
















 history
historySimilar presentations:










Profiles in Combat. Casualties
1.
Profiles in CombatCasualties
2.
WAR WOUNDSHistory, Wound Description,
Mechanisms and Wounding Agents,
Distribution of Wounds/Wounding By
Anatomical Location and by
Demography,
Following this lecture the participant will be
able to:
– Discuss why military medical personnel should
know something about weapons and the effects
they produce
– State which wounds are most commonly
associated with death.
3.
WAR WOUNDSFollowing this lecture the participant will be
able to (cont.):
– State the frequency with which the various type of
combat wounds occur and the impact that type of
combat, geography, and weapons available have on
the relative percentages of each type.
– List the various wounding patterns associated with
different types of weapons and different types of
combat
– State who primarily gets wounded/killed in combat
– State where in the echeloned combat health care
system the deaths occur
4.
Dulce bellum inexpertis(War is delightful to those who
have no experience of it)
Erasmus
5.
Military field therapy is the most importantsection of military medicine. Its content is
the study of the etiology, pathogenesis, clinic,
prevention and treatment of injuries from
military weapons and diseases of internal
organs that occur in the conditions of
combat activities of the troops, the
development of organizational forms for the
provision of therapeutic assistance to these
categories of victims.
6.
Stages of HTP developmentorigin
formation and design
further development in the conditions
real possibility of application
weapons of mass destruction
modern period of development
7.
On April 22, 1915, as a result of the first German gasballoon attack on the Anglo-French positions near the
Ypres River, 15,000 people were poisoned with chlorine,
of which about 5,000 (33%) died. AT
subsequent OV during the war were used repeatedly,
which led to significant losses in manpower.
Only in the Russian army 65158 people were struck.
Altogether in In the First World War, about 1.3 million
people were affected by chemical weapons.
So a new type of destruction of personnel arose - mass
combat therapeutic trauma, qualitatively different from
all what therapists had to deal with before.
8.
Thus, in the conditions of modern warfare,the relevance of combat therapeutic pathology, its essential
role in the structure of sanitary losses, in connection with
which the importance of organizing therapeutic care for the
sick and injured in the army increases. With the likely use of
weapons of mass destruction, the importance of organizing
therapeutic assistance to the sick and injured will increase
even more and become more complicated.which is
determined to a large extent by the magnitude and structure
of sanitary losses
9.
War in Afghanistan, events in Bosnia, Croatia, Serbia,Chechnya, Iraq, South Ossetia, a surge in armed
confrontations in different countries of the world have
caused medical concern.
The public. Civil health physicians increasingly
facewith modern combat surgical pathology, in which
the leading role is played not by bullet or shrapnel
wounds, but by multifactorial lesions inflicted by
explosive ammunition.
10.
The modern concept provides for the provision of the firstmedical, pre-medical and first aid according to urgent
indications in the focus or near the focus of emergency
situations, followed by evacuation of the victims to hospitals
medical institutions. At the same time, the decrease in
mortality is achieved by reducing the time for providing
medical care. The first hours and days are called “golden
time”.
However, it is during this period that the lack of forces and
means involved in the elimination of the consequences of
accidents is most acutely felt. A clear confirmation of this is
the fact that during the liquidation of the consequences of
the disaster in Bashkiria (June 4, 1989 1264 people of two
trains were injured, 408 died) the first a medical and
nursing team (out of 43 ambulances) arrived at the place of
assistance in an ambulance only after 1 hour 20 minutes,
the rest due to off-road reached the goal.
11.
Medical triage is the distribution of the wounded andpatients into groups based on the need for homogeneous
propreventive and therapeutic measures in accordance with
medical indications, the established amount of assistance
at this stage and the accepted evacuation procedure, is
carried out at each
stage of medical evacuation, in all its functional
subdivisions. It is divided into intrapoint and evacuation
transport sorting. When it is carried out, the division into
groups
affected is carried out on the basis of:
1. The need for sanitization (partial, complete) and
isolation;
2. the need for medical care, location and the order in
which it was received;
3. possibility and expediency of further evacuation, type of
vehicles, sequence, method of transportation and
evacuation purposes.
12.
Medical triage is the distribution of the wounded andpatients into groups based on the need for homogeneous
propreventive and therapeutic measures in accordance with
medical indications, the established amount of assistance at
this stage and the accepted evacuation procedure, is carried
out at each
stage of medical evacuation, in all its functional
subdivisions. It is divided into intrapoint and evacuation
transport sorting. When it is carried out, the division into
groups
affected is carried out on the basis of:
1. The need for sanitization (partial, complete) and isolation;
2. the need for medical care, location and the order in which
it was received;
3. possibility and expediency of further evacuation, type of
vehicles, sequence, method of transportation and evacuation
purposes.
13.
First medical aid is provided at the regiment's medical station (MPP) and includes measuresfor urgent indications and measures that may be delayed.
