 medicine
medicineSimilar presentations:










Chronic Heart Failure
1.
CRIMEAN STATE MEDICAL ACADEMYNAMED AFTER S. I. GEORGIEVSKY OF VERNADSKY CFU
DEPARTMENT OF INTERNAL MEDICINE NO.2
CHRONIC HEART FAILURE (CHF)
NAME : ABDUL NAZAR SHEIK ABDULLA THAMEEM
COURSE: 4TH
GROUP .: LA2-CO-171-2
2.
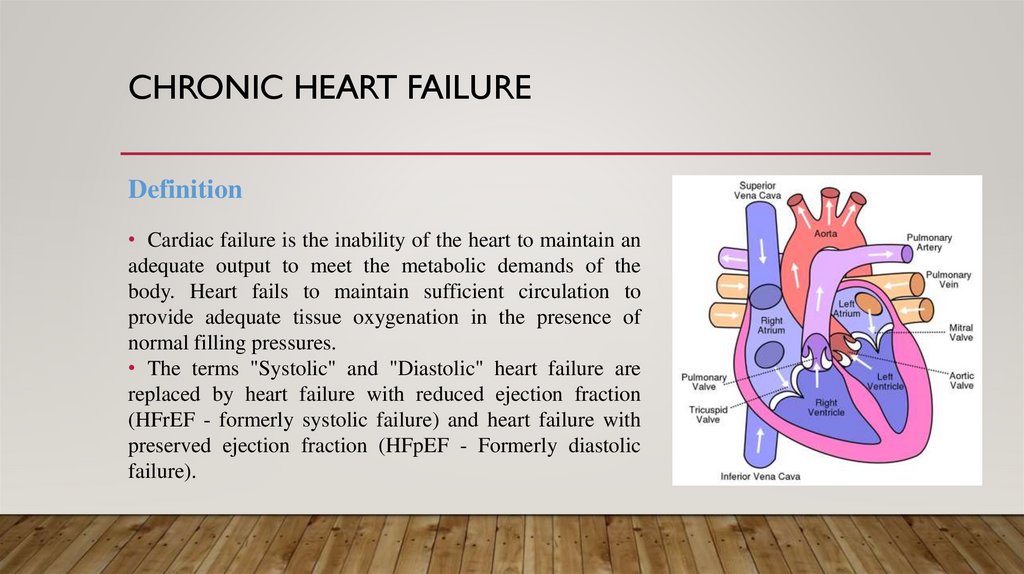
CHRONIC HEART FAILUREDefinition
• Cardiac failure is the inability of the heart to maintain an
adequate output to meet the metabolic demands of the
body. Heart fails to maintain sufficient circulation to
provide adequate tissue oxygenation in the presence of
normal filling pressures.
• The terms "Systolic" and "Diastolic" heart failure are
replaced by heart failure with reduced ejection fraction
(HFrEF - formerly systolic failure) and heart failure with
preserved ejection fraction (HFpEF - Formerly diastolic
failure).
3.
CHF - ETIOLOGY1) Reduced Ejection fraction (<40%)
2) Preserved Ejection Fraction (>40-50%)
3) High output states
A.
Reduced Ejection fraction (<40%)
• Coronary artery disease
– Myocardial infarction
– Myocardial ischaemia
• Chronic pressure overload
– Hypertension
– Obstructive valvular disease
• Chronic volume overload
– Regurgitation valvular disease
– Shunt lesions
– Extracardiac Shunting
• Chronic lung disease
– Corpulmonale
– Pulmonary vascular disorders
• Non-ischaemic dilated cardiomyopathy
– Familial / Genetic disorders
– Infiltrative disorders
• Toxic/drug induced damage
– Metabolic disorders
– Viral
• Chaga's disease
• Disorders of rate and rhythm
• Chronic tachyarrythmias
4.
CHF - ETIOLOGYB.Preserved Ejection Fraction (>40-50%)
• Pathologic hypertrophy
– Primary hypertrophic cardiomyopathy
– Secondary to Hypertension
– Ageing
• Restrictive Cardiomyopathy
– Infiltrative disorders (Amyloidosis,Sarcoidosis)
– Storage disorders
• Fibrosis
• Endomyocardial disorders
C.High output states
• Metabolic disorders
– Thyrotoxicosis
– Nutritional (Beriberi)
• Excessive blood flow requirements
– Systemic arteriovenous shunting
– Chronic anemia
5.
CHF - PATHOPHYSIOLOGYPathophysiology
• Low cardiac output leading to organ hypoperfusion and
inadequate oxygen supply along with decreased cardiac reserve,
pulmonary and systemic venous congestion
• Compensatory adaptations
– Increase in left ventricular mass(LVH) and
Volume(dilation)
– Increased Systemic Vascular Resistance
– Activation of Renin-Angiotensin-Aldosterone and
Vasopressin (ADH) Systems.
