 medicine
medicineSimilar presentations:










PowerPoint Handout: Lab 3, Anterior and Medial Thigh
1.
PowerPoint Handout: Lab 3, Anterior and Medial ThighSlide Title
Slide Number
Slide Title
Slide Number
Pelvis Osteology
Slide 2
Medial Compartment Muscles
Slide 16
Thigh Fascia: Fascia Lata and Iliotibial Band
Slide 3
Adductor Muscles: Clinical Anatomy
Slide 17
Thigh Fascia: Iliotibial Band
Slide 4
Obturator Artery and Nerve
Slide 18
Thigh Compartments
Slide 5
Adductor Canal
Slide 19
Thigh Fascia: Saphenous Opening & Saphenous Vein
Slide 6
Femoral Artery
Slide 20
Femoral Triangle
Slide 7
Deep Femoral Artery
Slide 21
Inguinal Ligament & Subinguinal Space
Slide 8
Medial Femoral Circumflex Artery
Slide 22
Femoral Sheath
Slide 9
Lumbar Plexus: Overview
Slide 23
Femoral Ring and Femoral Hernia
Slide 10
Slide 24
Femoral Artery & Vein Cannulation
Lumbar Plexus: Iliohypogastric n. and
Ilioinguinal n.
Slide 11
Lumbar Plexus: Genitofemoral n.
Slide 25
Anterior Compartment Muscles: Flexors of the Hip
Slide 12
Lumbar Plexus: Lateral Femoral Cutaneous n.
Slide 26
Psoas Abscess
Slide 13
Lumbar Plexus: Femora n., Obturator n., and
Lumbosacral Trunk
Slide 27
Anterior Compartment Muscles: Extensors of the
Knee
Slide 14
Avulsion Fracture: AIIS
Slide 15
2.
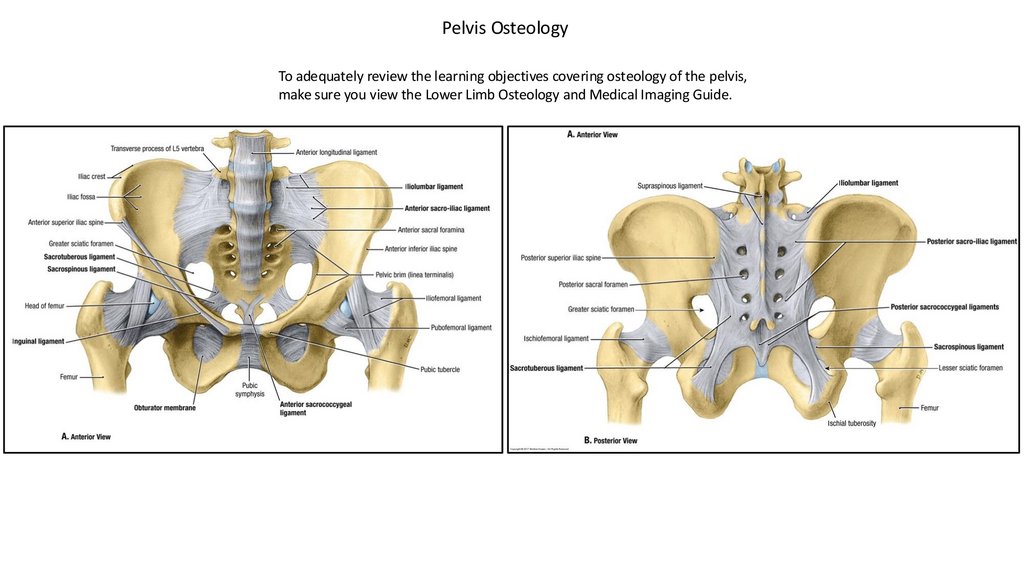
Pelvis OsteologyTo adequately review the learning objectives covering osteology of the pelvis,
make sure you view the Lower Limb Osteology and Medical Imaging Guide.
3.
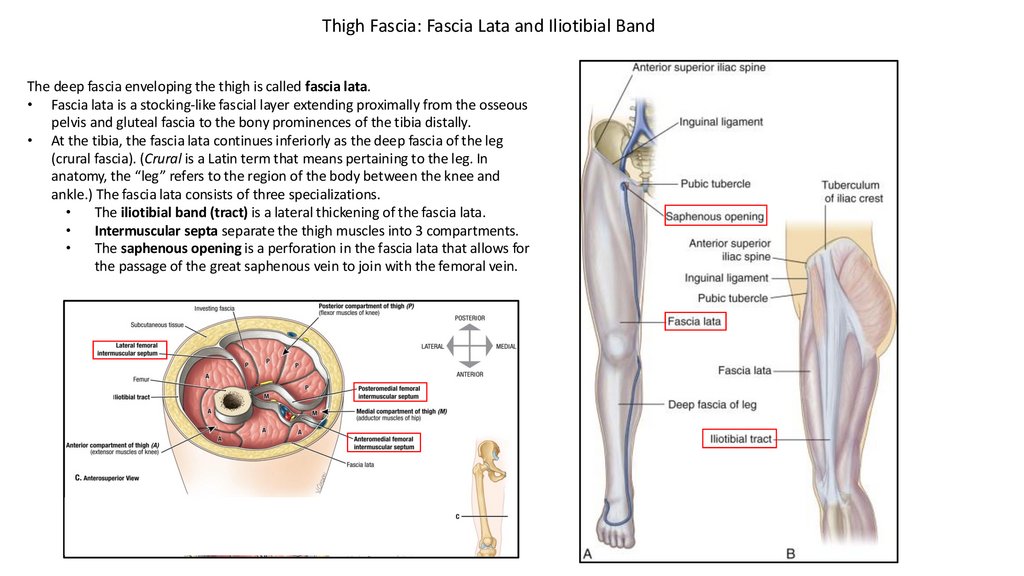
Thigh Fascia: Fascia Lata and Iliotibial BandThe deep fascia enveloping the thigh is called fascia lata.
• Fascia lata is a stocking-like fascial layer extending proximally from the osseous
pelvis and gluteal fascia to the bony prominences of the tibia distally.
• At the tibia, the fascia lata continues inferiorly as the deep fascia of the leg
(crural fascia). (Crural is a Latin term that means pertaining to the leg. In
anatomy, the “leg” refers to the region of the body between the knee and
ankle.) The fascia lata consists of three specializations.
The iliotibial band (tract) is a lateral thickening of the fascia lata.
Intermuscular septa separate the thigh muscles into 3 compartments.
The saphenous opening is a perforation in the fascia lata that allows for
the passage of the great saphenous vein to join with the femoral vein.
4.
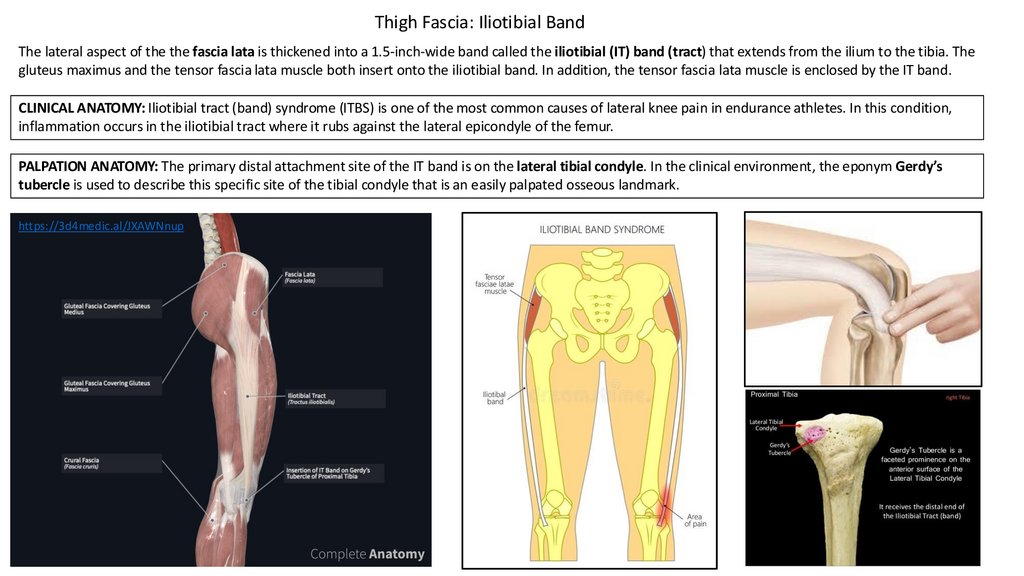
Thigh Fascia: Iliotibial BandThe lateral aspect of the the fascia lata is thickened into a 1.5-inch-wide band called the iliotibial (IT) band (tract) that extends from the ilium to the tibia. The
gluteus maximus and the tensor fascia lata muscle both insert onto the iliotibial band. In addition, the tensor fascia lata muscle is enclosed by the IT band.
CLINICAL ANATOMY: Iliotibial tract (band) syndrome (ITBS) is one of the most common causes of lateral knee pain in endurance athletes. In this condition,
inflammation occurs in the iliotibial tract where it rubs against the lateral epicondyle of the femur.
PALPATION ANATOMY: The primary distal attachment site of the IT band is on the lateral tibial condyle. In the clinical environment, the eponym Gerdy’s
tubercle is used to describe this specific site of the tibial condyle that is an easily palpated osseous landmark.
https://3d4medic.al/JXAWNnup
5.