Urgent first aid measures are carried out in conditions that threaten the life of the
affected:
- elimination of desorption of toxic substances (S) from uniforms (partial sanitization
(PSD), change of uniforms);
- cleaning the oral cavity and nasopharynx from mucus and vomit;
- the introduction of antidotes, anticonvulsants, bronchodilators and antiemetics;
- gastric lavage with a probe for oral
poisoning;
- the use of antitoxic serum for poisoning
bacterial toxins and non-specific prophylaxis for
lesions by bacterial agents;
- oxygen inhalation, mechanical ventilation, bloodletting;
- the introduction of cardiovascular drugs, respiratory analeptics, painkillers,
desensitizing and other drugs
14.
Conditionsrequiring
urgent
measures of qualified therapeutic assistance:
1. Relief of life-threatening complications,
diseases and defeats:
- convulsions;
- collapse;
- violations of intracardiac conduction;
- severe cardiac arrhythmias;
- hypertensive crisis;
- asphyxia; severe bronchospasm, laryngospasm;
bronchopneumonia
complicated
by
cardiovascular and respiratory failure;
- colic of various origins;
- cessation of breathing.
15.
Immediate interventions for qualified medical care include: Sanitary treatment of thewounded and sick in case of infection toxic substances;
- the introduction of antidotes and anti-botulinum serum;
- complex therapy of acute cardiovascular insufficiency, cardiac arrhythmias;
- complex therapy of acute respiratory failure;
- dehydration therapy for cerebral edema;
- correction of gross violations of the acid-base state and electrolyte balance;
- a set of measures in case of ingestion of toxic and other toxic substances;
- the introduction of painkillers, desensitizing, antiemetic, anticonvulsant and
bronchodilator drugs;
- the use of tranquilizers, neuroleptics in acute reactive states;
- forced diuresis;
- oxygen therapy;
16.
The Evolution ofWeapons of War
17.
Wounds of WarHistorical
Background
18.
The Inventionof Gunpowder
19.
Encoded formulafor gunpowder
and a depiction
of its use
20.
HISTORY OF WAR WOUNDSCHANGING PATTERNS OF
WOUNDING THROUGHOUT HISTORY
EFFECTS OF EVOLVING WEAPONS
SYSTEMS
EFFECTS OF EVOLVING TACTICS
21.
The Modern Battlefield:More Dangerous and Violent
Than Ever
“Smart” Weapons, Improved conventional
munitions
– Increased probability of multiple hits
Automatic Weapons - Multiple hits
– Decreased proportion of surviving wounded
Fragments will cause 80-90% of living
wounded
More extremity wounds - effects of protective
equipment
22.
Combat Wounds Are UniqueHigh percentage of penetrating
wounds
Multi-System injury
Multi-Etiologic
High degree of wound contamination
Old (delayed initial care)
23.
HighlyContaminated
“Old”
Wounds
24.
Mechanisms ofCombat Injury
25.
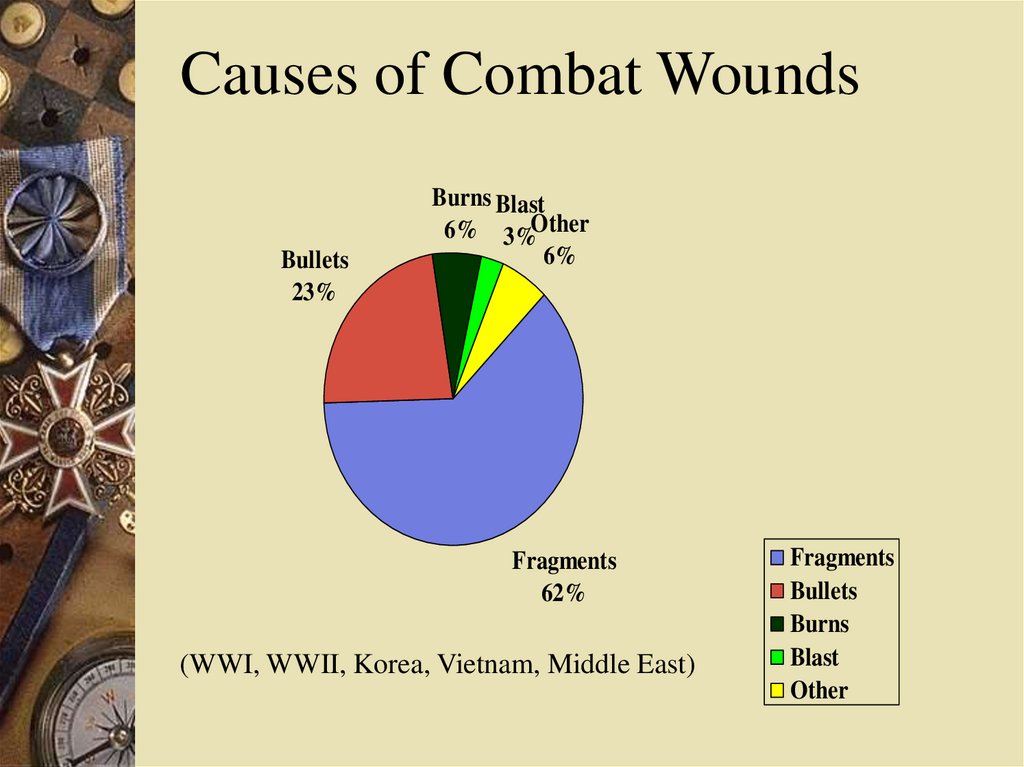
Causes of Combat WoundsBullets
23%
Burns Blast
6% 3%Other
6%
Fragments
62%
(WWI, WWII, Korea, Vietnam, Middle East)
Fragments
Bullets
Burns
Blast
Other
26.