Left ventricular Remodeling:• Alterations in myocyte biology
– Excitation-Contraction coupling
– Myosin heavy chain (Foetal) expression
– B-adrenergic desensitization
– Hypertrophy
– Myocytolysis
– Cytoskeletal proteins
• Myocardial changes
– Myocyte loss - necrosis, apoptosis, autophagy
– Matrix degradation and myocardial fibrosis
• Geometry alterations of LV chamber
– LV dilation with increased LV sphericity
– LV wall thinning and Mitral valve incompetence
Preload:Preload is the left ventricular end-diastolic pressure and it depends
on left ventricular compliance and venous return.
After load:Afterload is the left ventricular systolic wall tension that develops
during ventricular systole and is determined by aortic valve
resistance, the peripheral vascular resistance and the elasticity of
major blood vessels.
6.
CLASSIFICATION AND CLINICAL MANIFESTATIONCLASSIFICATION
1) High output and Low output Failure
2) Right and Left sided Heart Failure
3) Forward and Backward Heart Failure
4) Systolic and Diastolic Failure
Clinical Manifestations
• Major Criteria
• Minor Criteria
• Major/Minor criteria
7.
CLINICAL MANIFESTATIONMajor Criteria
* Paroxysmal Nocturnal dyspnoea
* Neck vein distension
* Crackles–Lung fields
* Cardiomegaly
* Acute pulmonary edema
* Third Heart sound– Gallop
* Increased Venous pressure(>16cm
H²O)
* Positive (+) Hepato- Jugular
reflex
Minor Criteria
* Peripheral(Extremity) Edema
* Nocturnal cough
* Dyspnoea on exertion
* Hepatomegaly
* Pleural Effusion
* Tachycardia
* Decreased vital capacity by 1/3
Major/Minor criteria
*Five days treatment causing weight loss
≥ 4.5kg
* For Diagnosis 1 Major + 2 minor
Criterias
8.
DIAGNOSIS1) Chest X-ray
2) ECG
3) Lab investigations
I. Chest X-ray:* Prominent Upper lobe veins(PCWP = 15mmHg)
* Kerley B lines(Engorged peripheral lymphatics seen in the lower lobe [PCWP = 20mmHg]
* Fluid in the fissures or interlobar effusion, known as "Phantom tumor" as it disappears with
the treatment of left sided Heart Failure
* Increase in broncho-Vascular markings( "Bat's Wing" or "Inverted moustache" sign)–
features of pulmonary oedema [PCWP:25mmHg]
* Pleural effusion may be bilateral and symmetrical, but if unilateral is usually right sided
* Cardiomegaly
9.
DIAGNOSIS2) ECG:* It shows Acute Brady or Tachyarrythmias
* It may shows Atrioventricular block
* The presence of left bundle branch block (LBBB)
on an ECG is a strong marker for diminished LV
systolic function.
3) Lab investigations:a) Complete Blood Count:Since anemia can exacerbate heart failure
b) Serum electrolyte and Creatinine:Before starting high dose diuretics
c) Fasting blood glucose:To evaluate possible Diabetes Mellitus
d) Thyroid Function Test:Since
Thyrotoxicosis
and
Hypothyroidism
results
in
Atrial
Fibrillation and Herat Failure respectively
e) Iron studies:To
screen
for
Hereditary
Hemochromatosis as a cause of Heart
failure
f) ANA:To evaluate for possible Lupus
g) Viral studies:If Viral Myocarditis is suspected
h) Cardiac Markers
i) BNP
10.
MANAGEMENTGeneral principles of Management are
1. Removal of precipitating causes i.e. anemia, arrhythmias, infection, smoking, alcohol; drugs
like– beta blockers, calcium channel blockers, NSAIDs, infective endocarditis, Hypertension,
myocardial infarction, pulmonary embolism, dietary and medical non-compliance
2. Correction of underlying causes, i.e congenital heart disease, rheumatic heart disease, IHD
3. Control of fluid and sodium retention
4. Enhancement of myocardial contractility
5. Reduction of pulmonary and systemic venous congestion
6. Minimisation of Cardiac workload
11.
MANAGEMENT1) Non-pharmacologic measures:a) Physical Rest:
In acute phase, absolute bed-rest is advised. Early ambulation is advocated to avoid deep vein thrombosis.