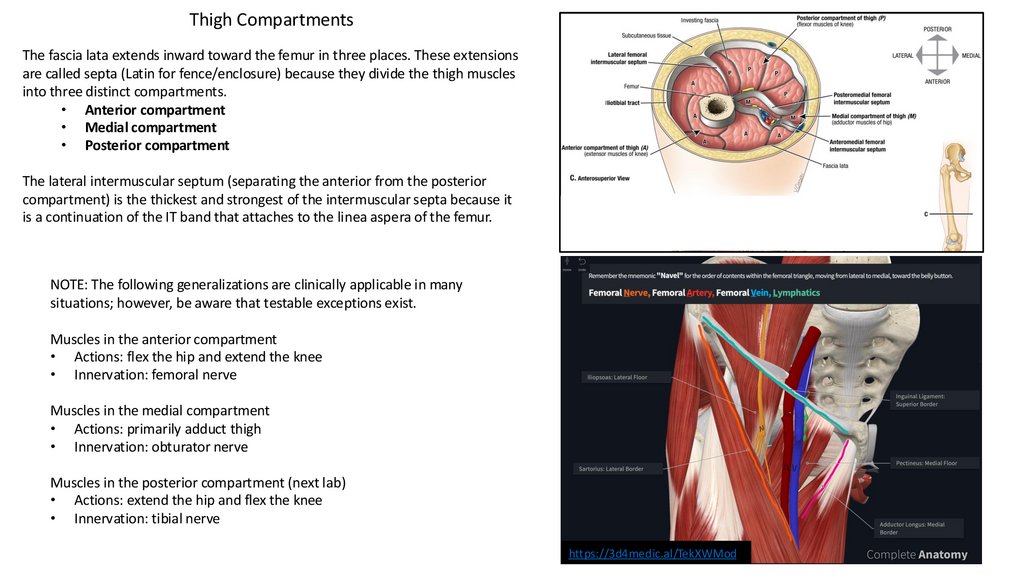
Thigh CompartmentsThe fascia lata extends inward toward the femur in three places. These extensions
are called septa (Latin for fence/enclosure) because they divide the thigh muscles
into three distinct compartments.
• Anterior compartment
• Medial compartment
• Posterior compartment
The lateral intermuscular septum (separating the anterior from the posterior
compartment) is the thickest and strongest of the intermuscular septa because it
is a continuation of the IT band that attaches to the linea aspera of the femur.
NOTE: The following generalizations are clinically applicable in many
situations; however, be aware that testable exceptions exist.
Muscles in the anterior compartment
• Actions: flex the hip and extend the knee
• Innervation: femoral nerve
Muscles in the medial compartment
• Actions: primarily adduct thigh
• Innervation: obturator nerve
Muscles in the posterior compartment (next lab)
• Actions: extend the hip and flex the knee
• Innervation: tibial nerve
https://3d4medic.al/TekXWMod
6.
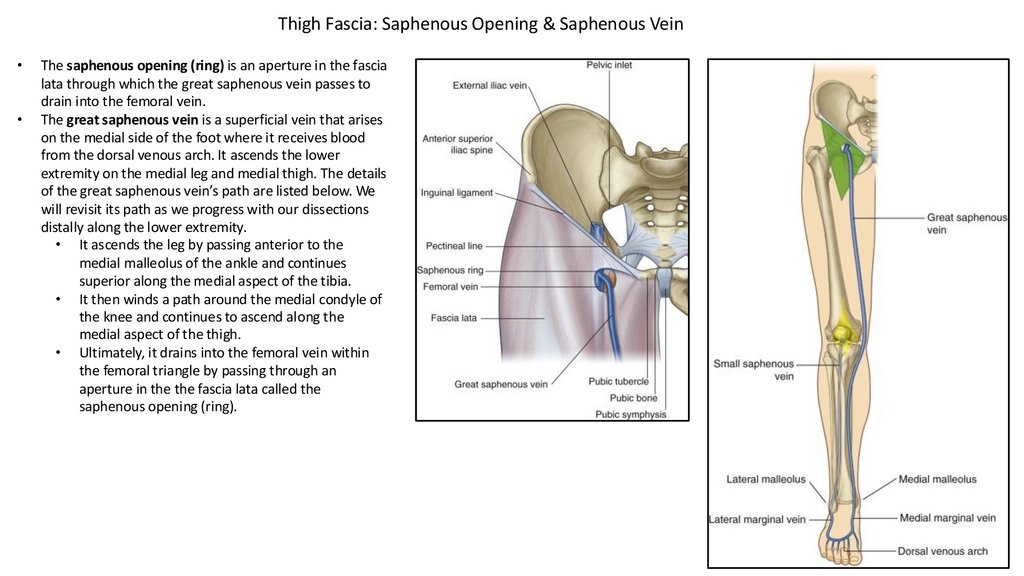
Thigh Fascia: Saphenous Opening & Saphenous VeinThe saphenous opening (ring) is an aperture in the fascia
lata through which the great saphenous vein passes to
drain into the femoral vein.
The great saphenous vein is a superficial vein that arises
on the medial side of the foot where it receives blood
from the dorsal venous arch. It ascends the lower
extremity on the medial leg and medial thigh. The details
of the great saphenous vein’s path are listed below. We
will revisit its path as we progress with our dissections
distally along the lower extremity.
• It ascends the leg by passing anterior to the
medial malleolus of the ankle and continues
superior along the medial aspect of the tibia.
• It then winds a path around the medial condyle of
the knee and continues to ascend along the
medial aspect of the thigh.
• Ultimately, it drains into the femoral vein within
the femoral triangle by passing through an
aperture in the the fascia lata called the
saphenous opening (ring).
7.
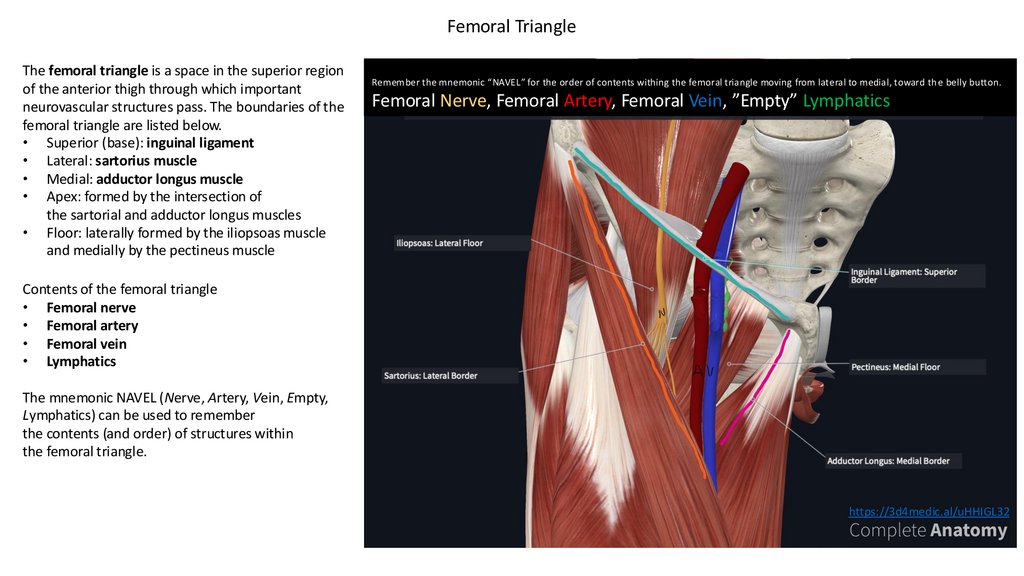
Femoral TriangleThe femoral triangle is a space in the superior region
of the anterior thigh through which important
neurovascular structures pass. The boundaries of the
femoral triangle are listed below.
• Superior (base): inguinal ligament
• Lateral: sartorius muscle
• Medial: adductor longus muscle
• Apex: formed by the intersection of
the sartorial and adductor longus muscles
• Floor: laterally formed by the iliopsoas muscle
and medially by the pectineus muscle
Remember the mnemonic “NAVEL” for the order of contents withing the femoral triangle moving from lateral to medial, toward th e belly button.
Femoral Nerve, Femoral Artery, Femoral Vein, ”Empty” Lymphatics
Contents of the femoral triangle
• Femoral nerve
• Femoral artery
• Femoral vein
• Lymphatics
The mnemonic NAVEL (Nerve, Artery, Vein, Empty,
Lymphatics) can be used to remember
the contents (and order) of structures within
the femoral triangle.
https://3d4medic.al/uHHIGL32
8.
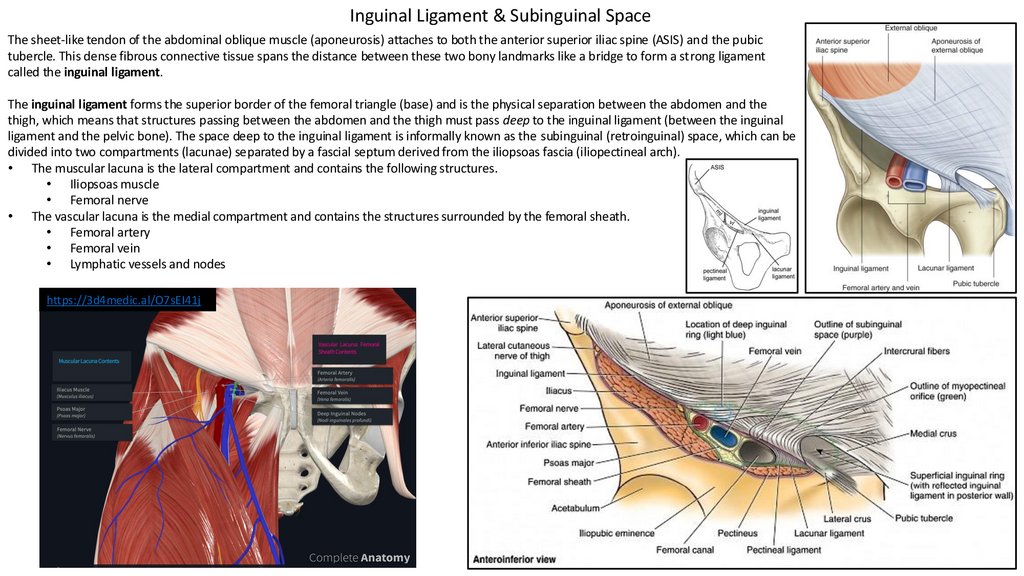
Inguinal Ligament & Subinguinal SpaceThe sheet-like tendon of the abdominal oblique muscle (aponeurosis) attaches to both the anterior superior iliac spine (ASIS) and the pubic
tubercle. This dense fibrous connective tissue spans the distance between these two bony landmarks like a bridge to form a strong ligament
called the inguinal ligament.
