airflow or electric power
of the dental unit into kinetic energy, followed by the transfer of rotational
motion to the micromotor tip.
There are air micromotors, electric brush motors and electric brushless
motors. The main structural element of all types of micromotors is the rotor,
from which rotation is transmitted through the pulley to the tip.
20.
• The principle of operation of the air micromotor is similar to the principle ofoperation of the turbine tip. The positive properties of the air micromotor
are a long continuous operation mode and high reliability of the design,
however, in comparison with electric micromotors, the cutting force and the
range of tool rotation speed (4000-25,000 rpm) the air micromotors have
significantly less.
• The design of electric brush micromotors includes carbon brushes through
which electric current enters the wire winding of the rotor and creates a
magnetic field, which, in turn, interacting with the magnetic field of
permanent magnets installed in the micromotor housing, drives the rotor.
The disadvantages of electric brush micromotors include the need to replace
carbon brushes with 30% wear, as well as intermittent operation to prevent
overheating of the micromotor. At the same time, electric brush
micromotors provide precise adjustment of the tool rotation speed and the
ability to work in a wide range of speeds (1000-40 000 rpm).
21.
Micromotor tips.Micromotor tips are used to transform the type and speed of movement
that micromotors tell them, and transfer this movement to the working tool.
Micromotor tips convert the rotational motion of the micromotor:
► into reciprocating motion (tips for endodontics);
► in rotary-oscillatory motion (tips for prevention);
► in vibratory motion (tips for condensation of amalgam);
► Retain rotational motion.
22.
• Depending on the type of tip, the speed of movement:• ► increases (increasing tips, red marking);
• ► reduced (lowering tips, green marking);
• ► does not change (blue marking).
• According to the presence and method of supplying the cooling spray,
micromotor tips are divided into tips:
• ► with external connection to the spray channel;
• ► With internal spray channel;
• ► Without spray.
23.
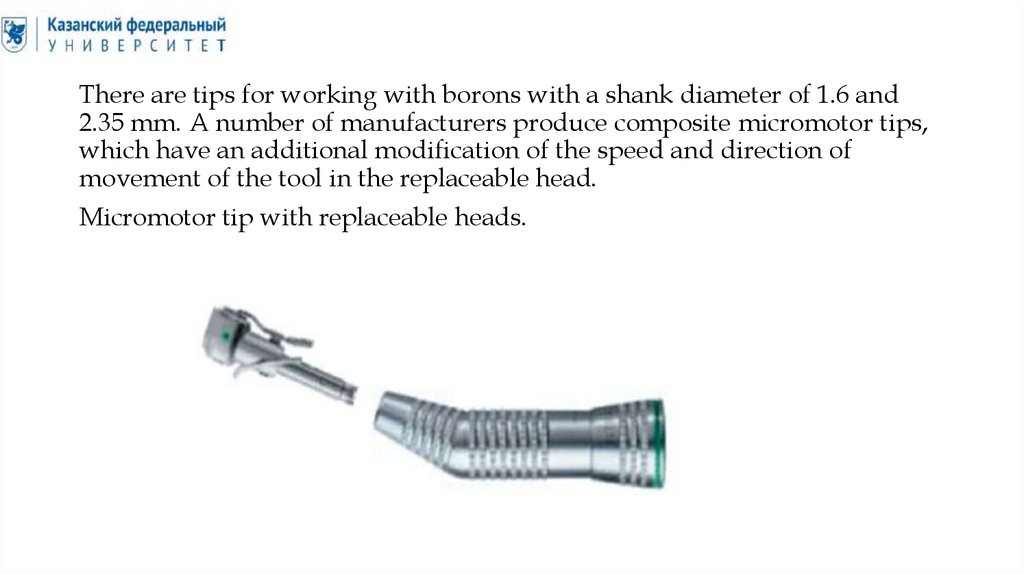
There are tips for working with borons with a shank diameter of 1.6 and2.35 mm. A number of manufacturers produce composite micromotor tips,
which have an additional modification of the speed and direction of
movement of the tool in the replaceable head.
Micromotor tip with replaceable heads.
24.
According to the shape of the body, straight and angular micromotor tipsare distinguished. Tips for special types of work may have some design
differences (preventive tips, endodontic tips, tips for condensation of
amalgam, tips for working with separation discs, etc.).
25.
Straight tips.Angular tips.
26.
Tips for removal of dental deposits.Scaler. The principle of operation of the scaler is to create high-frequency
vibrations on the central axis located in the body of the tip, followed by the
transmission of an ultrasonic wave to a replaceable nozzle. Depending on the
method of generating an ultrasonic wave, piezoelectric and air scalers are
distinguished.
► In piezoelectric scalers, ultrasonic vibrations are created by supplying an
alternating electric current to a piezoelectric element, while the nozzle oscillates in
the same plane with a frequency of up to 35,000 Hz.