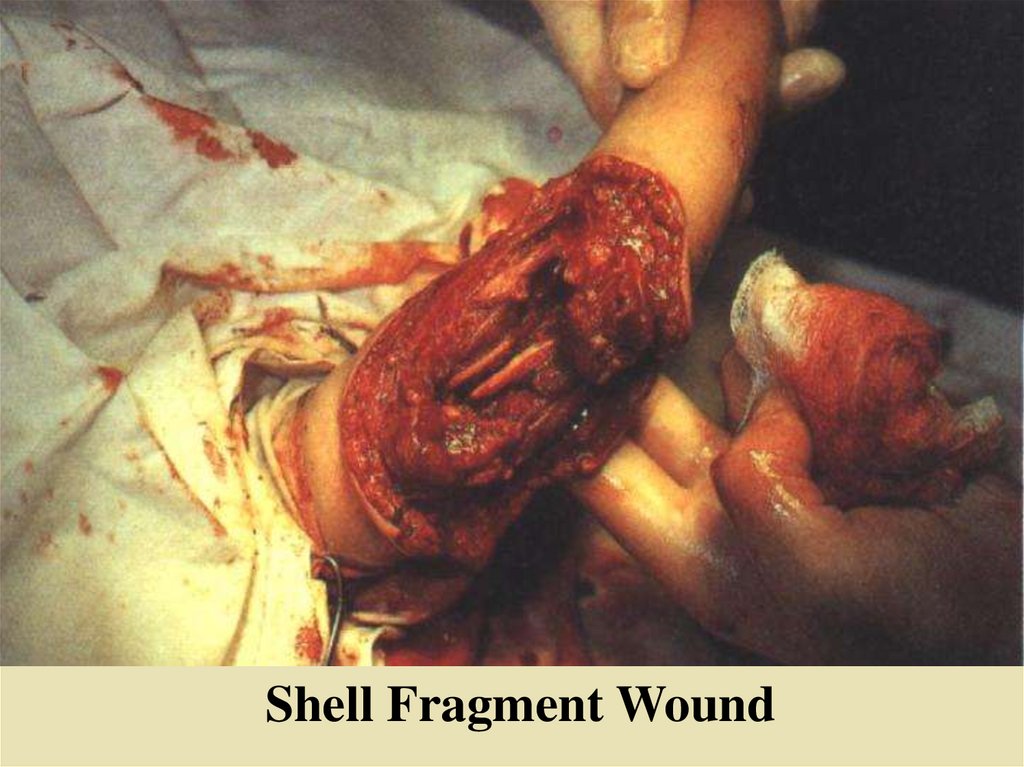
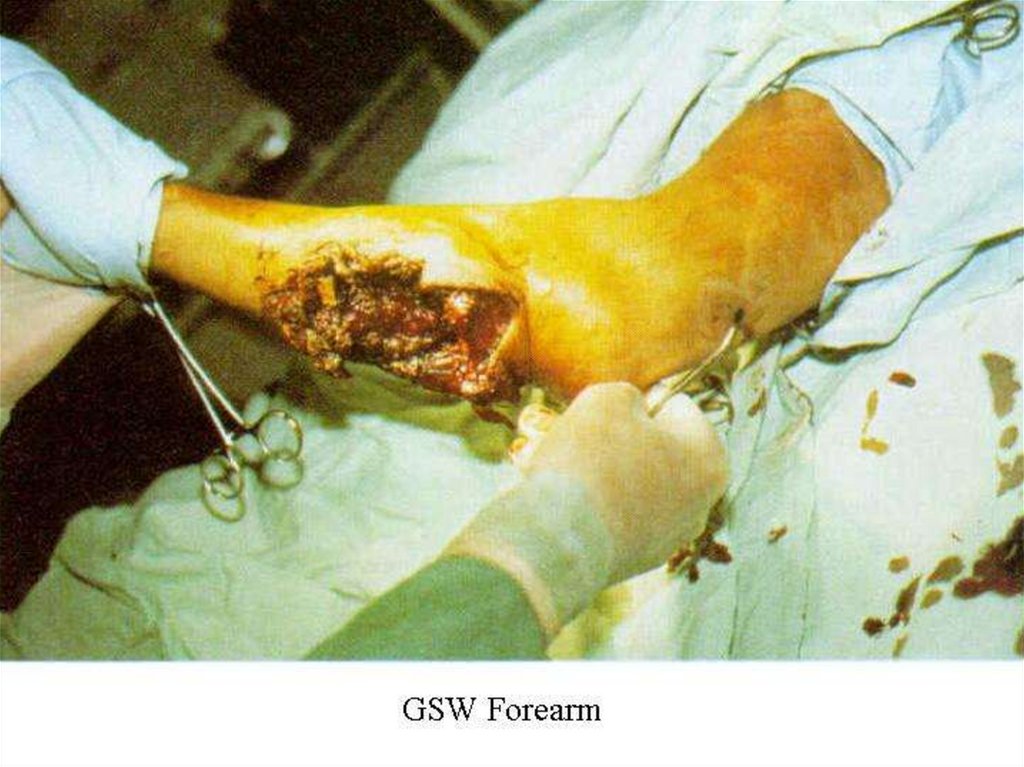
Shell Fragment Wound27.