The inguinal ligament forms the superior border of the femoral triangle (base) and is the physical separation between the abdomen and the
thigh, which means that structures passing between the abdomen and the thigh must pass deep to the inguinal ligament (between the inguinal
ligament and the pelvic bone). The space deep to the inguinal ligament is informally known as the subinguinal (retroinguinal) space, which can be
divided into two compartments (lacunae) separated by a fascial septum derived from the iliopsoas fascia (iliopectineal arch).
• The muscular lacuna is the lateral compartment and contains the following structures.
• Iliopsoas muscle
• Femoral nerve
• The vascular lacuna is the medial compartment and contains the structures surrounded by the femoral sheath.
• Femoral artery
• Femoral vein
• Lymphatic vessels and nodes
https://3d4medic.al/O7sEI41j
9.
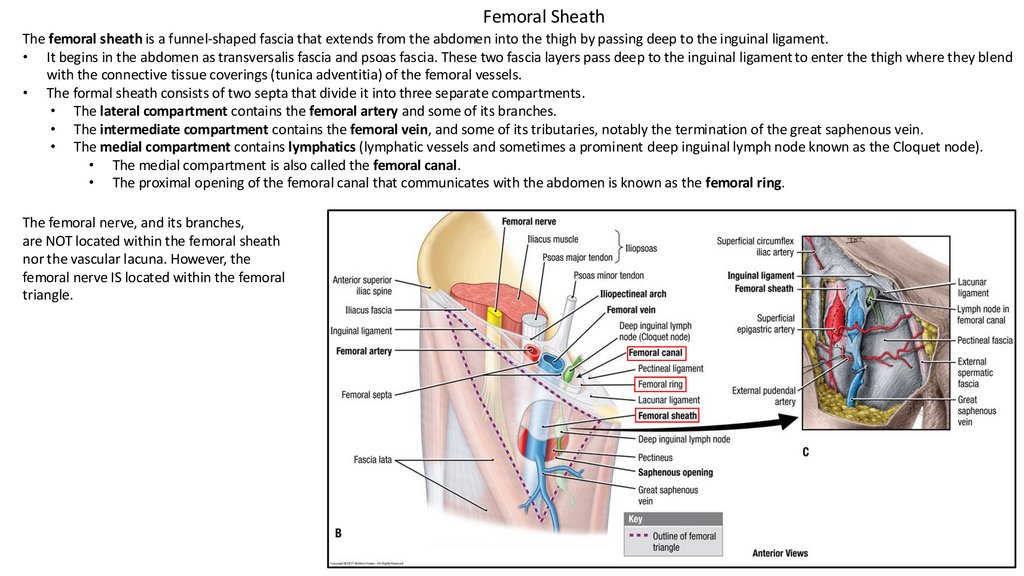
Femoral SheathThe femoral sheath is a funnel-shaped fascia that extends from the abdomen into the thigh by passing deep to the inguinal ligament.
• It begins in the abdomen as transversalis fascia and psoas fascia. These two fascia layers pass deep to the inguinal ligament to enter the thigh where they blend
with the connective tissue coverings (tunica adventitia) of the femoral vessels.
• The formal sheath consists of two septa that divide it into three separate compartments.
• The lateral compartment contains the femoral artery and some of its branches.
• The intermediate compartment contains the femoral vein, and some of its tributaries, notably the termination of the great saphenous vein.
• The medial compartment contains lymphatics (lymphatic vessels and sometimes a prominent deep inguinal lymph node known as the Cloquet node).
• The medial compartment is also called the femoral canal.
• The proximal opening of the femoral canal that communicates with the abdomen is known as the femoral ring.
The femoral nerve, and its branches,
are NOT located within the femoral sheath
nor the vascular lacuna. However, the
femoral nerve IS located within the femoral
triangle.
10.
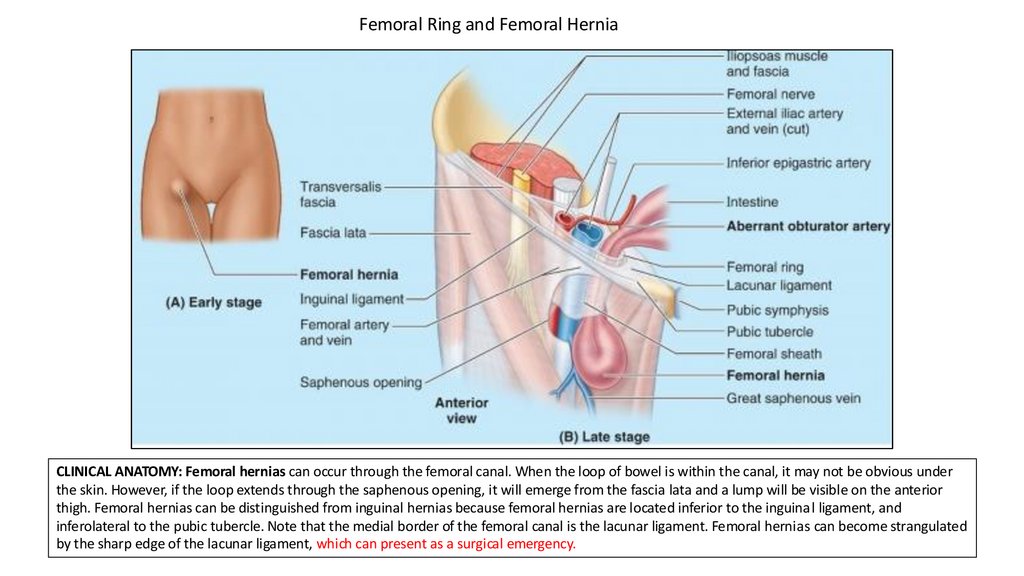
Femoral Ring and Femoral HerniaCLINICAL ANATOMY: Femoral hernias can occur through the femoral canal. When the loop of bowel is within the canal, it may not be obvious under
the skin. However, if the loop extends through the saphenous opening, it will emerge from the fascia lata and a lump will be visible on the anterior
thigh. Femoral hernias can be distinguished from inguinal hernias because femoral hernias are located inferior to the inguinal ligament, and
inferolateral to the pubic tubercle. Note that the medial border of the femoral canal is the lacunar ligament. Femoral hernias can become strangulated
by the sharp edge of the lacunar ligament, which can present as a surgical emergency.
11.
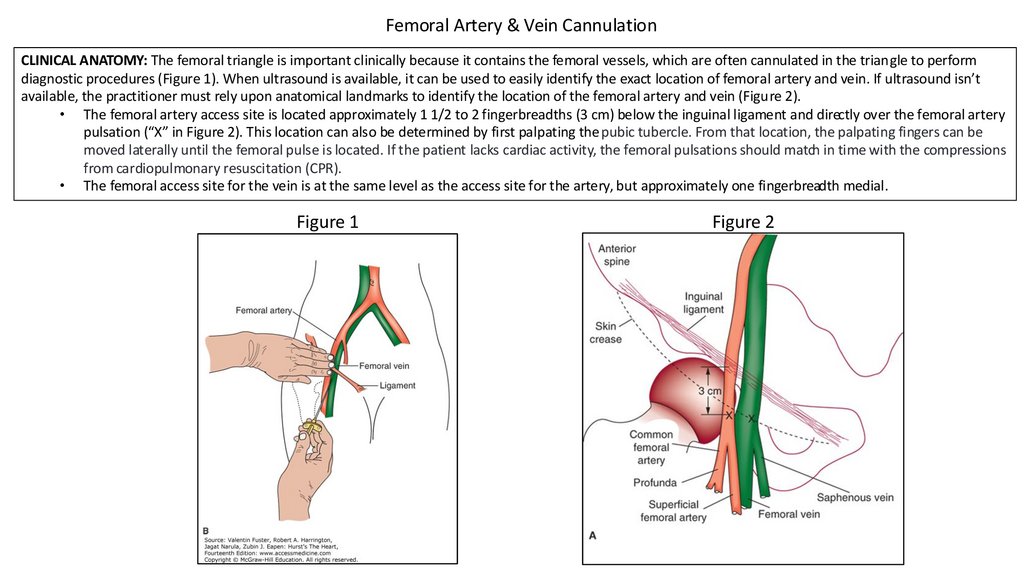
Femoral Artery & Vein CannulationCLINICAL ANATOMY: The femoral triangle is important clinically because it contains the femoral vessels, which are often cannulated in the triangle to perform
diagnostic procedures (Figure 1). When ultrasound is available, it can be used to easily identify the exact location of femoral artery and vein. If ultrasound isn’t
available, the practitioner must rely upon anatomical landmarks to identify the location of the femoral artery and vein (Figure 2).