Prophylactic low dose heparin 5000U SC/IV BD can be given. Degree of activity can be decided depending on the
cardiac status.
b) Mental Rest:
Diazepam 2 to 5 mg twice or thrice daily is given for several days.
c) Oxygen: It improves oxygen delivery and relieves dyspnoea
d) Diet:
Small frequent feeds instead of large meals and optimal calories depending on the nutritional status of the patient.
• Sodium restriction: In severe cases, sodium is restricted to 500mg/day and subsequently it can be increased to 2-3
mg/day with the usage of potent diuretics.
• Water restriction: 1-1.5 litres/day is permitted. Strict fluid restrictions is critical when serum sodium is less than
130mEq/L to prevent arrhythmias and neurologic abnormalities. Water intake maybe as libitum in all but the most
severe forms of CCE.
e) Dialysis and Ultrafiltration:
This procedure is indicated in severe HF with renal dysfunction. Therapeutic paracentesis, phlebotomy, rotating
tourniquet are other mechanical methods of fluid removal which are useful in the management of refractory failure.
12.
MANAGEMENT2) Pharmacologic Therapy
A) Diuretics
B) Vasodilator Therapy
A) Diuretics
a) High potency loop diuretics (Furosemide,
Bumetanide, Ethacrynic acid)
Dose:• Furosemide–40 to 200 mg/day
• Bumetanide–0.5 to 2 mg- maximum 10mg/day
• Ethacrynic acid–25 to 100 mg/day
• Torsemide–5 mg IV/10 mg Two time per day
b) Medium potency thaizide diuretics:- For Mild cardiac failure and in presence of normal
renal function.
Dose:• Chlorothiazides–250 to 500 mg/day
• Hydrochlorothiazide–25to 100 mg/day
• Chlorthalidone–25 to 100 mg/ day
• Metolazone–2.5 to 20 mg/day
• Indapamide–5 to 10mg/day
• Bendroflumethiazide–5 mg PO daily
• Benthiazide–25 mg PO 2 times daily
• Hydroflumethiazide–50 mg PO daily
• Methyclothiazide–2.5 mg PO daily
c) Low potency potassium sparing diuretics: Contraindicated in in Renal Failure patients
Dose:
• Spironolactone–50 to 200 mg/day
• Triamterene–100 to 200 mg/day
• Amiloride–5 to 10 mg/day
d) Eplerenone:- Selective Aldosterone receptor antagonist 25mg daily
13.
MANAGEMENTB) Vasodilator Therapy
It is used to Minimise the Workload to the Heart
a) Oral vasodilators:* ACE inhibitors:- Inhibit the formation of angiotensin 2
* Nitrates:- They are predominantly Venodilators and are useful in CHD with HF
* Hydralazine:- Arterial dilator and it reduces the afterload. Useful in the presence of valvular regurgitant lesions with volume overload
* Adrenergic blockers
° Alpha blockers:- powerful vasodilators and they reduce the systemic vascular resistance and thereby reduce the afterload
° Beta blockers: The adverse effects of endogenous catecholamines on the failing heart can be antagonized by by beta blockers. Beta blockers
with ISA activity like pindolol, Xamoterol have been tried. A minimum of two months therapy is required to demonstrate improvement in
ejection fraction and exercise tolerance. The drugs approved for use in cardiac failure are carvedilol, metoprolol and bisoprolol.
* Calcium channel blockers: Even though they dilate the vascular smooth muscle, their negative inotropic effect limit the usage in HF.
Amlodipine and Felodipine are preferable than Verapamil and Diltiazem in the management of heart failure especially in the presence of
Diastolic dysfunction. They enhance the diastolic relaxation of the ventricle. They are absolutely contraindicated in Cardiac Failure with low
ejection fraction (below 40%)
14.
MANAGEMENTb) Parenteral Vasodilators
They are useful in severe HF. Central Hemodynamic monitoring and optimal titration of dosage are essential
• Nitroglycerin: It is potent venodilator and it relives systemic and pulmonary venous congestion. This drug is useful in
Myocardial infarction
Dose:- 10 to 200 microgram/minute
• Sodium nitroprusside: It is very useful in severe hypertensive heart failure and in valvular regurgitant lesions with volume
overload
Dose:- 10 to 300 microgram/minute
• Enalaprilat: It can be used in the dose of 1.25 to 5 mg IV six hourly. The indications and adverse effects are similar to oral
form of enalapril
• Recombinant BNP-Nesitride: It can be used as a parenteral vasodilators in a dose of 2 microgram/Kg IV bolus followed by
continuous IV infusion of 0.01-0.03 microgram/kg/minute.
• Ecadotril: It is an inhibitor of Neutral endopeptidase (NEP) which causes breakdown of BNP
15.
