







")









 medicine
medicine biology
biologySimilar presentations:










Oral motor skills and feeding
1. Oral Motor Skills and Feeding
Debra Lauharn, M.A., OTRChristin R. Dowd, M.A., CCC-SLP
2.
AGENDA1. Anatomy and physiology of the oral/pharyngeal structures for feeding skills
2. A sequential look at development related to feeding skills
3. Oral motor treatment and feeding
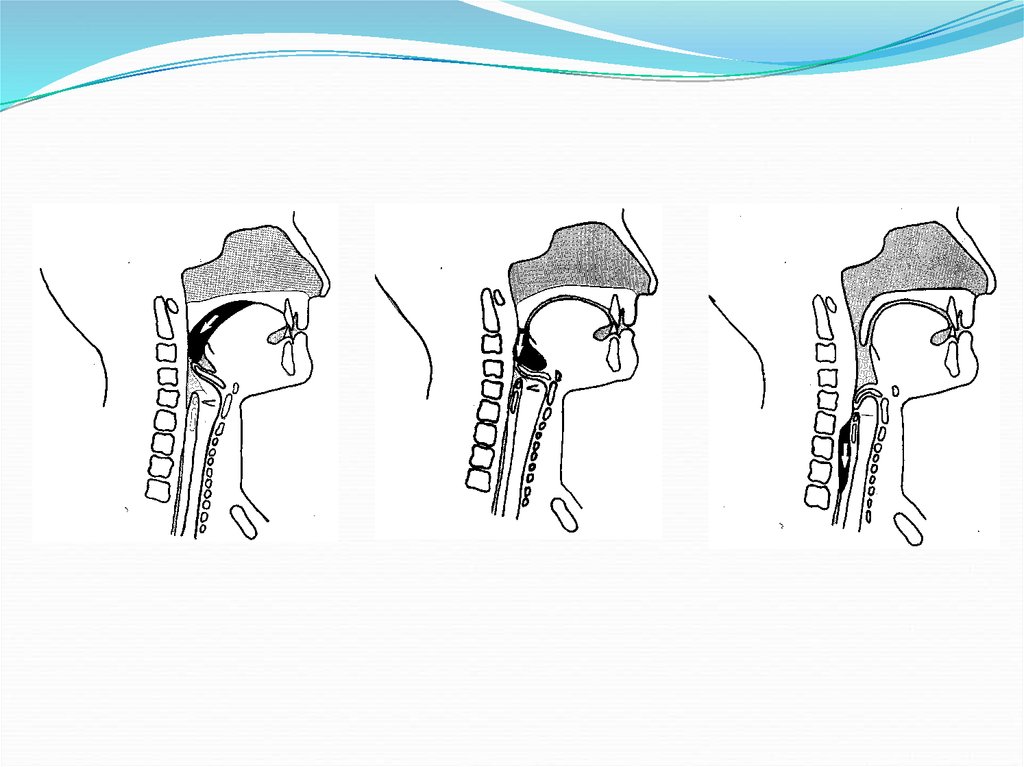
3. Anatomy
LipsTeeth
Tongue
Palate/Velum
Epiglottis
Trachea
Esophagus
4.
5. Normal Development and Feeding Skills
Please refer to handout6. Initial Observations
Look at motor patterns and body stability; positioningoptions
Determine sensory needs: gravitational security,
tactile/auditory/olfactory/gustatory defensiveness
Assess problems with function of individual oral
structures (jaw, kips, tongue, cheeks, palate)
Type of food child is eating
Behavioral issues: rule out medical, then determine if
it’s a sensory vs. behavioral issue
7. Medical Issues To Consider
Reflux: The backward flow of food or liquids that havealready entered the stomach.
Crying after eating
Excessive burping
Elongating of body (head to right and up)
Projectile vomiting
Not sleeping through the night
* medications
8.