Fragments from exploding anti-tank weapon28.
LandmineInjury
29.
30.
M-16 assault rifle 5.56mm GSW (exit)31.
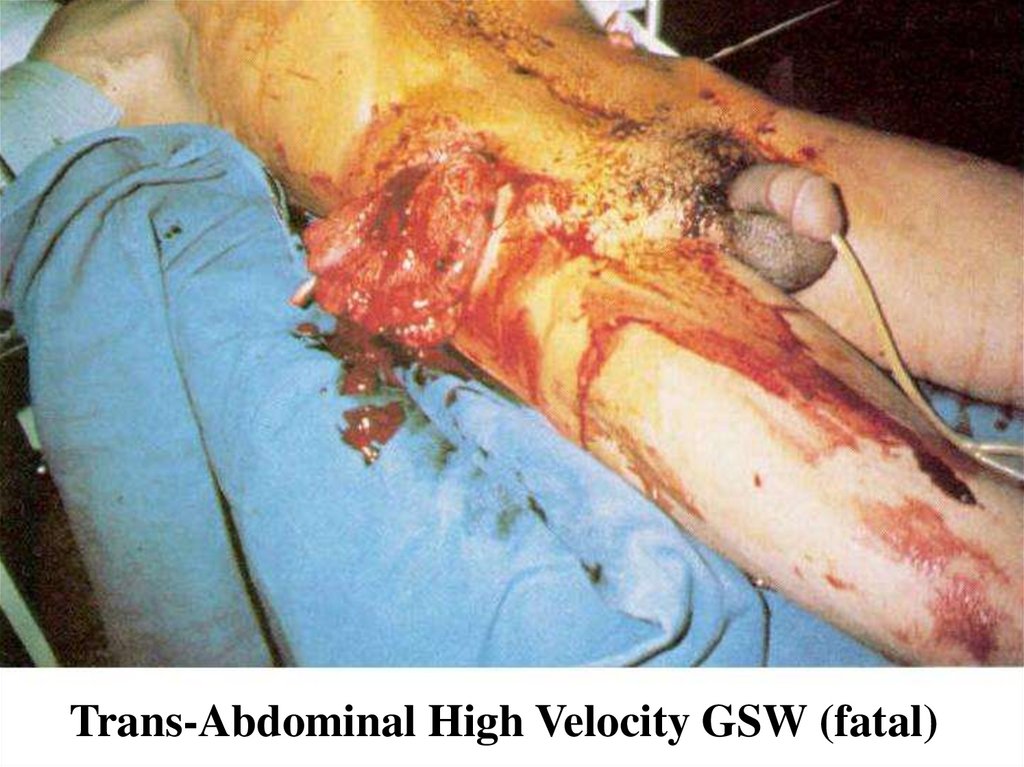
Trans-Abdominal High Velocity GSW (fatal)32.
FacialBurns
Kosovo
33.
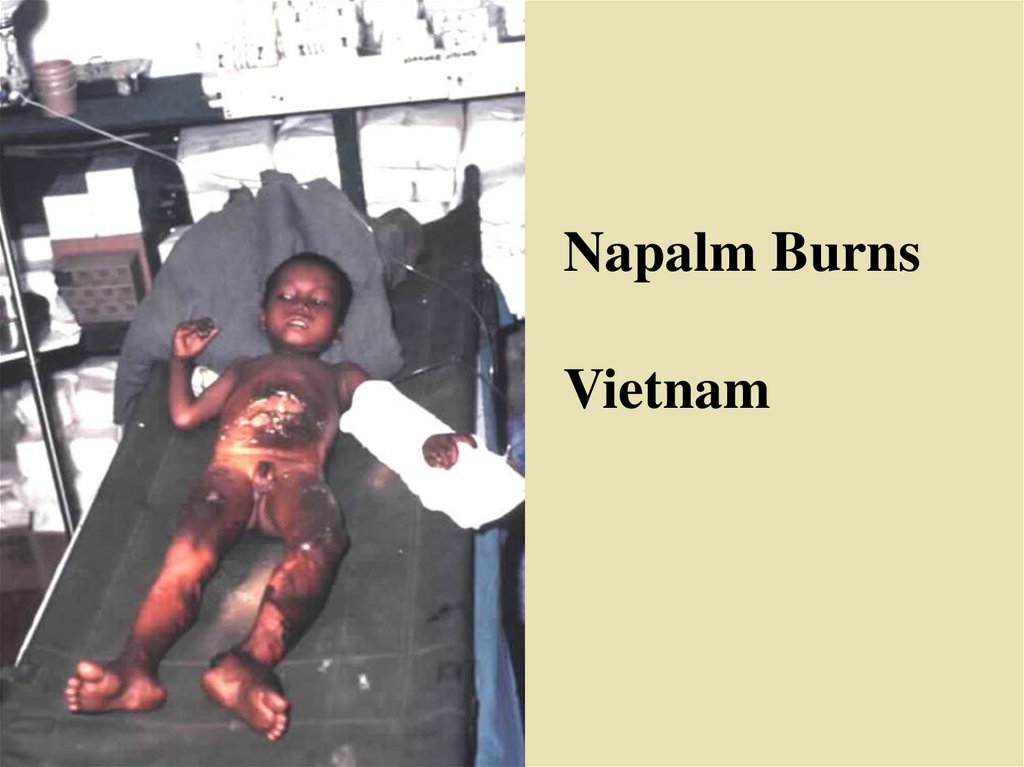
Napalm BurnsVietnam
34.