• The femoral artery access site is located approximately 1 1/2 to 2 fingerbreadths (3 cm) below the inguinal ligament and directly over the femoral artery
pulsation (“X” in Figure 2). This location can also be determined by first palpating the pubic tubercle. From that location, the palpating fingers can be
moved laterally until the femoral pulse is located. If the patient lacks cardiac activity, the femoral pulsations should match in time with the compressions
from cardiopulmonary resuscitation (CPR).
• The femoral access site for the vein is at the same level as the access site for the artery, but approximately one fingerbreadth medial.
Figure 1
Figure 2
12.
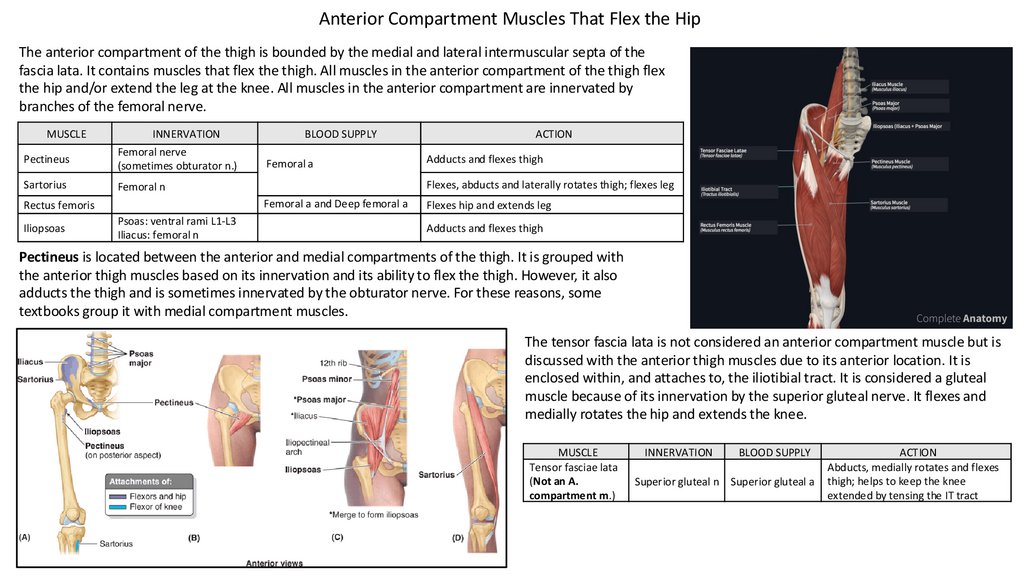
Anterior Compartment Muscles That Flex the HipThe anterior compartment of the thigh is bounded by the medial and lateral intermuscular septa of the
fascia lata. It contains muscles that flex the thigh. All muscles in the anterior compartment of the thigh flex
the hip and/or extend the leg at the knee. All muscles in the anterior compartment are innervated by
branches of the femoral nerve.
MUSCLE
INNERVATION
Pectineus
Femoral nerve
(sometimes obturator n.)
Sartorius
Femoral n
Femoral a
Psoas: ventral rami L1-L3
Iliacus: femoral n
ACTION
Adducts and flexes thigh
Flexes, abducts and laterally rotates thigh; flexes leg
Femoral a and Deep femoral a
Rectus femoris
Iliopsoas
BLOOD SUPPLY
Flexes hip and extends leg
Adducts and flexes thigh
Pectineus is located between the anterior and medial compartments of the thigh. It is grouped with
the anterior thigh muscles based on its innervation and its ability to flex the thigh. However, it also
adducts the thigh and is sometimes innervated by the obturator nerve. For these reasons, some
textbooks group it with medial compartment muscles.
The tensor fascia lata is not considered an anterior compartment muscle but is
discussed with the anterior thigh muscles due to its anterior location. It is
enclosed within, and attaches to, the iliotibial tract. It is considered a gluteal
muscle because of its innervation by the superior gluteal nerve. It flexes and
medially rotates the hip and extends the knee.
MUSCLE
Tensor fasciae lata
(Not an A.
compartment m.)
INNERVATION
BLOOD SUPPLY
Superior gluteal n Superior gluteal a
ACTION
Abducts, medially rotates and flexes
thigh; helps to keep the knee
extended by tensing the IT tract
13.
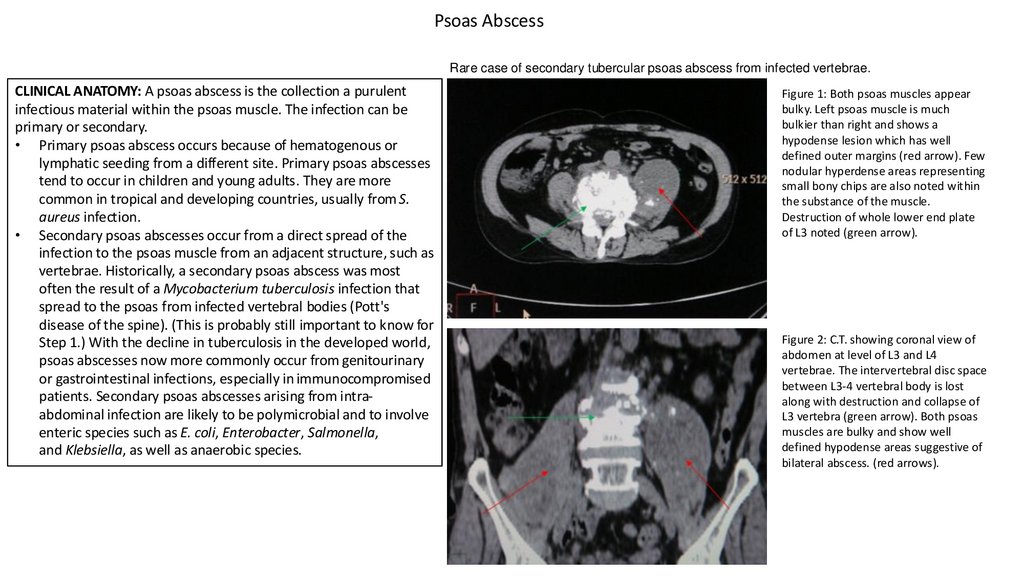
Psoas AbscessRare case of secondary tubercular psoas abscess from infected vertebrae.
CLINICAL ANATOMY: A psoas abscess is the collection a purulent
infectious material within the psoas muscle. The infection can be
primary or secondary.
• Primary psoas abscess occurs because of hematogenous or
lymphatic seeding from a different site. Primary psoas abscesses
tend to occur in children and young adults. They are more
common in tropical and developing countries, usually from S.
aureus infection.
• Secondary psoas abscesses occur from a direct spread of the
infection to the psoas muscle from an adjacent structure, such as
vertebrae. Historically, a secondary psoas abscess was most
often the result of a Mycobacterium tuberculosis infection that
spread to the psoas from infected vertebral bodies (Pott's
disease of the spine). (This is probably still important to know for
Step 1.) With the decline in tuberculosis in the developed world,
psoas abscesses now more commonly occur from genitourinary
or gastrointestinal infections, especially in immunocompromised
patients. Secondary psoas abscesses arising from intraabdominal infection are likely to be polymicrobial and to involve
enteric species such as E. coli, Enterobacter, Salmonella,
and Klebsiella, as well as anaerobic species.
Figure 1: Both psoas muscles appear
bulky. Left psoas muscle is much
bulkier than right and shows a
hypodense lesion which has well
defined outer margins (red arrow). Few
nodular hyperdense areas representing
small bony chips are also noted within
the substance of the muscle.
Destruction of whole lower end plate
of L3 noted (green arrow).
Figure 2: C.T. showing coronal view of
abdomen at level of L3 and L4
vertebrae. The intervertebral disc space
between L3-4 vertebral body is lost
along with destruction and collapse of
L3 vertebra (green arrow). Both psoas
muscles are bulky and show well
defined hypodense areas suggestive of
bilateral abscess. (red arrows).
14.
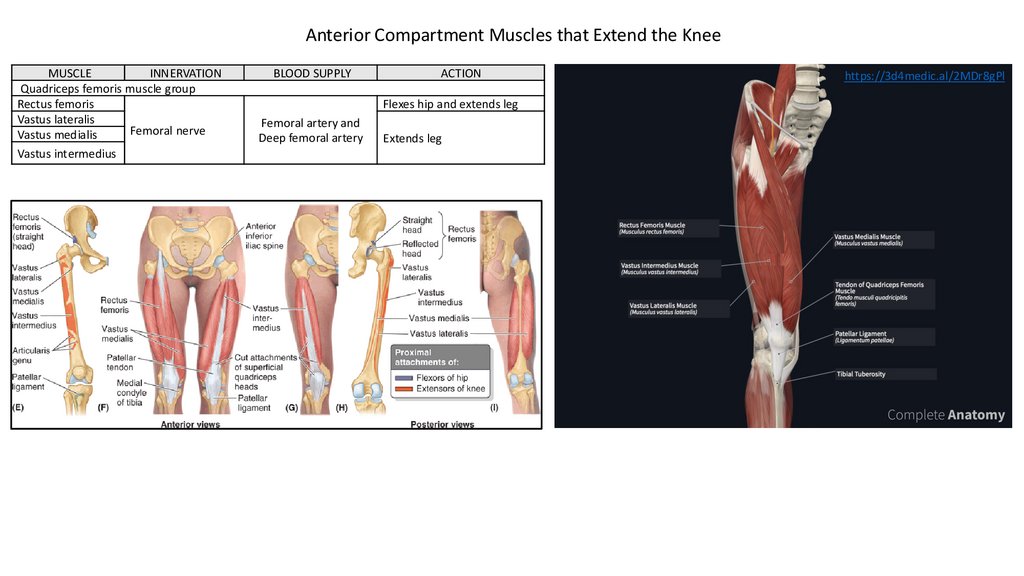
Anterior Compartment Muscles that Extend the KneeMUSCLE
INNERVATION
Quadriceps femoris muscle group
Rectus femoris
Vastus lateralis
Femoral nerve
Vastus medialis
Vastus intermedius
BLOOD SUPPLY
ACTION
Flexes hip and extends leg
Femoral artery and
Deep femoral artery
Extends leg
https://3d4medic.al/2MDr8gPl
15.
