











 medicine
medicineSimilar presentations:


")







Асute viral hepatitis B (VHB)
1.
АСUTE VIRAL HEPATITIS B (VHB)F. Hepadnaviridae, G. Orthohepadnavirus.
Virus has the spherical form by a size 42 nm, is covered
lipoproteinal envelope with the thickness by 7 nm
(It is HBs Ag). The nucleocapsid (соre) has a diameter by
28 nm inside contains ring two-filamentous DNA. Internal
(+) chain on 25 - 40 % more shortly outside (-) chain.
Genome of VHB contains S, C, X, P genes.
The formation of main protein and his subtypes encodes
by genes S, pre-S1,pre-S2.
The protein pre-S2 has specific receptors to albumin,
which allocates on hepatocytes
The protein S 1 - carrier of a dominating antigenic site "a"
also answers for species specificity of a virus.
2.
3.
All these proteins are found out in plasma duringreplication of viruses!!!
• The gene C- encodes protein of a nucleocapsid HBcAg
(it is only inside hepatocytes), but his soluble antigenic
variety HBe Ag circulates in a blood and has 3 serovars
• Gene Х - the activator of all genes VHB, probably
induces appearance of a hepatocell carcinoma (these
patients have for high number anti-HBX!)
• The gene Р - occupies 80 % (-) chain DNA - encodes
DNA-polymerase, return transcriptase, ribonuclease
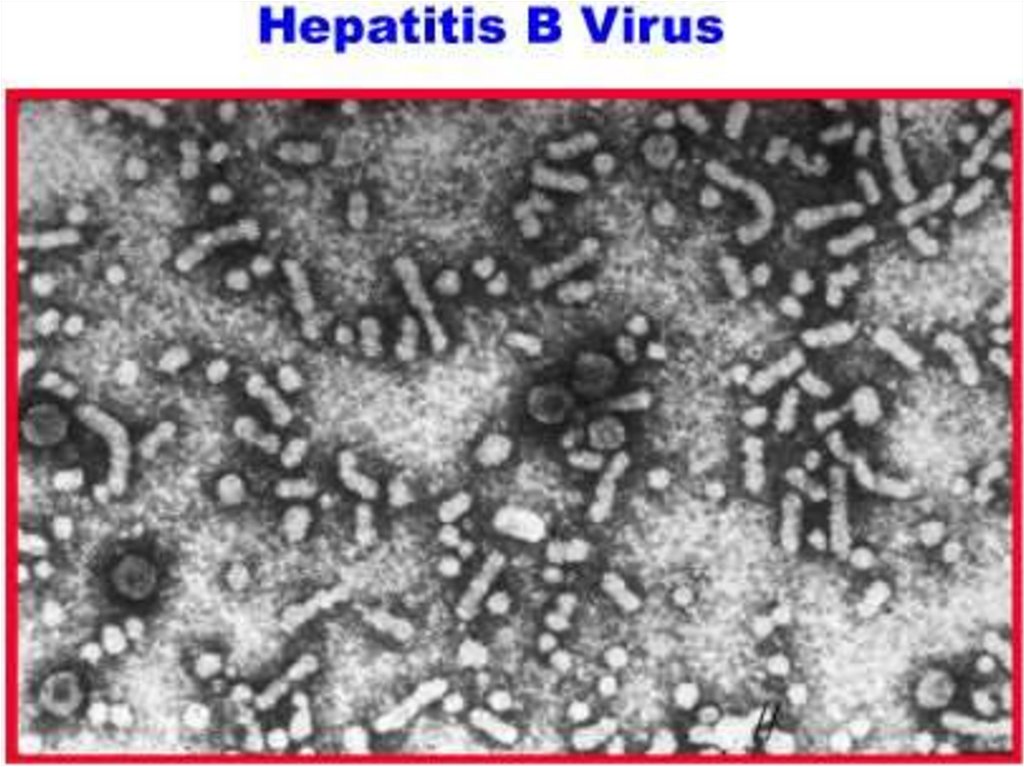
• The surface antigene НBsAg ( size from 22 up to 700 nm)
has 4 main subtypes (ayw, ayr, adw, adr)
4.