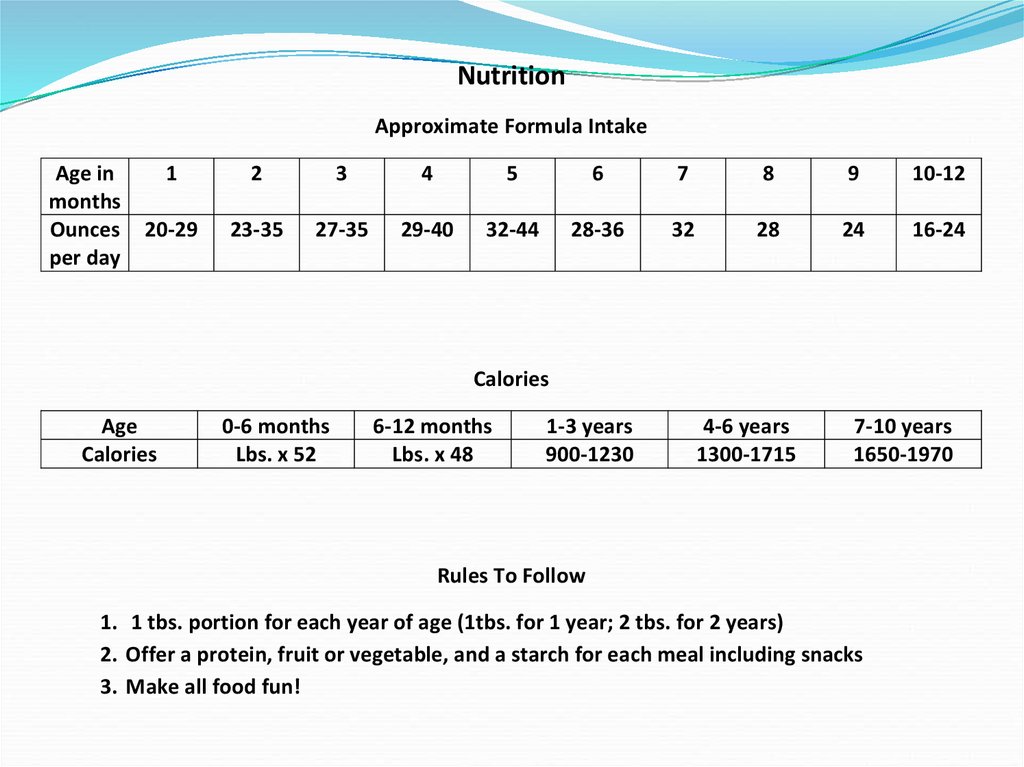
NutritionApproximate Formula Intake
Age in
months
Ounces
per day
1
2
3
4
5
6
7
8
9
10-12
20-29
23-35
27-35
29-40
32-44
28-36
32
28
24
16-24
Calories
Age
Calories
0-6 months
Lbs. x 52
6-12 months
Lbs. x 48
1-3 years
900-1230
4-6 years
1300-1715
7-10 years
1650-1970
Rules To Follow
1. 1 tbs. portion for each year of age (1tbs. for 1 year; 2 tbs. for 2 years)
2. Offer a protein, fruit or vegetable, and a starch for each meal including snacks
3. Make all food fun!
9. Positioning: What happens in your hips passes to your lips!
Mobility develops from proximal to distal; preciseinterchange between stability and mobility that
influences oral motor skills.
Oral stability is dependent upon the development of
neck and shoulder stability that is in turn dependent
on trunk and pelvic stability.
Lips, cheeks, and tongue are dependent on jaw
stability.
Position the child to support the head and trunk so
that the hands and mouth are free to work.
10.
11. For Safety Sake
Children should always be fed in a highchair or the lap of their parentNo cracked or sticky/gummy nipples (replace them)
Children under the age of 3 should not be given hard candy
No chocolate of any kind before 1 year
No honey before age 1
Hot dogs, peanuts, peanut butter, whole grapes, and candy are choking
hazards.
Begin open cup drinking at 6 months
Never lay a baby down with a propped bottle
Never give a baby a bottle or sippy cup to keep in their bed to pacify
them. If you must, only fill it with water
No bottles after 15 months
No cereal in bottle!!!!!
12. Sensory Needs How comfortable is the child in his/her feeding environment
Change the noise, lighting and visual stimuliPrepare the body and mouth for eating (PRR/brushing,
swinging, proprioception, vibration, massage)
Changing food (temp, taste, texture) slowly
Hyposensitivity (ASD, low tone) prefer to drink and not eat
or prefer to eat soft/easy foods. *add spice to their life
Hypersensitivity (CP, high tone) use smooth bland food
Be social and engaging during meal times.
13. Techniques For Dysfunctional Oral Structures (Lips, jaw tongue and cheeks)
Jaw: slack/low muscle tone or jaw thrustopen/increased muscle tone and teeth grinding
Check positioning of the hips/shoulders/chin (reduce
hip extension or posterior tilt and shoulder retraction,
and position the chin down)
Give jaw control/support as needed
Calm/organize the mouth with vibration
Ice/cold increases swallow reflex (ie ice straw)
Chew tubes
Bite tip on Z-Vibe (front to back on left and right)
14. Chewing Techniques
The goal is to teach a graded, lateral chew with tongue-tipdissociation and movement across midline.
Graded lateral chew with tongue tip pointing: chew tube or Z-Vibe
perpendicular to the lateral molar ridge as you support jaw as
needed, encourage 2-3 bites. Alternate sides 4-5 times. Intro.
Veggie stix or ice straw
Tongue tip Pointing and movement of bolus to lateral incisor and
molar ridge: place tube/stick food from molar ridge to lateral
incisor and alternate sides
Tongue-tip pointing and tongue lateralization across midline:
present stick-shaped food or tube on lateral incisor and bit quickly
present bolus to opposite lateral incisor.