► In air scalers, ultrasonic vibrations occur when the air flow indirectly acts on the
central axis, which transmits circular vibrations to the nozzle. The frequency of
vibrations of the nozzle in air scalers is less than in piezoelectric, and is 7000 Hz. In
addition to removing dental deposits, scalers are also used for filling root canals
during root apical resection, preparing approximally located carious cavities and
setting tabs and intra-channel pins.
27.
Scaler.28.
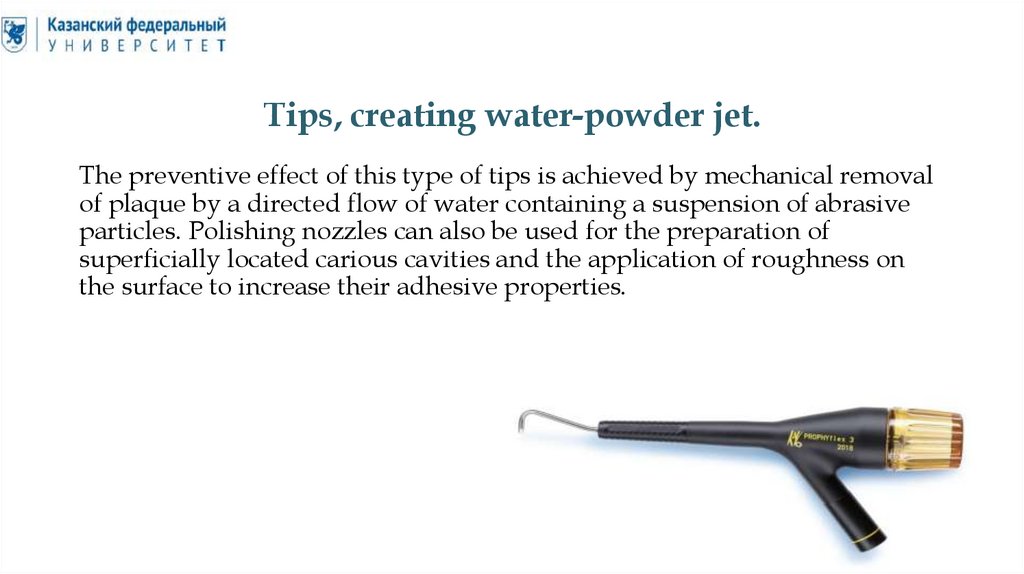
Tips, creating water-powder jet.The preventive effect of this type of tips is achieved by mechanical removal
of plaque by a directed flow of water containing a suspension of abrasive
particles. Polishing nozzles can also be used for the preparation of
superficially located carious cavities and the application of roughness on
the surface to increase their adhesive properties.
29.
Endodontic tips.Endodontic tips are used with standard micromotors of dental installations
(air or electric). Without exception, all endodontic tips that are used with
micromotors of dental units have various types of gearboxes to reduce the
speed of movement of the instrument in the channel. Low speed (250-350
rpm) is a prerequisite for safe operation in the channel. Endonecons, in
turn, are divided into two groups.
30.
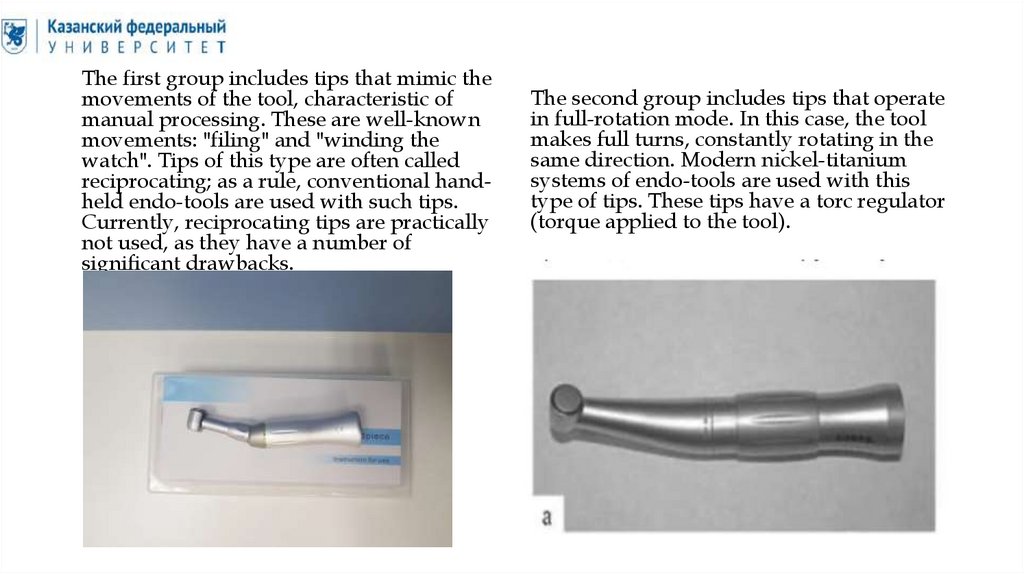
The first group includes tips that mimic themovements of the tool, characteristic of
manual processing. These are well-known
movements: "filing" and "winding the
watch". Tips of this type are often called
reciprocating; as a rule, conventional handheld endo-tools are used with such tips.