5.
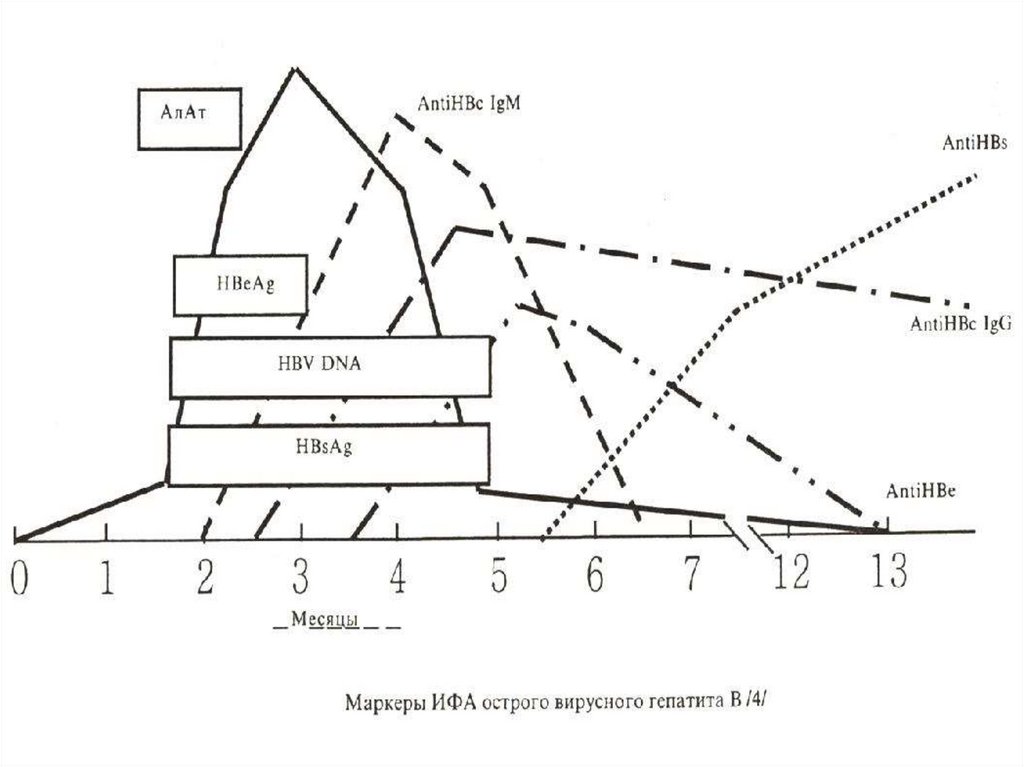
Against all antigenes the antibodies are worked outmajor markers of this hepatitis.
Cytopathic of effect virus - DOES NOT RENDER!!!
Is very steady in the environment, being inactivated:
- At room temperature - in 6 months
- At 60 dg. C- in 10 hours
- At 98 dg. C- in 20 minutes
- At 160 dg. C (dry fever) - in 1 hour
- In an autoclave (120 dg. С) - in 30 minutes
- In the dried up plasma - in 25 YEARS!!!
- In a refrigerator - in 6 months
- At рН 2.4 - in 2 hours
- In usual concentrations of disinfectant solutions through 2 - 7 days!!!
6.
EPIDEMIOLODY:33 % of the population of a planet transfer VHB and 350 400 millions from them have remained the carriers HBsAg!!
Groups of high risk
- Мedical workers, contacting with a blood
- Recipients of biological tissues of the man
- Patients with often parenteral infusions
- Mentally retarded and looking after staff
- Patients with chronic diseases of a liver
- Children birthing from the mothers - carriers HBsAg
- Drug addicts and prostitute
- Homosexuals and persons by HIV-infection
- Inhabitants hyperendemic on VHB of districts of a earth
7.
Frequency of revealing of markers VHB:- Among medical workers 33.3 %
- Among the patients with venereal diseases – 49.3 %
- Among the donors of a blood 14.5 %
- Among the population 3.8 %
The mode of transmission - PARENTERAL.