5 point bite: present the stick shaped bolus perpendicular to the
lateral molar ridge, to the incisor, to the front, and move bolus
around midline to opposite molar ridge.
15. Tongue Retraction
In tongue retraction the tongue pulls back into theposterior ¾ of the mouth or in the pharyngeal airway.
Can be related to low or high muscle tone with neck
hyper extension or cleft palate
Work on building tone by bouncing on a ball or lap
before positioning for eating
Child is prone over lap then stroke tongue from middle
to tip toward lips
When seated, keep child’s chin tucked down, gently
tap/hold under chin to increase tongue tone/stability,
vibrate from middle to tip and lateral to tip (Z-vibe)
16. Tongue Protrusion
Low tone tongue moves forward beyond the border of thegums and may stick out between the lips and may cause
food to be pushed out of the mouth
Build tone in the trunk and provide proximal stability by
compression of spine through shoulders, bounce on lap or
ball
Position in feeding chair with increased support of the trunk
and feet
Feed to the sides of the mouth to improve tongue
lateralization
Thicken liquids
Present flat bowl spoon in horizontal position midway and
vibrate to tip (Z-Vibe)
Offer vibration with battery operated toothbrush or Z-Vibe
17. Lip retraction
Lip retraction occurs with increase muscle tone pulling/drawing thelips and cheeks backward to form a tight horizontal mouth, making it
difficult to suck from a bottle or remove food from a spoon. Lip pursing
occurs when the child attempts to counteract the effects of retraction.
Before each meal:
Check sitting position for too much hip extension/shoulder
retraction/head extension
check for overstimulating environment and sensory properties of the food
given (spicy/bland)
Midline orientation/3 point massage (cheeks, facial folds, upper lip)
Reduce hypertonicity in cheeks with vibrating hands on each cheek forward
or vibrating bug/Z-vibe
Lip massage: rub infadent finger or roll cut down toothette from the R
corner to midline, the L corner to midline *DO NOT CROSS MIDLINE
Facial molding with towel or flat palms move the cheeks forward and
chin/lower lip upward
Straw drinking or cup drinking (with cut out cup)
18. Low tone cheeks/lips
Hypotonia in the cheeks reduces the strength/skill of thelips causing inefficient sucking and bolus collection,
excessive drooling and open mouth, decreased awareness
and overstuffing/food pocketing. Before each meal:
Increase tone in body with bouncing and compressions
Engage midline orientation with 3 point massage
Play patty-cake and other games to the cheeks that provide firm
input to sides of the face
Lip massage: rub lips from midline out ward to sides (stretch)
Explore mouth with ice, spicy, tart/sour foods to increase pucker
“Hide” soft food/banana or cheese in cheek pockets and have child
squeeze side of cheek to push food to center
Vibrate to increase awareness
Straw drinking
Three Point massage…
19. Straw drinking/Cup use
Use a squeeze box with short, thick straw *place straw atcorner of mouth and quickly move to midline (repeat on
each side).
Use aquarium tubing in squeeze bottle
Use cork or medium bead to adjust the length of straw in
the mouth. The portion that enters the mouth should be
very short at first.
Use thick liquids (honey consistency) with straw or cup (ie.
milkshake, applesauce, baby food)
Use cut out cup and push corner to corner to improve lip
closure and decrease tone *use jaw control as needed.
*Try club soda and juice to increase awareness of liquid
20. Incorporate solid foods in therapy
Cheetos and other junk food are good starter foods(they melt)
Shave a carrot or potato for teething, texture, and
proprioception/biting
Use veggie stix for chewing
21. Prevent Food Jags
Food jags are when a child will only eat certain foodsand may demand that they are presented the same way
(ie.certain label food, on a stick, wrapped in paper
towel)
The brain does not produce pathways to accept other
foods
Steps to prevent food jags
22.
Works Cited(2010). Retrieved September 20, 2010, from Mealtime notions llc: http://www.mealtimenotions.com
C Drobek, C. M. (2005). Building Blocks of Pediatric Therapy. Detroit: Children's Hospital of Michigan Detroit Medical Center/Wayne State University.
Harrison, T. (1996). Feeding your 1 to 5 year old building good eating habits. Okemos, Michigan: United Dairy Council of Michigan.
K. Toomey, E. R. (2007). When Children Won't Eat The SOS Approach to Feeding. Farmington Hills, MI: Abilities Center.
Klein, S. M. (1987). Pre-Feeding Skills. Tucson: Therapy Skill Builders.
Logemann, J., (1993). Manual for the videofluorographic study of swallowing (2nd ed.) Austin, TX: Pro-Ed
Overland, L. (1996). Feeding Therapy: A Sensory Motor Approach. Talk Tools Inoovative Therapists International.
Winstock, A. (2005). Eating & Drinking Difficulties in Children. Oxen: Speechmark Publishing Ltd.