Currently, reciprocating tips are practically
not used, as they have a number of
significant drawbacks.
The second group includes tips that operate
in full-rotation mode. In this case, the tool
makes full turns, constantly rotating in the
same direction. Modern nickel-titanium
systems of endo-tools are used with this
type of tips. These tips have a torc regulator
(torque applied to the tool).
31.
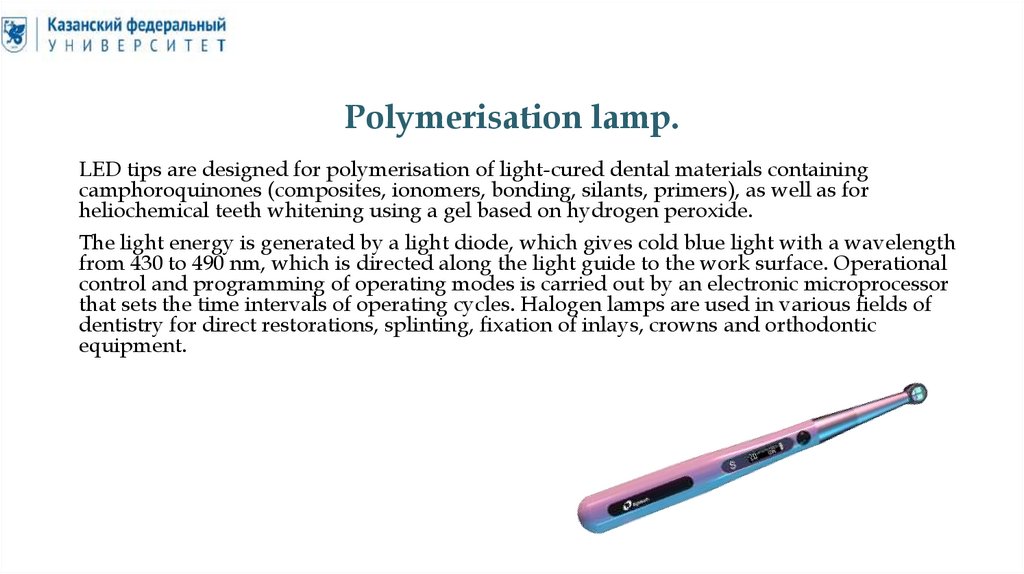
Polymerisation lamp.LED tips are designed for polymerisation of light-cured dental materials containing
camphoroquinones (composites, ionomers, bonding, silants, primers), as well as for
heliochemical teeth whitening using a gel based on hydrogen peroxide.
The light energy is generated by a light diode, which gives cold blue light with a wavelength
from 430 to 490 nm, which is directed along the light guide to the work surface. Operational
control and programming of operating modes is carried out by an electronic microprocessor
that sets the time intervals of operating cycles. Halogen lamps are used in various fields of
dentistry for direct restorations, splinting, fixation of inlays, crowns and orthodontic
equipment.
32.
Tips for removing prosthetic structure.The tip is designed for non-destructive
removal of crowns, bridges, and other fixed
orthopedic structures. The tip is mounted on
an air drive; special forceps, staples and
hinges are used to secure the prosthetic
structures. Compared with non-powered
tools, the machine tip is more efficient, since
it allows you to control the disintegration
process and has more power.
33.
Cutting and abrasive tools.Dental burs are cutting or abrasive rotating tools used when working with a
tip for preparing hard tooth tissues, processing fillings, etc.
Consist of:
• Rod (tail);
• Necks;
• Heads.
34.
• There are burs for straight, angular and turbine tips.• The burs for the straight tip have a shank with a diameter of 2.35 mm and
a length of 44.5 mm.(4.4cm).
• For the angular tip, burs with a shank length of 22, 26 and 34 mm and a
diameter of 2.35 mm are produced. At the end of the shank of these hogs,
a circulation thread is applied to fix them in the tip.
• The diameter of the shank of the hogs for the turbine tip is 1.6 mm, and its
length can be different. The absolute accuracy of the concentric rotation of
such hogs creates ideal working conditions.
• Burs with a length of 19 mm, long burs with a length of 21 mm and extra–
long burs with a length of 25 mm are also available. The end part of the
hog shank for the turbine tip can be flat or rounded.