Natural modes of transmission:
- sexual 51.9 %
- intranatal and postnatal 1% - 10% - 50 %
- transplacental 6 - 10 %
- hemopercutaneus (home contacts) - 6 - 10 %
8.
2. Artificial of modes of transmission:- all medical manipulations with damage skins and
mucous
- IV drug addicts , tattoo, cosmetic procedures
Infection a dose of a blood - 0,00004 - 0,000001 ml.
Frequency infection newborn – 0.02 - 40 %
The hazard of a chronic carriage HBsAg after infection:
- at infection newborn - 90 %,
- 1-st year of life 50 %,
- is higher than 1-st year 20 %
- and for adult 5 - 10 %
The one injection of a blood with HBsAg - causes diseases
in 90 % of cases.
Hazard after a one prick of infection needle - 34 %
In 50 % of cases the source of an infection is not revealed!
9.
10.
11.
PATHOGENY1. Implantation of a virus after a sorption on surface
of a hepatocyte through protein pre- S2 by the
method endocytosis.
2. "«Undressing" of a virus and beginning of his
replication:
- the nucleocapsid is shaped in core of hepatocyte,
where through virus DNA-polymerase the chain (+)
is completed !!
- is shaped m - RNA (with the help cellular RNA-polymerase on which there is a copying at once (-), and
then and (+) chains
- synthesis of protein of the external envelope occurs
in cytoplasma
12.
3. The assembling of viruses is completed by a secretionin a blood soluble nucleocapsid HBeAg, which
decrease both cellular (lowering of production Interferons) and humoral (suppression formation antibody
and induction immunotolerance), which impedes his
going out from hepatocytes
4. Except for liver replication of a virus is possible in cells
of an marrow brain, spleen, monocytes and of lymphatic
tissue.
5. The immune answer at VHB corresponds immunopathological response - clinical form arise at particular activity Т-cellular immunity. When this immunity
depressed completely - the disease does not develop!!!
13.
6. The immune system of the host destroys:- hepatocytes, containing VHcAg,
- damages cells with protein pre-S2
- but is neutral to cells with HBsAg!!!
7. Humoral immunity formation of an antibody In the
following sequence:
- anti - HBc Ag Ig M, then IgG
- anti -pol and anti -pre S1
- anti -HBe Ag and anti -pre S2
- anti -HBs Ag (occur last)
- anti -HBxAg (are not reveald for all patients)
8. Can occur circulating immune complexes especial at
shape of the chronic forms hepatitis!!!
14.
15.
9. Except for immune cytolisis hepatocytes damage:- antibody - dependence immune cytolisis of hepatocytes, on surface which the complex antigeneantibody is shaped what increased activity by Tk –
lymphocytes
- autoantibodies against of a hepatic lipoprotein
- violation of a metabolism in the struck cells
CLINIC VHB
Incubation 80 days (from 40 about 200 days)
More often the patients have of average age (18 - 55 years)
Positive parenteral anamnesis or contact to carriers
HBs Ag
Step-by-step beginning of disease with long-lived
by preicteric period
16.