Burns - The IsraeliExperience
Six Day War 1967 - 4.6% Burn Injuries
October War 1973 - 8.1% Burn Injuries
Lebanon War 1982 - 7.6% Burn Injuries
35.
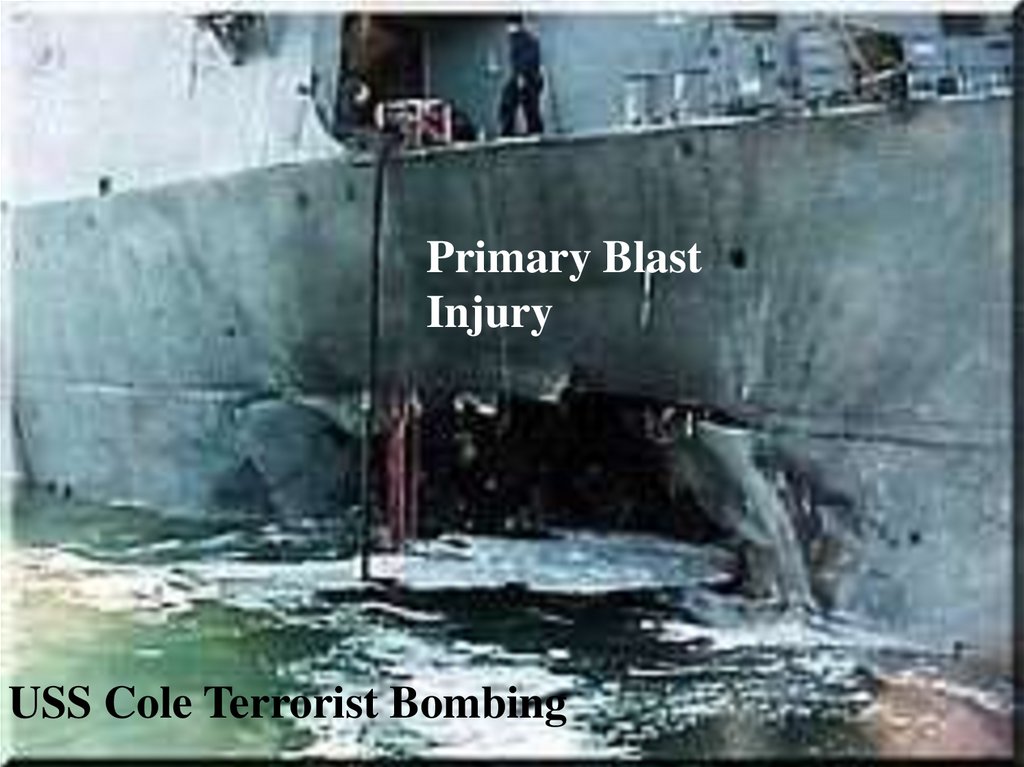
Primary BlastInjury
USS Cole Terrorist Bombing
36.
Primary Blast InjuryPrimary Blast Injury is uncommon in most
combat casualties but:
– In an armored vehicle that has been penetrated by a
large warhead,1-20% of the survivors will have some
degree of 1o blast injury in addition to other wounds.
– Primary blast injury is considerably more common in
casualties due to naval combat
37.
War Wound DistributionChest
13%
Other
9%
Head & Neck
17%
Abdomen
5%
Upper
Extremities
21%
Lower
Extremities
35%
Upper Extremities
Lower Extremities
Abdomen
Head & Neck
Chest
Other
38.
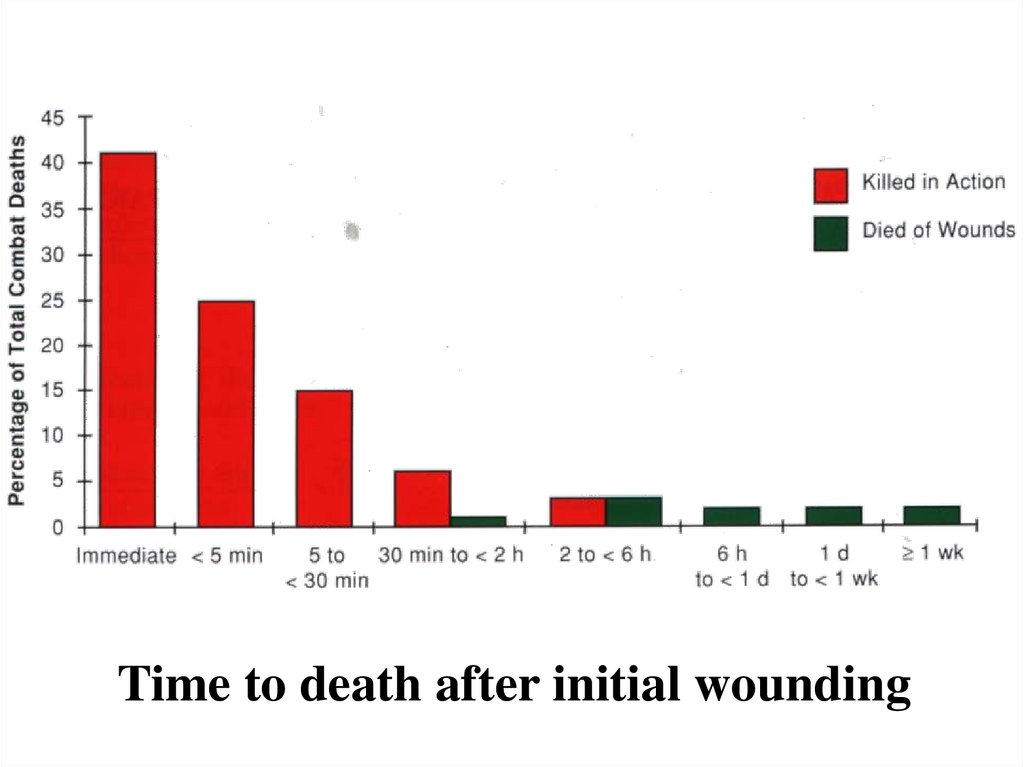
Time to death after initial wounding39.