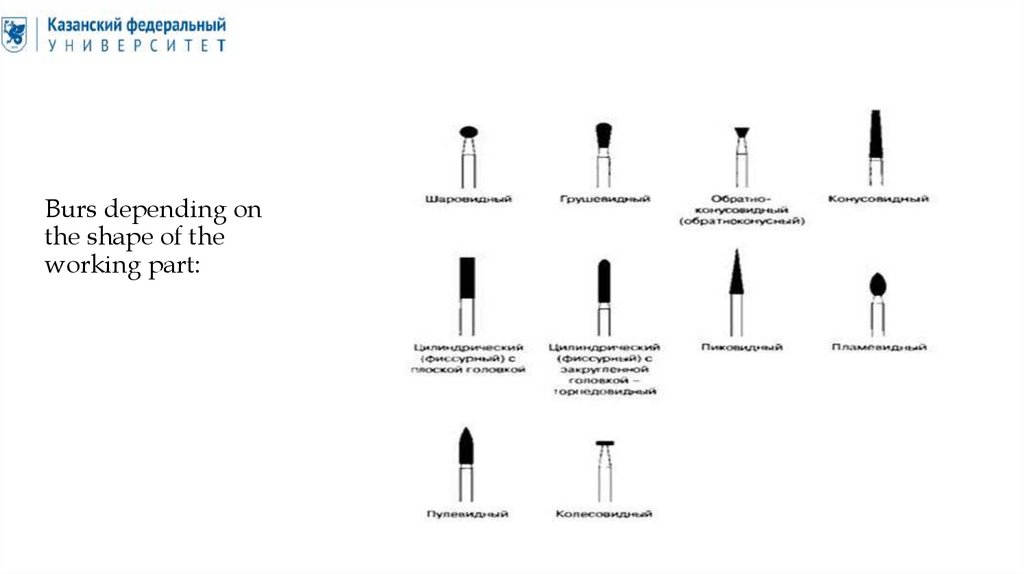
35.
Burs depending onthe shape of the
working part:
36.
By material of working part:• Burs with a working surface made of steel.
• The working surface of the drills and cutters is made of hardened
tungsten vanadium subsidized tool steel or hardened stainless steel. Such
burs are used only in drills operating at low speeds when performing
interventions on bone tissues during surgical operations. For the
preparation of hard tooth tissues, steel bores are currently rarely used,
since they are significantly inferior to carbide bores. In the dental
laboratory, steel burs can be used for processing plastics and gypsum.
37.
38.
• Carbide burs.• The working part of carbide drills and milling cutters is made of tungsten
carbide. Carbide burs are characterized by a long service life and high
cutting capacity. They are universal, can be used both in therapeutic
dentistry and in orthopedics. The number of cutting edges on the working
surface of the boron determines the indications for its use. So, the more
cutting edges, the smoother the surface becomes after processing. Carbide
burs with a large number of cutting edges are used for the final (finishing)
finishing of seals made of composites. There may be 8,10,12,16,30 cutting
faces on the working surface of such hogs. For the usual procedure of
preparation of hard tissues of teeth, burs with 6 or 8 blades are used.
39.
40.
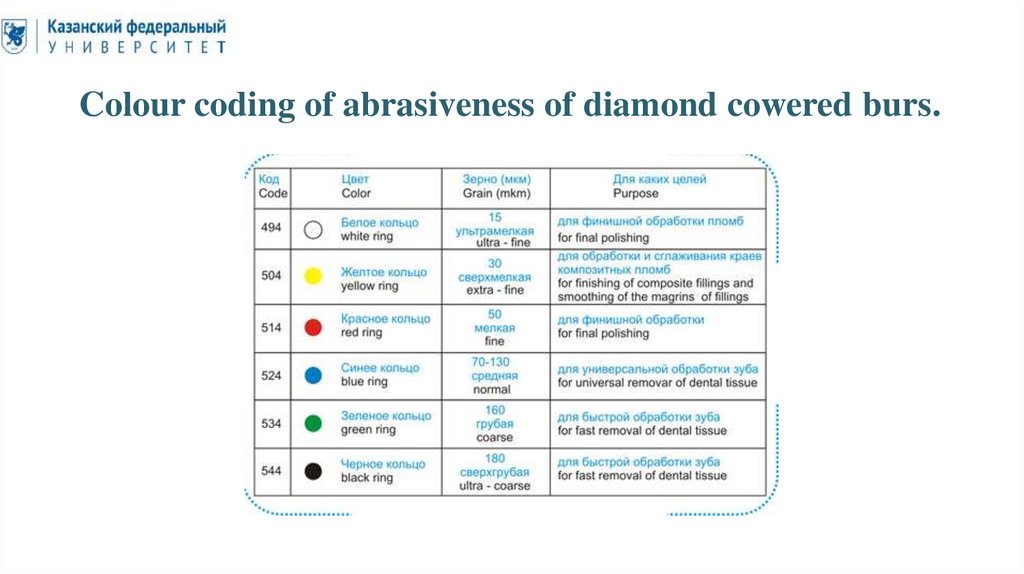
• Diamond-coated burs.• Natural and synthetic diamonds are used as abrasive grains for the
production of the working part of the boron. Synthetic diamond grain is
inferior to natural in its properties and cutting characteristics. The quality
of the tool depends on the method of fixing the diamond grain. There are
two options. One of the options is to apply diamond chips at different
levels. As a rule, such tools are of poor quality. With this technology,
diamond grains unevenly protrude from the binder layer, which leads to
accelerated wear and reduced tool durability. The best quality are bores
with a uniform diamond coating. Such burs have accelerated cutting
ability, they have reduced heat generation during operation. This ensures
a longer service life of the hog.