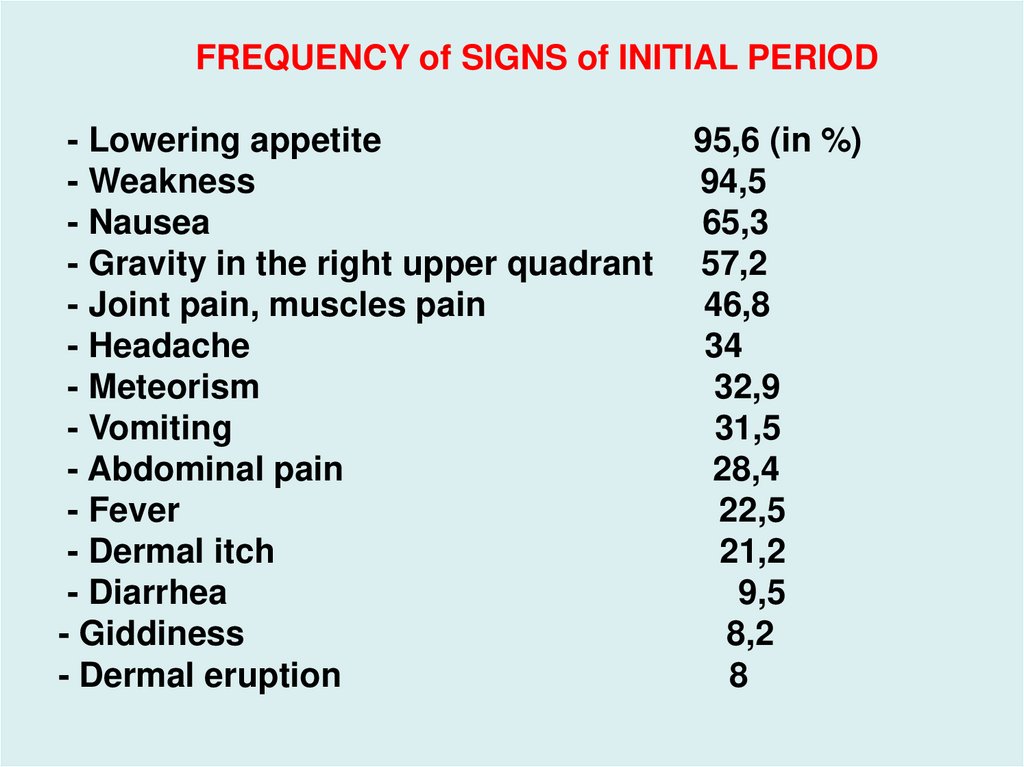
FREQUENCY of SIGNS of INITIAL PERIOD- Lowering appetite
- Weakness
- Nausea
- Gravity in the right upper quadrant
- Joint pain, muscles pain
- Headache
- Meteorism
- Vomiting
- Abdominal pain
- Fever
- Dermal itch
- Diarrhea
- Giddiness
- Dermal eruption
95,6 (in %)
94,5
65,3
57,2
46,8
34
32,9
31,5
28,4
22,5
21,2
9,5
8,2
8
17.
18.
With appearance of an icterus - intoxication intensify:- a nausea, vomiting, anorexia
- icteric colouring of a skin and scleras, dark urine,
decolorized feces,
- increase of a liver and lien for all patients.
VHB more often proceeds in the moderate form, but can
be both mild, and severe forms of disease .
Fulminant the form up to 2 %
Duration of icteric period from 1 about 12 weeks.
Cholestatic of the form of illness from 5 up to 15 %
Lingering current from 5 up to 10 %
The period of a reconvalescence can be delayed on
some months
19.
FULMINANT the FORMResults to acute hepatic unsufficiency and lasts from 2
about 8 weeks, being ended in 80 - 90 % of cases by death
of the patients. For it are characteristic:
- obstinate nausea and vomiting, anorexia
- progressing hemorrhagic syndrome
- fast decrease of sizes and density of a liver
- a "hepatic" smell of a skin and exhaled air
- a neutrophilic leukocytosis
- accelerated ESR
- decrease АLТ and АSТ, prothrombin Index
- Increase of a fraction of an indirect bilirubin
- increase of prothrombin time more 12 cek.
20.