Mechanisms of Injuryand Distribution of
Injuries by
Geographic Environment
and Type of Combat
40.
North AfricaAgent
Percent
Shell fragments...................................…. 75
Bullets...................................................... 20
Mines........................................................ 2
Bombs....................................................... 1
Other......................................................... 2
_____
Total............100
41.
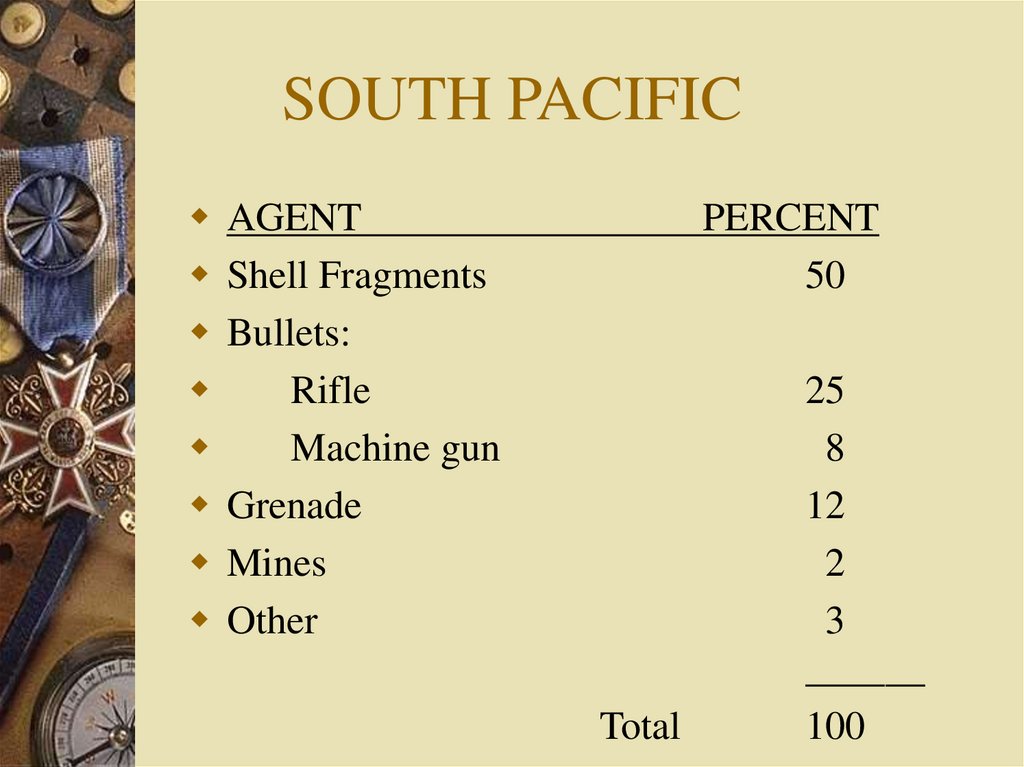
SOUTH PACIFICAGENT
Shell Fragments
Bullets:
Rifle
Machine gun
Grenade
Mines
Other
PERCENT
50
Total
25
8
12
2
3
______
100
42.
VietnamAgent
Shell Fragments
(Artillery, mortar, rocket)
Bullets (rifle and pistol)
Booby traps, mines, grenades
Percent
38.9
23.8
27.7
43.
Wounding Agents in theFalklands
Gunshot Wounds - 38%
Fragment- Caused Wounds - 40%
Burns - 18%
44.
Sites of Wounding - FalklandsHead and Neck - 30/133 (23%)
Upper Limb - 42/133 (31%)
Lower Limb - 88/133 (68%)
Intra-thoracic - 11/133 (8%)
Intra-peritoneal - 12/133 (8%)
Multiple Wounding Sites - 59/133 (41%)
45.
Distribution of Wounds ByAnatomic Group - Viet Nam
Head and Neck - 16.5%
Thorax - 7.3%
Abdomen - 8.0%
Upper Extremities - 27.7%
Lower Extremities - 40.5%
46.