41.
Colour coding of abrasiveness of diamond cowered burs.42.
43.
• Bores with ruby coating.• Instruments with ruby chips are designed for the final processing of
dental plastic products. The binding element in them, as in diamond tools,
is metal. The advantage of ruby finiers is the absence of the effect of
heating the surface, which allows for precise adjustment of plastic
prostheses without deformation of the structure.
44.
45.
• Bores with corundum coating.• Corundum (Al2O3) is used as an abrasive additive in tools intended for
the final processing of dental materials. Depending on the abrasiveness of
the grain, corundum-filled tools are used both for pre-treatment of the
surface (abrasives) and for finishing grinding (polishes). The binding and
forming element in corundum tools is a ceramic mass, which can vary in
degree of rigidity. Synthetic resins are used to fix abrasive grains in
corundum separation discs, elastic silicone ligament is used in polishing
tools.
46.
47.
• Burs with silicone-carbide filling.• Tools with a working part made of silicone carbide (SiC) with varying
degrees of granularity of the filling are used in clinical and laboratory
practice in the form of abrasives and polishes for leveling and grinding
dental structures (Fig. 3.83). Ceramics, silicone and synthetic resins serve
as a binding matrix in silicone carbide tools, as well as in corundum tools,
some instruments also use a soft magnesite ligament. Silicone carbide
tools are used for processing dental tissues, ceramics, metal alloys and
acrylic plastics.
48.
49.
• Burs with a sandstone coating.• Sandstone abrasive stones (SiO2) as part of a synthetic binder are
produced with fine–grained and medium-grained silicate filling for
finishing polishing, and coarse-grained filling for pretreatment. Sandstone
tools are mainly used in laboratory practice for grinding plastic products,
metal structures and composites.
50.
51.
• Tools with silicone coating.• Silicone-coated instruments are manufactured on the basis of highmolecular organosilicon compounds with the general chemical formula [O-Si(R2)-O-]n. Silicone rubbers are non-toxic, resistant to aggressive
chemical environments and thermally resistant, which allows the use of
silicone polishes both at the dental reception and in the dental laboratory.
The scope of application of silicone tools: final processing of ceramics,
precious and base metals, restorations of composites and amalgam,
plaque removal and enamel polishing.
52.
53.
• Tools with rubber coating.• The working part of rubber polishes is represented by high-quality
vulcanized thermo- and wear-resistant rubber. Rubber polishes are used
at the final stages of processing metal structures made of chromium-cobalt
alloys, titanium and precious metal alloys.
54.
55.
• A tool with a ceramic coating of the working part.• Tools with ceramic coating of the working part are designed for highspeed processing of soft tissues of the oral cavity. Tissue resection is
accompanied by the effect of coagulation, which reduces bleeding in the
preparation area. A ceramic trimmer is used to remove hyperplastic
gums, expose retentive teeth and separate inter-root granulations; also,
this tool is used in orthopedic dentistry to open the dental sulcus when
taking impressions.
56.
57.
Asepsis.Asepsis is a system for preventing infection from entering the wound during
operations, preventing the development of nosocomial infection. Asepsis
includes a set of measures to ensure the sterilisation of instruments, materials
and compliance with the rules during operations and invasive surgical
manipulations.
58.
Antiseptics.Antiseptics is a system of measures aimed at the destruction of microorganisms in
the wound, pathological focus, organs and tissues, as well as in the patient's body as
a whole, using mechanical and physical methods of exposure, active chemicals and
biological factors.
Mechanical antiseptics is the destruction of microorganisms by mechanical methods,
that is, the removal of areas of non-viable tissues, blood clots, purulent exudate.
Mechanical methods are fundamental - if they are not used, all other methods are not
effective.
Physical antiseptics are methods that create unfavourable conditions in the wound
for the development of bacteria and the absorption of toxins and tissue breakdown
products.
Chemical antiseptics is the destruction of microorganisms in a wound, a pathological
focus or the patient's body with the help of various chemicals.