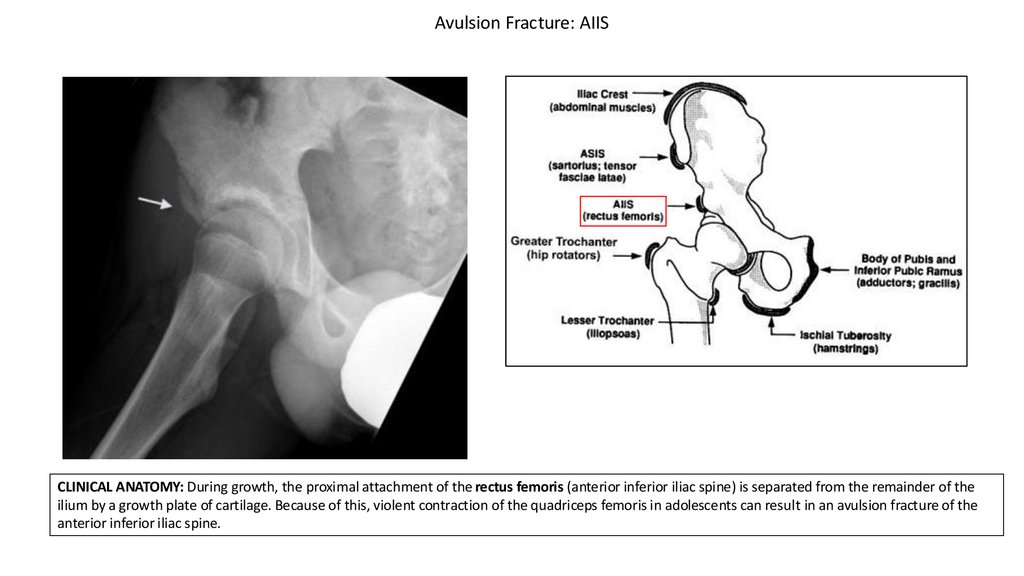
Avulsion Fracture: AIISCLINICAL ANATOMY: During growth, the proximal attachment of the rectus femoris (anterior inferior iliac spine) is separated from the remainder of the
ilium by a growth plate of cartilage. Because of this, violent contraction of the quadriceps femoris in adolescents can result in an avulsion fracture of the
anterior inferior iliac spine.
16.
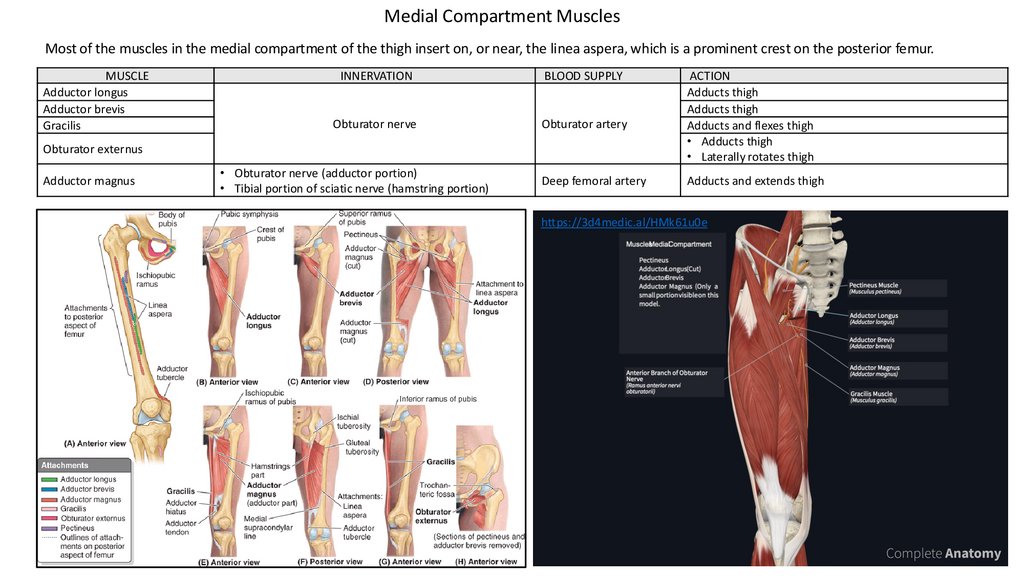
Medial Compartment MusclesMost of the muscles in the medial compartment of the thigh insert on, or near, the linea aspera, which is a prominent crest on the posterior femur.
MUSCLE
Adductor longus
Adductor brevis
Gracilis
INNERVATION
BLOOD SUPPLY
Obturator nerve
Obturator artery
Obturator externus
Adductor magnus
• Obturator nerve (adductor portion)
• Tibial portion of sciatic nerve (hamstring portion)
Deep femoral artery
ACTION
Adducts thigh
Adducts thigh
Adducts and flexes thigh
• Adducts thigh
• Laterally rotates thigh
Adducts and extends thigh
https://3d4medic.al/HMk61u0e
17.
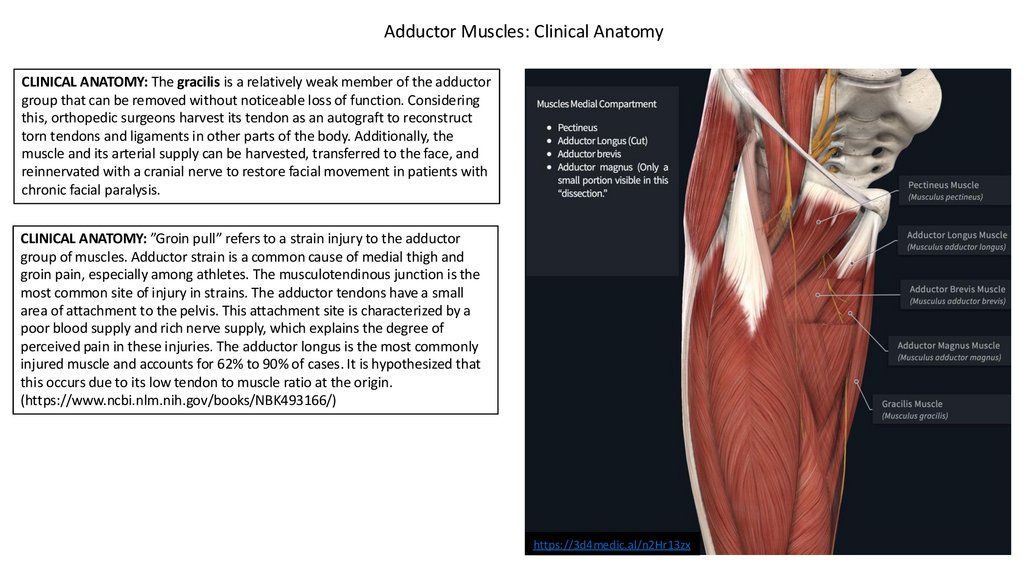
Adductor Muscles: Clinical AnatomyCLINICAL ANATOMY: The gracilis is a relatively weak member of the adductor
group that can be removed without noticeable loss of function. Considering
this, orthopedic surgeons harvest its tendon as an autograft to reconstruct
torn tendons and ligaments in other parts of the body. Additionally, the
muscle and its arterial supply can be harvested, transferred to the face, and
reinnervated with a cranial nerve to restore facial movement in patients with
chronic facial paralysis.
CLINICAL ANATOMY: ”Groin pull” refers to a strain injury to the adductor
group of muscles. Adductor strain is a common cause of medial thigh and
groin pain, especially among athletes. The musculotendinous junction is the
most common site of injury in strains. The adductor tendons have a small
area of attachment to the pelvis. This attachment site is characterized by a
poor blood supply and rich nerve supply, which explains the degree of
perceived pain in these injuries. The adductor longus is the most commonly
injured muscle and accounts for 62% to 90% of cases. It is hypothesized that
this occurs due to its low tendon to muscle ratio at the origin.
(https://www.ncbi.nlm.nih.gov/books/NBK493166/)
https://3d4medic.al/n2Hr13zx
18.