War WoundsWho is wounded /
killed in war?
47.
Vietnam - Marine CorpsWounded
Mean Age - 20.7 years old
Distribution by Pay Grade
E1 - E3 - 71.2% of those wounded
E4 - E6 - 25.6% of those wounded
Officers - 2.7% of those wounded
48.
Distribution of Wounding inVietnam by Occupation
Infantry - 71.8% of those wounded
Artillery - 2.2% of those wounded
Direct Correlation between a Lack of Combat Experience
and Increased Wounding
49.
When only ground troopsare studied, the ratio of
WIA/KIA, which was
4.2/1 in WW II, has
remained essentially
unchanged for the past 200
years.
50.
SITE OF EXSANGUINATION IN98 VIET NAM COMBAT DEATHS
16 - Heart/Ascending Aorta
13 - Lung/Pulmonary Artery
10 - Liver
10 - Multiple Abdominal Sites
9 - Great Vessels of the Thorax (Principally the
Aorta)
*9 - Arteries in the Lower Extremity
8 - Great Vessels of the Abdomen (especially the
Aorta/Vena Cava
51.
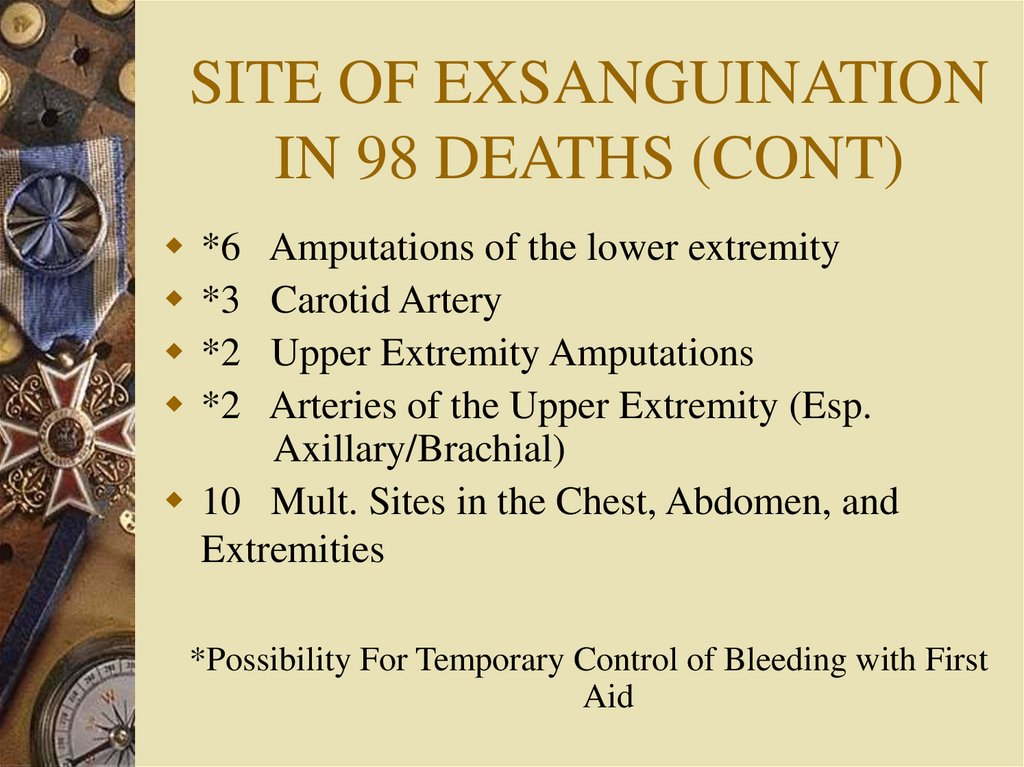
SITE OF EXSANGUINATIONIN 98 DEATHS (CONT)
*6 Amputations of the lower extremity
*3 Carotid Artery
*2 Upper Extremity Amputations
*2 Arteries of the Upper Extremity (Esp.
Axillary/Brachial)
10 Mult. Sites in the Chest, Abdomen, and
Extremities
*Possibility For Temporary Control of Bleeding with First
Aid
52.