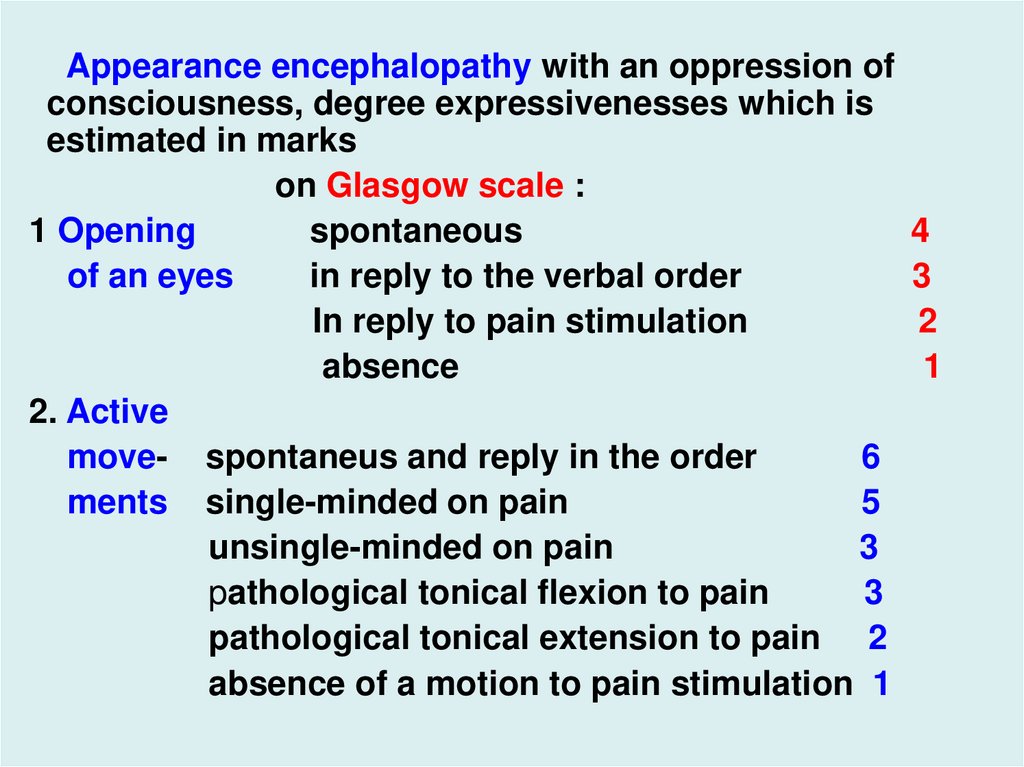
Appearance encephalopathy with an oppression ofconsciousness, degree expressivenesses which is
estimated in marks
on Glasgow scale :
1 Opening
spontaneous
of an eyes
in reply to the verbal order
In reply to pain stimulation
absence
2. Active
move- spontaneus and reply in the order
6
ments single-minded on pain
5
unsingle-minded on pain
3
pathological tonical flexion to pain
3
pathological tonical extension to pain 2
absence of a motion to pain stimulation 1
4
3
2
1
21.
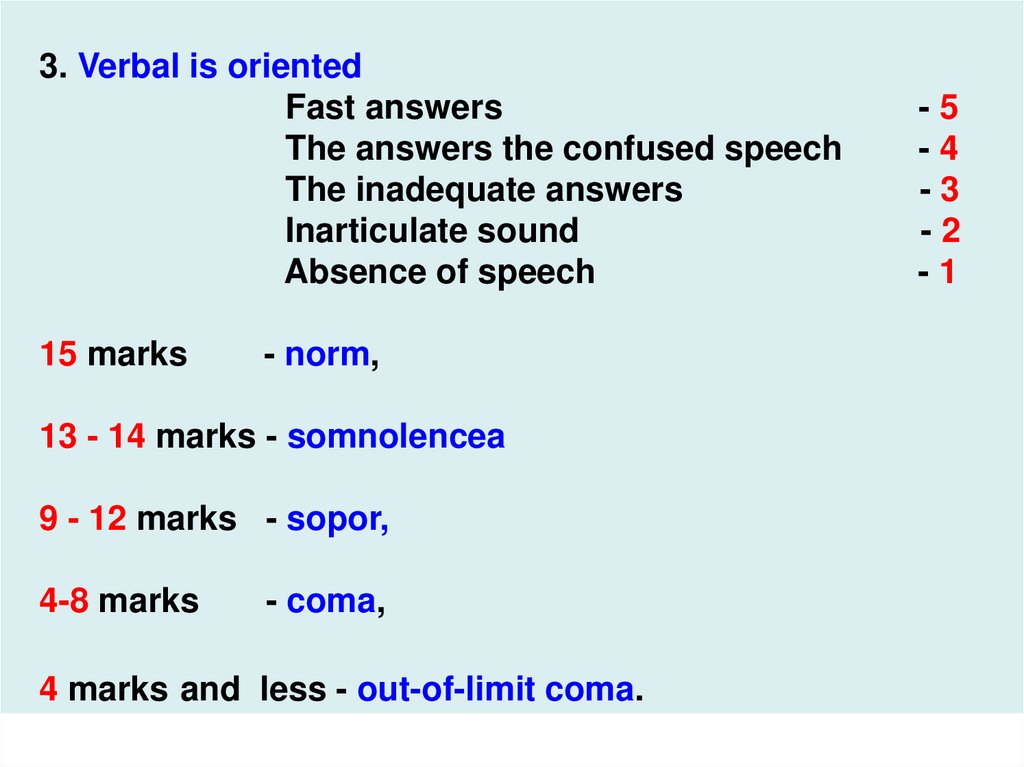