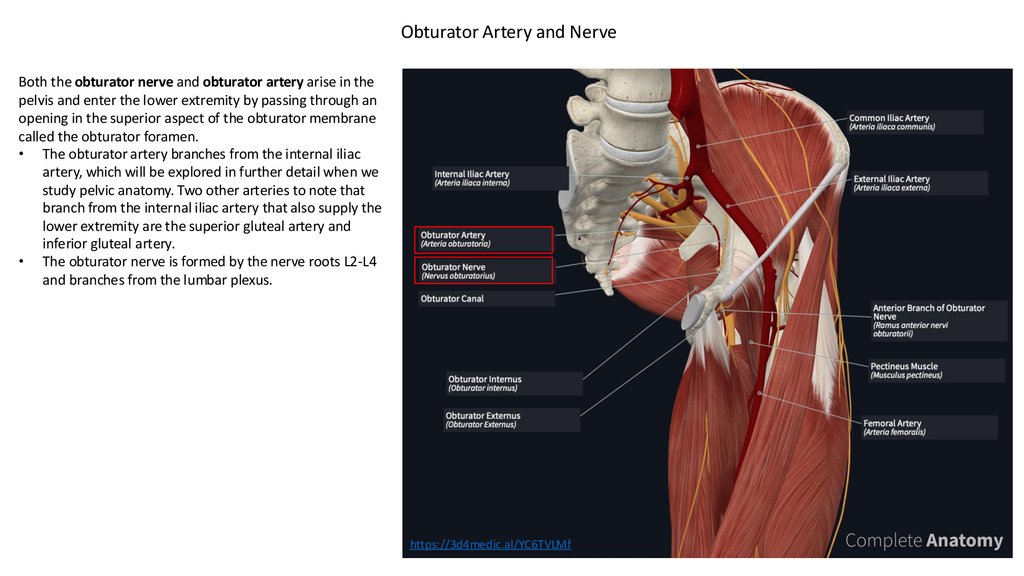
Obturator Artery and NerveBoth the obturator nerve and obturator artery arise in the
pelvis and enter the lower extremity by passing through an
opening in the superior aspect of the obturator membrane
called the obturator foramen.
• The obturator artery branches from the internal iliac
artery, which will be explored in further detail when we
study pelvic anatomy. Two other arteries to note that
branch from the internal iliac artery that also supply the
lower extremity are the superior gluteal artery and
inferior gluteal artery.
• The obturator nerve is formed by the nerve roots L2-L4
and branches from the lumbar plexus.
https://3d4medic.al/YC6TVLMf
19.
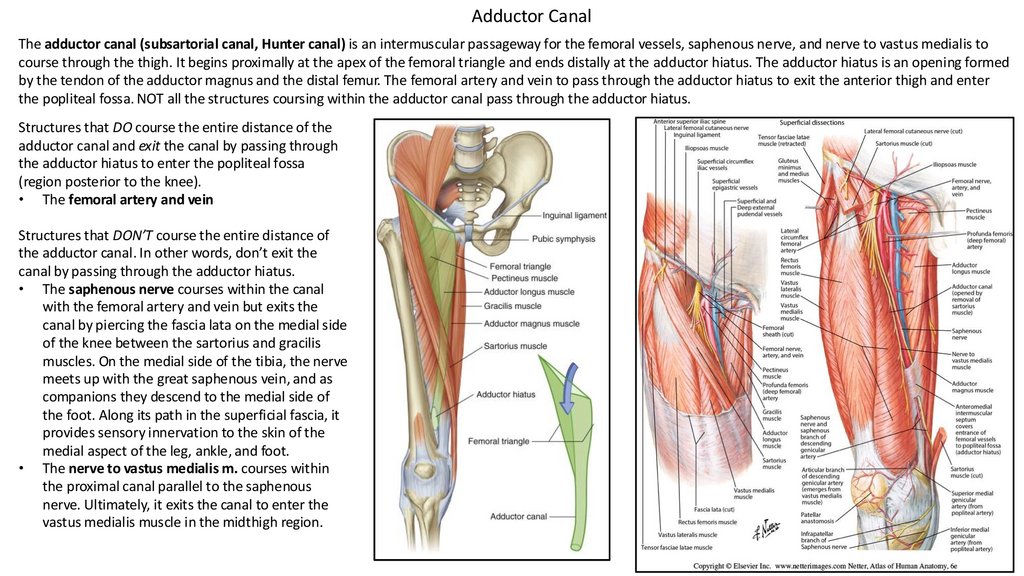
Adductor CanalThe adductor canal (subsartorial canal, Hunter canal) is an intermuscular passageway for the femoral vessels, saphenous nerve, and nerve to vastus medialis to
course through the thigh. It begins proximally at the apex of the femoral triangle and ends distally at the adductor hiatus. The adductor hiatus is an opening formed
by the tendon of the adductor magnus and the distal femur. The femoral artery and vein to pass through the adductor hiatus to exit the anterior thigh and enter
the popliteal fossa. NOT all the structures coursing within the adductor canal pass through the adductor hiatus.
Structures that DO course the entire distance of the
adductor canal and exit the canal by passing through
the adductor hiatus to enter the popliteal fossa
(region posterior to the knee).
• The femoral artery and vein
Structures that DON’T course the entire distance of
the adductor canal. In other words, don’t exit the
canal by passing through the adductor hiatus.
• The saphenous nerve courses within the canal
with the femoral artery and vein but exits the
canal by piercing the fascia lata on the medial side
of the knee between the sartorius and gracilis
muscles. On the medial side of the tibia, the nerve
meets up with the great saphenous vein, and as
companions they descend to the medial side of
the foot. Along its path in the superficial fascia, it
provides sensory innervation to the skin of the
medial aspect of the leg, ankle, and foot.
• The nerve to vastus medialis m. courses within
the proximal canal parallel to the saphenous
nerve. Ultimately, it exits the canal to enter the
vastus medialis muscle in the midthigh region.
20.
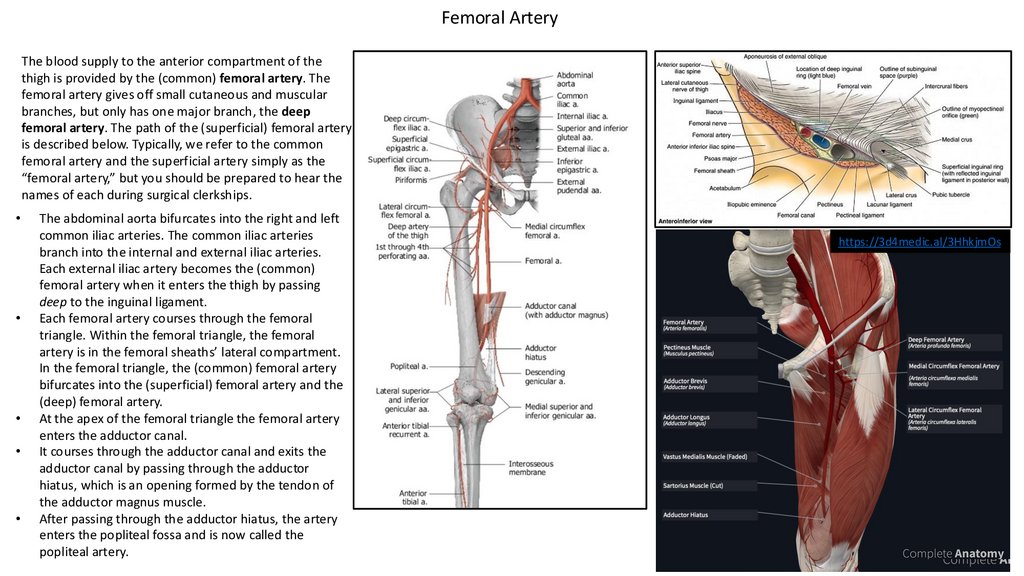
Femoral ArteryThe blood supply to the anterior compartment of the
thigh is provided by the (common) femoral artery. The
femoral artery gives off small cutaneous and muscular
branches, but only has one major branch, the deep
femoral artery. The path of the (superficial) femoral artery
is described below. Typically, we refer to the common
femoral artery and the superficial artery simply as the
“femoral artery,” but you should be prepared to hear the
names of each during surgical clerkships.
The abdominal aorta bifurcates into the right and left
common iliac arteries. The common iliac arteries
branch into the internal and external iliac arteries.
Each external iliac artery becomes the (common)
femoral artery when it enters the thigh by passing
deep to the inguinal ligament.
Each femoral artery courses through the femoral
triangle. Within the femoral triangle, the femoral
artery is in the femoral sheaths’ lateral compartment.
In the femoral triangle, the (common) femoral artery
bifurcates into the (superficial) femoral artery and the
(deep) femoral artery.
At the apex of the femoral triangle the femoral artery
enters the adductor canal.
It courses through the adductor canal and exits the
adductor canal by passing through the adductor
hiatus, which is an opening formed by the tendon of
the adductor magnus muscle.
After passing through the adductor hiatus, the artery
enters the popliteal fossa and is now called the
popliteal artery.
https://3d4medic.al/3HhkjmOs
21.
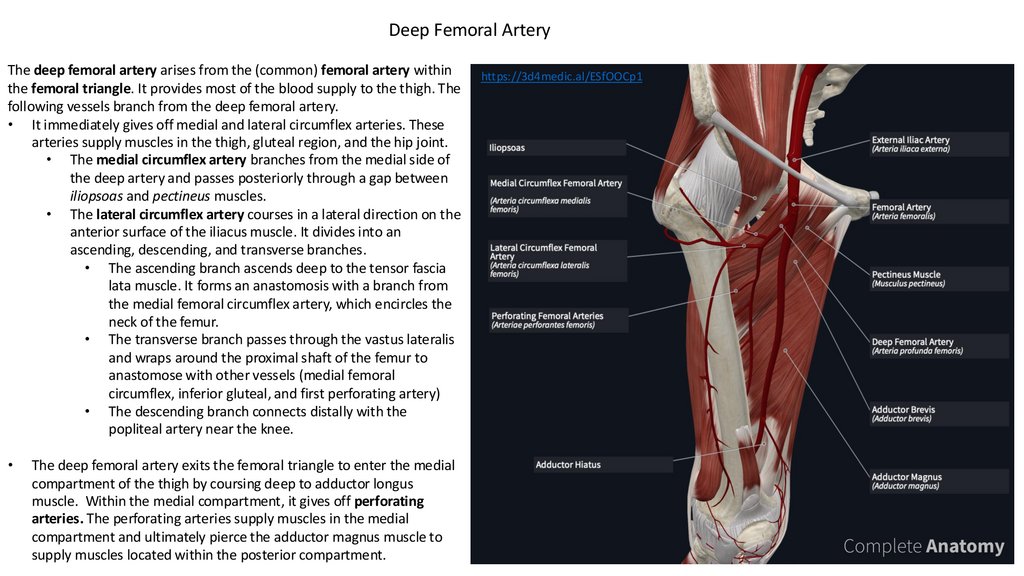
Deep Femoral ArteryThe deep femoral artery arises from the (common) femoral artery within
the femoral triangle. It provides most of the blood supply to the thigh. The
following vessels branch from the deep femoral artery.