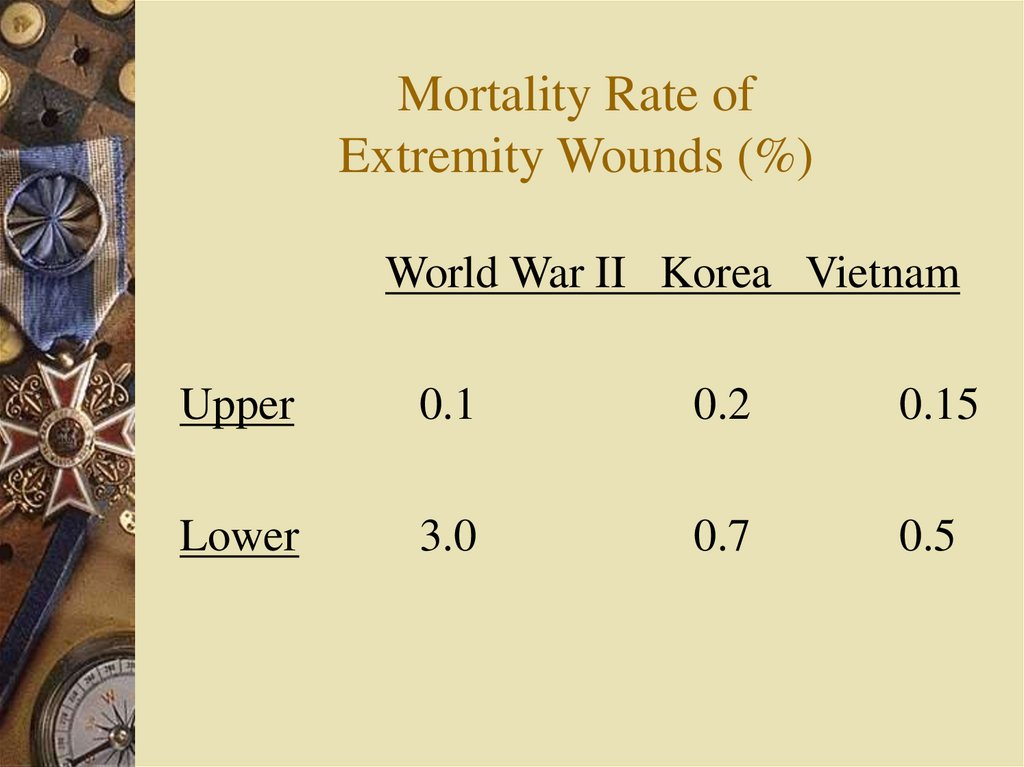
Mortality Rate ofExtremity Wounds (%)
World War II Korea Vietnam
Upper
0.1
0.2
0.15
Lower
3.0
0.7
0.5
53.
"BATTLE CASUALTIES,INCIDENCE, MORTALITY,
AND LOGISTIC
CONSIDERATIONS"
By
Gilbert W. Beebe, Ph.D..
Michael E. De Bakey, MD
54.
UNDERSTANDINGWAR, HISTORY
AND THEORY OF
COMBAT
BY
T.N. Dupuy, 1987
Paragon House Publishers,
N.Y.
55.
FACTORS WHICH INFLUENCEWOUNDING RATES ON THE
BATTLEFIELD
Ratio of enemy to strength.
Type of weapons employed and ratio of
enemy to firepower
The experience and training of the troops
Terrain
Tactical advantage and the excellence of the
plan.
56.
FACTORS WHICH INFLUENCEWOUNDING RATES ON THE
BATTLEFIELD (cont)
Availability of prepared positions
Possession of key terrain
Quality of available intelligence
Tactical and strategic support
Logistic support
57.
The site of death for 90% of fatally woundedcombat casualties is the battlefield.
58.
Casualty RatesAVERAGE WORLD WAR II DIVISION
ENGAGEMENT
– Casualty rates were 1-3% per day
59.
Attrition RatesAttrition Rates in the 1973
Arab-Israeli October War
Were Comparable to World
War II
60.
It is vital that the medicalofficer "...be in a position to
check the tactical situation
estimates with other staff
officers so that his plans may
be more securely grounded".
61.
QuotesVICTORY IS THE
BEST MEDICINE
62.
Quotes...[M]edicine has...[an] indirect
influence on war which is not
negligible. there seems little doubt
that some of the reckless courage
of...American troops...[is]
stimulated by the knowledge that
in front of them [is] only
the...[enemy], but behind
them...[are] the assembled
surgeons of America, with sleeves
rolled up.”
Hans Zinsser, “Rats, Lice and History”
63.
SummaryFollowing this lecture the participant will be able
to:
– Military medical personnel should know something
about weapons and the effects they produce because
such knowledge is useful
• for medical planning purposes
• to aid in developing or improving wounding prevention
methods
• in helping to estimate the number and types of casualties that
might be generated
• To improve communication with the line
64.
Summary– The most common combat wounding mechanisms are
• Fragments
• Fragments
• Fragments
• Fragments
• Bullets
• Bullets
• Blast and burns and all other (unless you are in the navy
AND you are assigned to a ship in which case blast and burn
make up a larger percent)
65.
Summary– The frequency with which the various type of
combat wounds occur (see above) – all of
these depend upon type of combat (geography,
weapons available, type of combat etc.)
• Fragments (all types) 50 – 90%
• Bullets <10% - 50%
• Primary Blast – generally <5%
• Burn (all types) – generally <5
66.
Summary– Wounding patterns associated with different types of
weapons
• For most weapons wounding location is random and thus
primarily based upon body surface area therefore – Extremities which make up roughly 55% of BSA account from
roughly 55% of sites of wounding
– Landmines clearly primarily affect the lower extremities
– Some bullets are aimed so there is a slightly higher percent of
wounds in torso and head
– Head and neck are injured somewhat disproportionate to their
BSA because these body parts are more commonly exposed
(have to be able to see to shoot!) -roughly 17% instead of 10%
67.
SummaryWho primarily gets wounded/killed in combat
– Young men ages 18 – 24
– Predominantly infantrymen
– Almost entirely enlisted men with 2nd Lieutenants
being at highest risk of death among officers
Which wounds most commonly cause death?
– Head and Chest Wounds
Where do most deaths occur?
– On the battlefield (mostly at the point of wounding
and within <5 minutes of wounding)
– Relatively few die once reaching a hospital