MANAGEMENT3) Digitalis:Digoxin is the most effective drug in the management of heart failure especially in the presence of
* Supraventricular tachycardia
* Dilated left ventricle
* Impaired systolic function
It causes reversible inhibition of sarcolemmal sodium-potassium adenosine triphosphate. This
enhances the myocardial contractility. It slows conduction and prolongs refractory period in Va node,
purkinje fibres and thus reduces the ventricular rate
Dose:Digitalising dose: Adult– 1 to 1.5 mg. Initiate with p.5 mg and follow it with 0.25 mg 4 times daily.
Maintenance dose: Digoxin–0.25 mg 2 times daily.
• Digoxin specific Fab antibody fragment: Fab antibody fragments are considered when other modes
of therapy fail. Each 40mg vial is given in the form of Infusion in 100 ml of normal saline in 30
minutes
Number of vials = Serum level × Weight in Kg/100
16.
MANAGEMENT4) Sympathomimetic Amines:Norepinephrine, epinephrine, isoprenaline, dopamine and dobutamine.
• Dopamine: It increases renal blood flow, GFR and sodium excretion by stimulating specific dopaminergic receptors at dose of
1 to 3 microgram/kg/minute. By stimulating beta¹adrenoceptprs at dose of 3 to 5 microgram/ kg/ minute, it increases the
myocardial contractility and
heart rate. At a higher dose of 5 to 10 microgram/kg/ minute it causes vasoconstriction.
• Dobutamine: It is a synthetic catecholamines with marked beta¹ and weak beta² and alpha receptor activity
Dose:- 2.5 mg to 10 microgram/ kg/ minute
5) Phosphodiesterase inhibitors:- (Amrinone, Milrinone, Enoximone, Primobendan)
They exert positive inotropic and vasodilator effect through the inhibition of phosphodiesterase 3 and which is a membrane
bound enzyme responsible for the breakdown of cyclic AMP.
Dose:
* Amrinone– 750 microgram/kg bolus followed by 2.5 to 10 microgram/kg/minute.
* Milrinone– 50 microgram/kg bolus followed by 0.5 to 0.75 microgram/kg/ minute
• Levosimendon: By increasing the sensitivity of Cardiac muscle to calcium, cardiac contractility is increased without a rise in
intracellular calcium- positive inotropic effect.
17.
MANAGEMENTDose:- Initial bolus dose 12 microgram/kg followed by maintenance dose 0.1 to 0.3 microgram/kg/min
Agents that decrease the Mortality in CHF:• ACE inhibitors
• Angiotensin receptor blockers
• Beta blockers
• Aldosterone antagonist
• Isosorbide dinitrate
• Hydralazine
Mechanical circulatory support:This maybe considered when medical measure fail either in transient Myocardial dysfunction or when alternative
procedures like CABG or Cardiac transplantation are planned
a) Intra-aortic balloon pump
b) Ventricular assist devices
c) Enhanced external counter pulsation
d) Resynchronization therapy/biventricular pacing
18.
1)CONGESTIVE HEART FAILURE HAS BECOME AN EMERGING EPIDEMIC THE IN THE WORLD TODAY,AFFECTING OVER 5 MILLION AMERICANS IN OUR COUNTRY ALONE.
2)PHARMACOLOGIC TREATMENTS ARE CONSIDERED A FIRST OPTION FOR ITS TREATMENT, BUT
WAVE OF NEW, SURGICAL COURSES OF TREATMENTS HAS BEGAN TO DEVELOP.
3)IT IS ESSENTIAL FOR CRITICAL APPRAISAL OF THESE SURGICAL THERAPIES SO THAT THEY CAN
BE OFFERED TO THE GROWING POPULATION SUFFERING FROM HEART FAILURE.
4)ALTHOUGH A COMPLETE HEART TRANSPLANT IS CONSIDERED TO BE THE GOLD STANDARD OF
TREATMENT FOR A FAILING HEART, THERE ARE FAR TOO FEW DONOR HEARTS TO SUPPLY AN EVER
GROWING POPULATION WHO POTENTIALLY COULD BENEFIT FROM THEM.
5)THIS IS WHY IT IS CRUCIAL TO SEEK OTHER APPROACHES TO CORRECTING THIS PROBLEM.
6)DIAGNOSIS AND TREATMENT OF CHF REMAIN IMPORTANT AND CHALLENGING AND THE
UTILIZATION OF AVAILABLE SOURCES AND SOUND UNDERSTANDING OF THE PATHOPHYSIOLOGY
AND PHARMACOTHERAPY CAN PRODUCE REWARDING RESULTS WHEN CARING FOR THIS
FREQUENTLY ENCOUNTERED AND EVER CHALLENGING DIVERSE PATIENT GROUP.