• It immediately gives off medial and lateral circumflex arteries. These
arteries supply muscles in the thigh, gluteal region, and the hip joint.
• The medial circumflex artery branches from the medial side of
the deep artery and passes posteriorly through a gap between
iliopsoas and pectineus muscles.
• The lateral circumflex artery courses in a lateral direction on the
anterior surface of the iliacus muscle. It divides into an
ascending, descending, and transverse branches.
• The ascending branch ascends deep to the tensor fascia
lata muscle. It forms an anastomosis with a branch from
the medial femoral circumflex artery, which encircles the
neck of the femur.
• The transverse branch passes through the vastus lateralis
and wraps around the proximal shaft of the femur to
anastomose with other vessels (medial femoral
circumflex, inferior gluteal, and first perforating artery)
• The descending branch connects distally with the
popliteal artery near the knee.
The deep femoral artery exits the femoral triangle to enter the medial
compartment of the thigh by coursing deep to adductor longus
muscle. Within the medial compartment, it gives off perforating
arteries. The perforating arteries supply muscles in the medial
compartment and ultimately pierce the adductor magnus muscle to
supply muscles located within the posterior compartment.
https://3d4medic.al/ESfOOCp1
22.
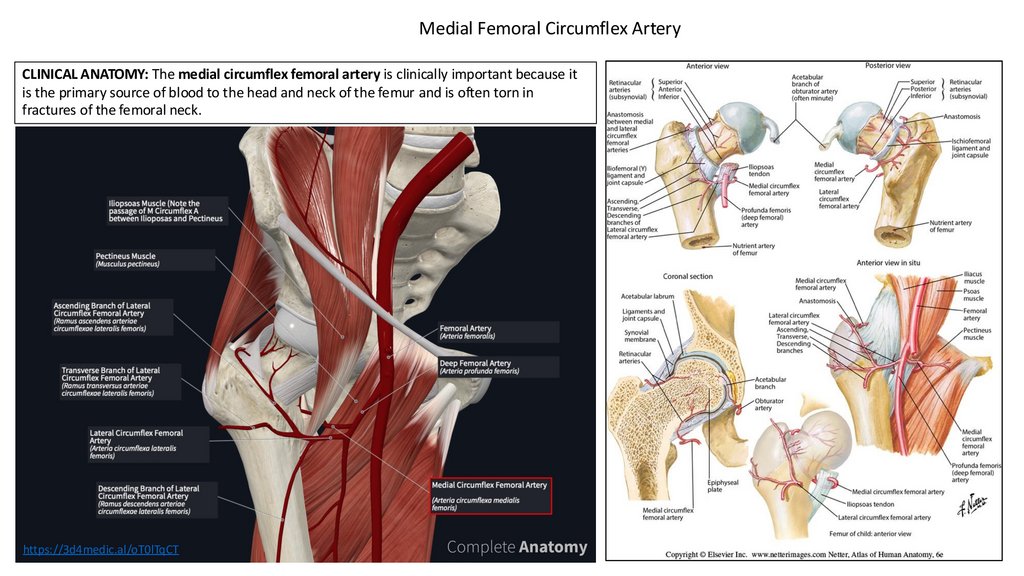
Medial Femoral Circumflex ArteryCLINICAL ANATOMY: The medial circumflex femoral artery is clinically important because it
is the primary source of blood to the head and neck of the femur and is often torn in
fractures of the femoral neck.
https://3d4medic.al/oT0lTqCT
23.
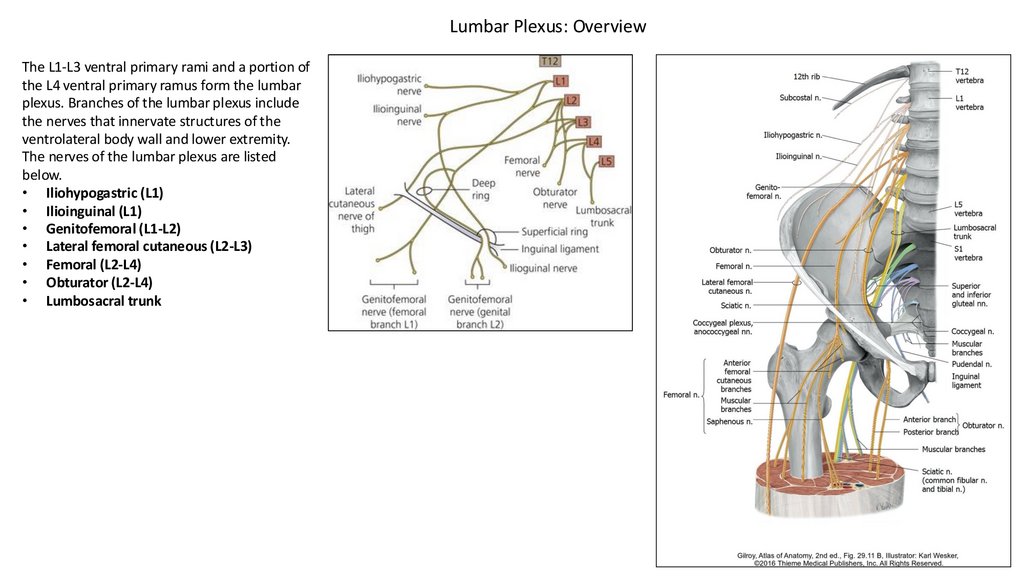
Lumbar Plexus: OverviewThe L1-L3 ventral primary rami and a portion of
the L4 ventral primary ramus form the lumbar
plexus. Branches of the lumbar plexus include
the nerves that innervate structures of the
ventrolateral body wall and lower extremity.
The nerves of the lumbar plexus are listed
below.
• Iliohypogastric (L1)
• Ilioinguinal (L1)
• Genitofemoral (L1-L2)
• Lateral femoral cutaneous (L2-L3)
• Femoral (L2-L4)
• Obturator (L2-L4)
• Lumbosacral trunk
24.
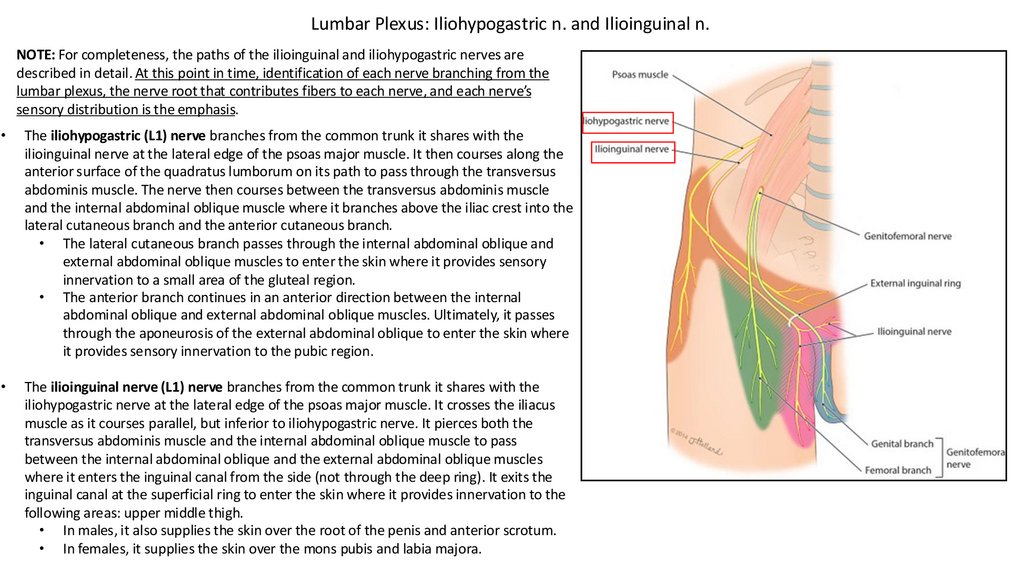
Lumbar Plexus: Iliohypogastric n. and Ilioinguinal n.NOTE: For completeness, the paths of the ilioinguinal and iliohypogastric nerves are
described in detail. At this point in time, identification of each nerve branching from the
lumbar plexus, the nerve root that contributes fibers to each nerve, and each nerve’s
sensory distribution is the emphasis.
The iliohypogastric (L1) nerve branches from the common trunk it shares with the
ilioinguinal nerve at the lateral edge of the psoas major muscle. It then courses along the
anterior surface of the quadratus lumborum on its path to pass through the transversus
abdominis muscle. The nerve then courses between the transversus abdominis muscle
and the internal abdominal oblique muscle where it branches above the iliac crest into the
lateral cutaneous branch and the anterior cutaneous branch.