Biological antiseptics is the use of biological preparations acting both directly on
microorganisms and their toxins, and acting through a macroorganism.
59.
Desinfection.• Disinfection - (French. Des-destruction, inficio - infection) is a set of methods,
methods and means of complete, partial or selective destruction (killing) of
potentially pathogenic microorganisms for humans. During disinfection, bacteria,
viruses, fungi are destroyed, but bacterial spores are not destroyed.
• There are five main disinfection methods:
• 1) Mechanical - wet cleaning, washing, dust removal, washing clothes, air
filtration, hand washing, whitewashing, painting of premises.
• 2) Physical - the effect of high temperatures, UV irradiation, boiling, the effect of
hot air. The principles that are laid down in the device of devices and devices for
disinfection and sterilisation.
• 3) Biological - used for disinfection of sewage, garbage. It is based on antagonistic
relationships of microorganisms.
• 4) Chemical - exposure to disinfectants by wiping, irrigation, soaking, falling
asleep.
• 5) Combined - all of the above methods in various combinations
60.
Sterilisation.Sterilisation is the complete destruction of microorganisms and their spores on or in the sterilised
object.
Classification of sterilisation methods:
According to the obligate state of the sterilising agent:
► Liquid methods;
► using gaseous substances;
► plasma sterilisation;
► using radiation.
By the factor of exposure to the sterilised object:
► penetrating or volumetric (destroy the protein of microorganisms);
► having a surface effect.
According to the method of exposure to the sterilised object:
► Chemical;
► Physical;
► Combined.
61.
Liquid sterilisation• Chemical. This type includes easy-to-use methods of soaking, processing tools
in solutions [for example, 3; 6% solution of hydrogen peroxide (hydrogen
peroxide), salts of hypochlorous acid, 1-3% solution of chloramine, etc.].
Solutions can also be used for processing casts, during ultrasonic processing.
The advantages of the method are the possibility of processing internal
channels of small diameter, low processing temperature. The disadvantages of
the method are: surface exposure, the need to comply with safety regulations,
the duration of treatment (at least 10 hours), the mandatory conduct of several
washings, harmful effects on personnel, the problem of waste disposal.
• Thermal. Sterilization of all-metal dental instruments (burs, needles,
corkscrews, hooks, reusable syringes, etc.), materials can be carried out by
boiling in distilled water with the addition of 1-2% sodium bicarbonate
solution for at least 30 minutes. The method is penetrating, environmentally
friendly. However, the duration of the procedure, the impossibility of boiling
sharp cutting tools limit its use. Sterilization of dental tips can be carried out
by boiling for 1 hour in vaseline oil with the addition of a 2% solution of oxyquinoline followed by centrifugation. The method is reliable, penetrating, but
long-lasting and requires special equipment.
62.
Gas sterilisation• Chemical. Gas sterilization with ethylene oxide. The sterilized object is kept in a gas environment for 1 hour,
after which it is necessary to ventilate the room for 10 hours. The reliability of the method is very high (100%
sterilization). The method is penetrating, has high productivity, as it is carried out centrally, in large batches
of the sterilized object. The method has no restrictions on the materials of the sterilized object. Sterilization
can be carried out in a package. All disposable tools undergo this treatment. The disadvantages of the
method are the use of highly toxic gas, which can have a harmful effect on the environment, the possibility of
toxic precipitation on surfaces after treatment, and the duration of the procedure.
• Ozone sterilization. The object is kept in an ozone atmosphere for 1.5 hours (for example, in the SS-5
apparatus). The method has no restrictions on the materials of the sterilized object. However, a large amount
of ozone is toxic, and the duration of the process is a disadvantage of this method.
• Thermal. The dry-burning method is the most common in dentistry, as it is easy to use, environmentally
friendly, and allows the processing of an object in a package. However, not all instruments can be sterilized
by this method. The object is kept at a temperature of 180 ° C for 1 hour. The dry-burning cabinet cannot be
filled (low reliability). High temperature requires compliance with safety regulations.
• Steam (autoclaving) method. The sterilizing agent in this case is steam heated to 120 °C at a pressure of 1.1
atm for 12 minutes, to 134 °C for 4 minutes. The method is penetrating, environmentally friendly, the speed
is high. However, high temperature and humidity limit its use for cutting tools and require compliance with
safety regulations. Recently, the method has become widespread.
• The glasperlene method is also penetrating, but is used only for the sterilization of small instruments. The
working part of the tools is immersed in a medium heated to 240-270 ° C for a few seconds.
63.
Sterelisation with the radiation• Radiation sterilization. The use of penetrating ionizing radiation, the source of
which is 60Co, is possible only in industrial conditions due to the risk of
personnel exposure. The method has the same positive characteristics as gas
(ethylene oxide).