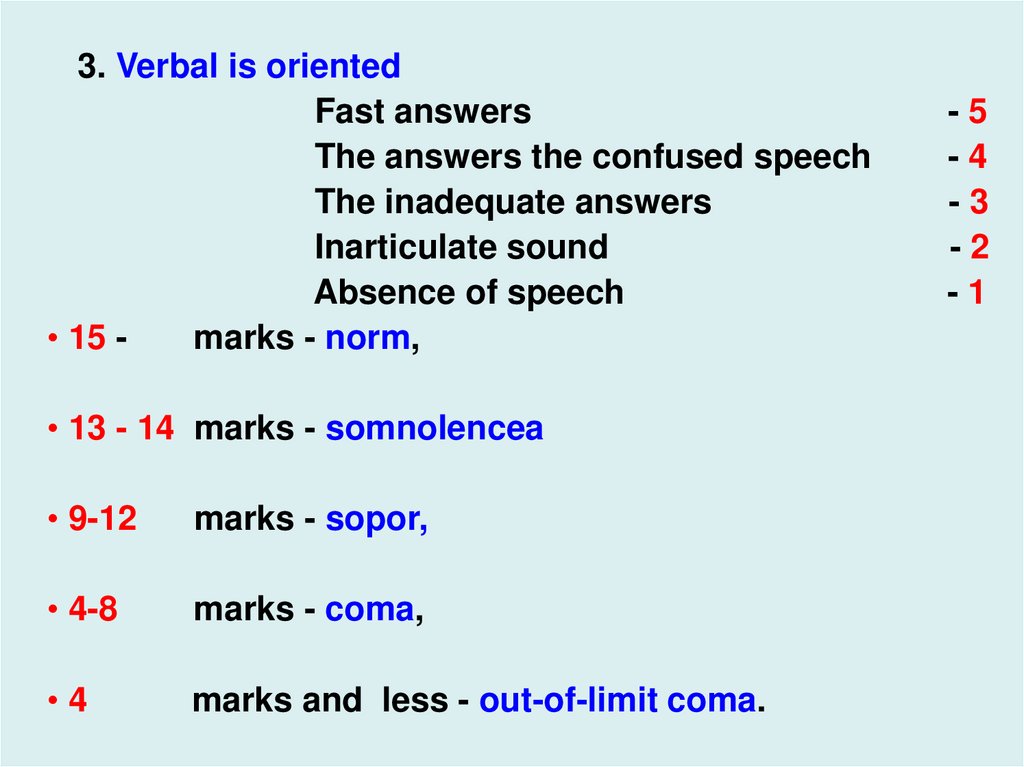
3. Verbal is orientedFast answers
The answers the confused speech
The inadequate answers
Inarticulate sound
Absence of speech
15 marks
- norm,
13 - 14 marks - somnolencea
9 - 12 marks - sopor,
4-8 marks
- coma,
4 marks and less - out-of-limit coma.
-5
-4
-3
-2
-1
22.
3. Verbal is orientedFast answers
The answers the confused speech
The inadequate answers
Inarticulate sound
Absence of speech
• 15 marks - norm,
• 13 - 14 marks - somnolencea
• 9-12
marks - sopor,
• 4-8
marks - coma,
•4
marks and less - out-of-limit coma.
-5
-4
-3
-2
-1
23.