• The lateral cutaneous branch passes through the internal abdominal oblique and
external abdominal oblique muscles to enter the skin where it provides sensory
innervation to a small area of the gluteal region.
• The anterior branch continues in an anterior direction between the internal
abdominal oblique and external abdominal oblique muscles. Ultimately, it passes
through the aponeurosis of the external abdominal oblique to enter the skin where
it provides sensory innervation to the pubic region.
The ilioinguinal nerve (L1) nerve branches from the common trunk it shares with the
iliohypogastric nerve at the lateral edge of the psoas major muscle. It crosses the iliacus
muscle as it courses parallel, but inferior to iliohypogastric nerve. It pierces both the
transversus abdominis muscle and the internal abdominal oblique muscle to pass
between the internal abdominal oblique and the external abdominal oblique muscles
where it enters the inguinal canal from the side (not through the deep ring). It exits the
inguinal canal at the superficial ring to enter the skin where it provides innervation to the
following areas: upper middle thigh.
• In males, it also supplies the skin over the root of the penis and anterior scrotum.
• In females, it supplies the skin over the mons pubis and labia majora.
25.
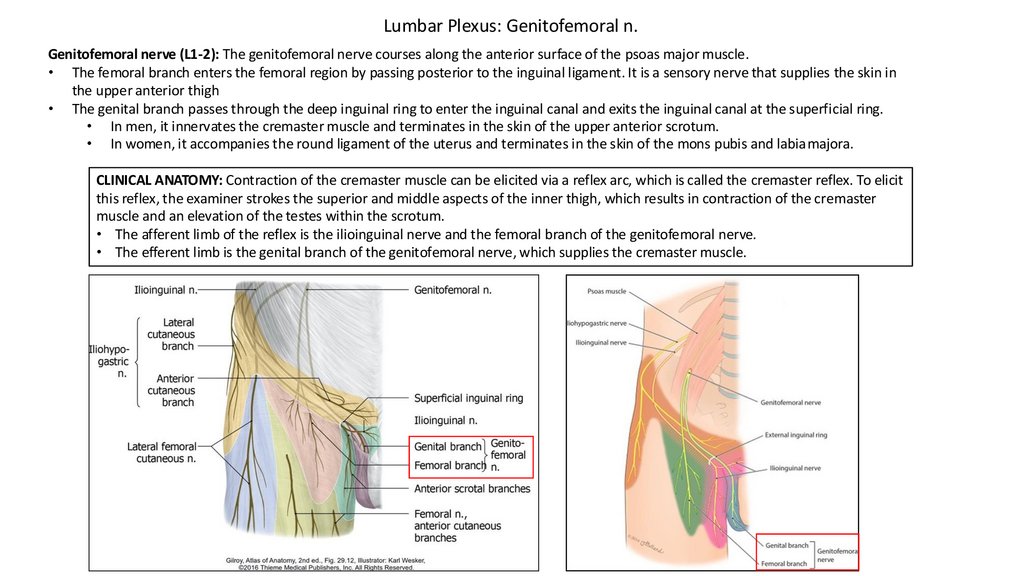
Lumbar Plexus: Genitofemoral n.Genitofemoral nerve (L1-2): The genitofemoral nerve courses along the anterior surface of the psoas major muscle.
• The femoral branch enters the femoral region by passing posterior to the inguinal ligament. It is a sensory nerve that supplies the skin in
the upper anterior thigh
• The genital branch passes through the deep inguinal ring to enter the inguinal canal and exits the inguinal canal at the superficial ring.
• In men, it innervates the cremaster muscle and terminates in the skin of the upper anterior scrotum.
• In women, it accompanies the round ligament of the uterus and terminates in the skin of the mons pubis and labiamajora.
CLINICAL ANATOMY: Contraction of the cremaster muscle can be elicited via a reflex arc, which is called the cremaster reflex. To elicit
this reflex, the examiner strokes the superior and middle aspects of the inner thigh, which results in contraction of the cremaster
muscle and an elevation of the testes within the scrotum.
• The afferent limb of the reflex is the ilioinguinal nerve and the femoral branch of the genitofemoral nerve.
• The efferent limb is the genital branch of the genitofemoral nerve, which supplies the cremaster muscle.
26.
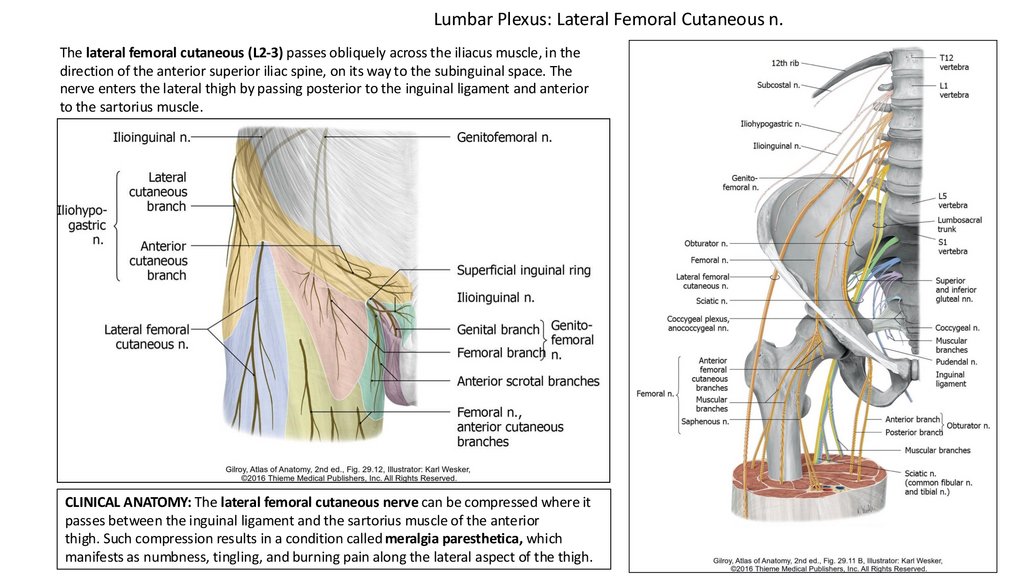
Lumbar Plexus: Lateral Femoral Cutaneous n.The lateral femoral cutaneous (L2-3) passes obliquely across the iliacus muscle, in the
direction of the anterior superior iliac spine, on its way to the subinguinal space. The
nerve enters the lateral thigh by passing posterior to the inguinal ligament and anterior
to the sartorius muscle.
CLINICAL ANATOMY: The lateral femoral cutaneous nerve can be compressed where it
passes between the inguinal ligament and the sartorius muscle of the anterior
thigh. Such compression results in a condition called meralgia paresthetica, which
manifests as numbness, tingling, and burning pain along the lateral aspect of the thigh.
27.
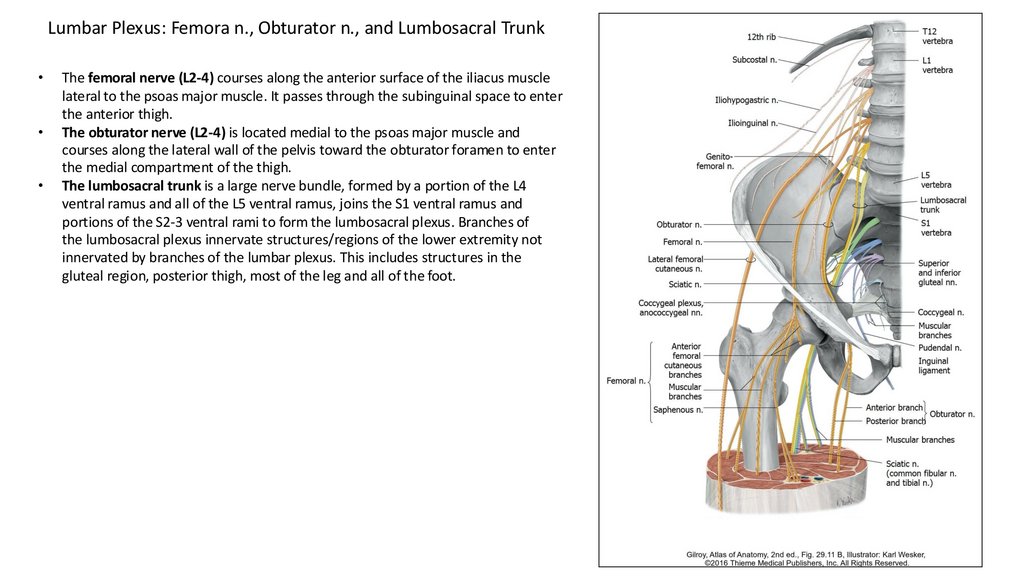
Lumbar Plexus: Femora n., Obturator n., and Lumbosacral TrunkThe femoral nerve (L2-4) courses along the anterior surface of the iliacus muscle
lateral to the psoas major muscle. It passes through the subinguinal space to enter
the anterior thigh.
The obturator nerve (L2-4) is located medial to the psoas major muscle and
courses along the lateral wall of the pelvis toward the obturator foramen to enter
the medial compartment of the thigh.
The lumbosacral trunk is a large nerve bundle, formed by a portion of the L4
ventral ramus and all of the L5 ventral ramus, joins the S1 ventral ramus and
portions of the S2-3 ventral rami to form the lumbosacral plexus. Branches of
the lumbosacral plexus innervate structures/regions of the lower extremity not
innervated by branches of the lumbar plexus. This includes structures in the
gluteal region, posterior thigh, most of the leg and all of the foot.