• Ultraviolet sterilization. The use of ultraviolet radiation is possible only for
open surfaces of the sterilized object. The method is simple, but during
prolonged operation of the device, a large amount of ozone is released.
• Infrared sterilization. Infrared radiation is also used to sterilize exposed
surfaces (surface exposure) the sterilized object, but the method gives heating
of the surfaces.
• Ultrahigh frequency sterilization. Ultrahigh frequency currents
(electromagnetic radiation) have a sterilizing effect. The method is ineffective,
harmful to personnel, and the effect on the sterilized object is short-lived.
64.
Sterilisation control.Sterilisation control is carried out by one of the following methods:
selective microbiological control (flushing is sown on nutrient media);
the use of chemical indicators (indicator strips that change colour at a certain
temperature);
The use of biological indicators (strips with test microbial cultures, which after
sterilisation are placed in nutrient media, in the presence of growth, the entire
batch is rejected).
65.
Ergonomic in dentistry.Ergonomics (from Greek ergon - science and nomos - law) is a complex
scientific discipline based on the knowledge of physiology, human
psychology, using the data of anatomy, toxicology, hygiene, achievements of
technical sciences in order to create optimal working conditions, which
makes it possible to make a medical worker highly productive and preserve
his strength and health.
66.
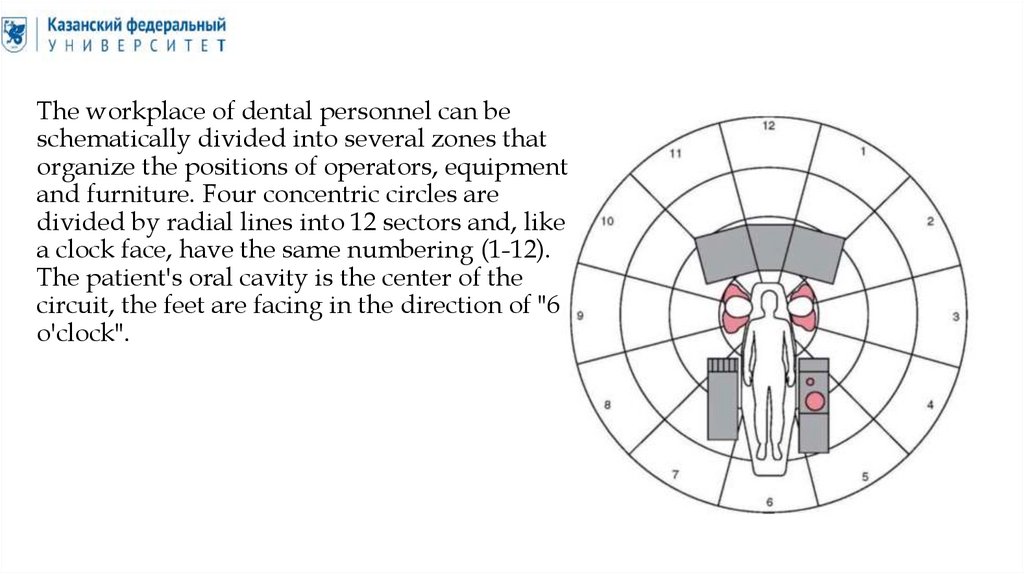
The workplace of dental personnel can beschematically divided into several zones that
organize the positions of operators, equipment
and furniture. Four concentric circles are
divided by radial lines into 12 sectors and, like
a clock face, have the same numbering (1-12).
The patient's oral cavity is the center of the
circuit, the feet are facing in the direction of "6
o'clock".
67.
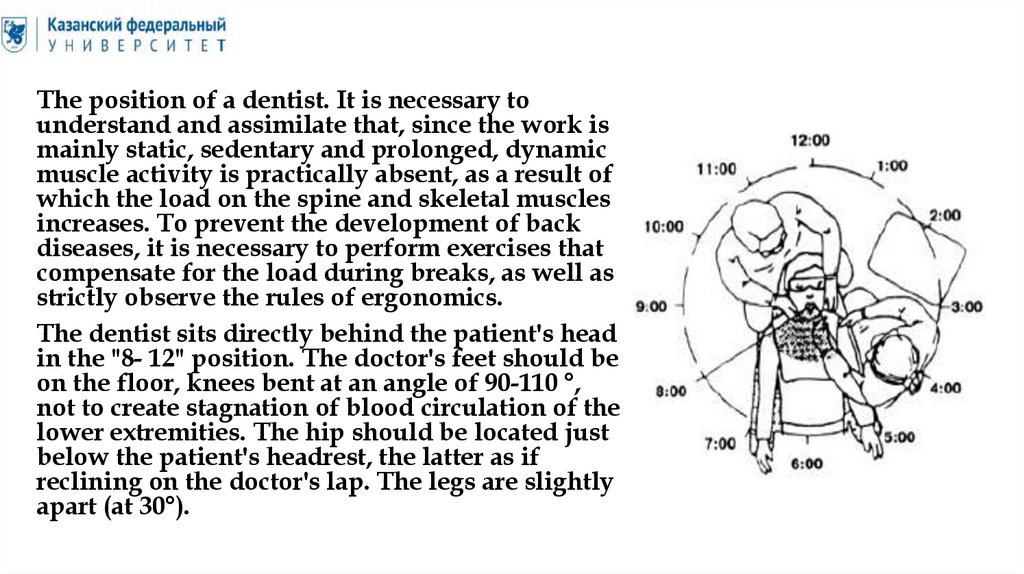
The position of a dentist. It is necessary tounderstand and assimilate that, since the work is
mainly static, sedentary and prolonged, dynamic
muscle activity is practically absent, as a result of
which the load on the spine and skeletal muscles
increases. To prevent the development of back
diseases, it is necessary to perform exercises that
compensate for the load during breaks, as well as
strictly observe the rules of ergonomics.
The dentist sits directly behind the patient's head
in the "8- 12" position. The doctor's feet should be
on the floor, knees bent at an angle of 90-110 °,
not to create stagnation of blood circulation of the
lower extremities. The hip should be located just
below the patient's headrest, the latter as if
reclining on the doctor's lap. The legs are slightly
apart (at 30°).
68.
The "static" zone is located between positions "12" and "2". It is multifunctional.Usually no one sits here, except in cases when the technology is used "in six
hands" (when manipulating several lasers at the same time or with some
restoration technologies).
In the "9" position, the doctor treats the upper jaw area both with and without a
mirror. The mirror is held in the left hand, which is supported on the patient's
forehead. If the doctor deals with the lateral (vestibular or oral) surfaces of
premolars and molars, then the patient's head must be rotated in such a way as
to see these surfaces directly. The equipment for removing fluid from the oral
cavity is placed on the tilted side of the patient's head.
In the "10" position, the doctor works with the teeth located on the left in the
lower jaw, as well as in the entire lower row.
In the "11" position, the dentist works with the teeth located on the right in the
lower jaw, and with the mirror - and on the right in the upper jaw.
In the "12" position, the doctor treats the teeth in the upper and lower dentition.
They work with oral surfaces using a mirror. Hygienists often work in this
position. When working with vestibular and oral surfaces, the patient's head
tilts to the left or right.
69.
There are certain principles of the "doctor-patient" position.► The doctor should sit under the patient's headrest, i.e. the patient's head is above
the doctor's abdomen.
► The dentist's elbows should be positioned at the height of the patient's head.
The elbows should always be as close to the body as possible, otherwise the load
on the spine and joints of the upper extremities increases.
► When moving in the direction of the patient, the doctor needs to turn his head
and shoulders at the same time; the number of independent turns of the head
should be limited to a minimum, since this increases the load on the cervical spine.
To avoid this mistake, it is necessary to place the patient's head in a position that
mainly satisfies the doctor, naturally observing all safety rules.
► The dentist's hands should always be fixed when working: the left hand rests on
the patient's head, the right hand has a fulcrum in the patient's oral cavity.
► The distance between the doctor's eyes and the patient's face should be
approximately 40-50 cm.
The correct fit of the doctor during work involves the formation of blunt angles
(between the ankle and the instep, under the knee, in the hip joint, between the
shoulder and forearm).
70.
The position of "doctor-assistant". When working "in four hands", the assistant islocated in the "3" or "9" position, and can work standing or sitting. When working
while sitting, it is necessary to adjust the assistant's chair so that with the feet
mounted on the foot support, the hips are parallel to the floor, and the assistant
himself is 10-15 cm above the doctor's level for a convenient overview of the
operating field, while the neck and back should be straightened. A prerequisite
for the assistant's work is the convenient location of the drawers of the mobile
table to provide the doctor with the necessary tools and materials. When working
with the tips of a vacuum cleaner or saliva suction, it is necessary to install them
in such a way that they do not cover the doctor's working field. All surfaces that
the assistant or the doctor will touch must be insulated with disposable coatings.
The assistant's desk is usually located on his right hand. The next zone is the
"transfer zone" located between zones "5" and "8". In it, the assistant passes the
necessary tools to the doctor.
The main attention in the treatment process is directed to the patient's oral cavity,
therefore, the most frequently used materials and tools should be rationally
arranged around it. There are two workspaces: large and small.
71.
• A large workspace is an area 50 cm away fromthe body. In order to take a tool from this area,
the arm is fully extended, while the gaze is
taken away from the working field, so this
area is not entirely favorable for postponing
the most commonly used tools.
• A small workspace is an area that is up to 25
cm away from the body. The instrument is
taken by touch and without a wide
withdrawal of the hand. This zone is most
favorable for the location of the tools used
most often.
72.
Thank you for yourattention .