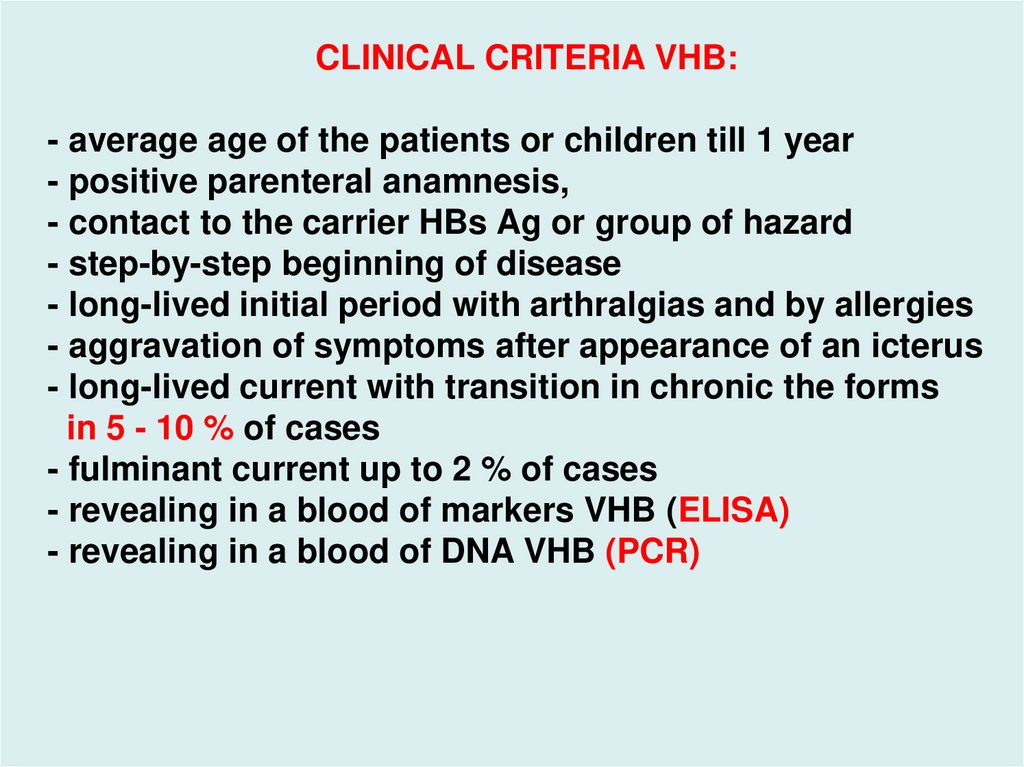
CLINICAL CRITERIA VHB:- average age of the patients or children till 1 year
- positive parenteral anamnesis,
- contact to the carrier HBs Ag or group of hazard
- step-by-step beginning of disease
- long-lived initial period with arthralgias and by allergies
- aggravation of symptoms after appearance of an icterus
- long-lived current with transition in chronic the forms
in 5 - 10 % of cases
- fulminant current up to 2 % of cases
- revealing in a blood of markers VHB (ELISA)
- revealing in a blood of DNA VHB (PCR)
24.
25.
26.
A 16-year-old Caucasian male born of a hepatitis B carriermother was incidentlly discovered to have serum HBsAg
and elevated ALT are AST. He denied any symptoms. His
liver was not palpable. Six months later he still had
elevated ALT values. Abdominal ultrasound examination
reavealed a normal liver and spleen. The needle biopsy shows
preservation of the lobular architecture. The portal area has moderate
degree of chronic inflammation with mononuclear cells.There is mild
piecemeal necrosis, the parenchyma shows foci of necrosis, and
several hepatosytes have uniformly pale eosinophilic cytoplasm
(ground glass cytoplasm ) indicating intracellular accumulation of
HBsAg.
Laboratory investigations: ALT- 312 U/L , AST- 164 U/L, Platelet
count - 250 x 10 in 9 dg., Bilirubin – 18.8 mmol/L, Albumin – 43 g/L,
HBV-DNA > 1,000 pg/mL., anti-HBc IgM –absent, HBsAg - present,
HBeAg – present, anti-HCV – absent
27.
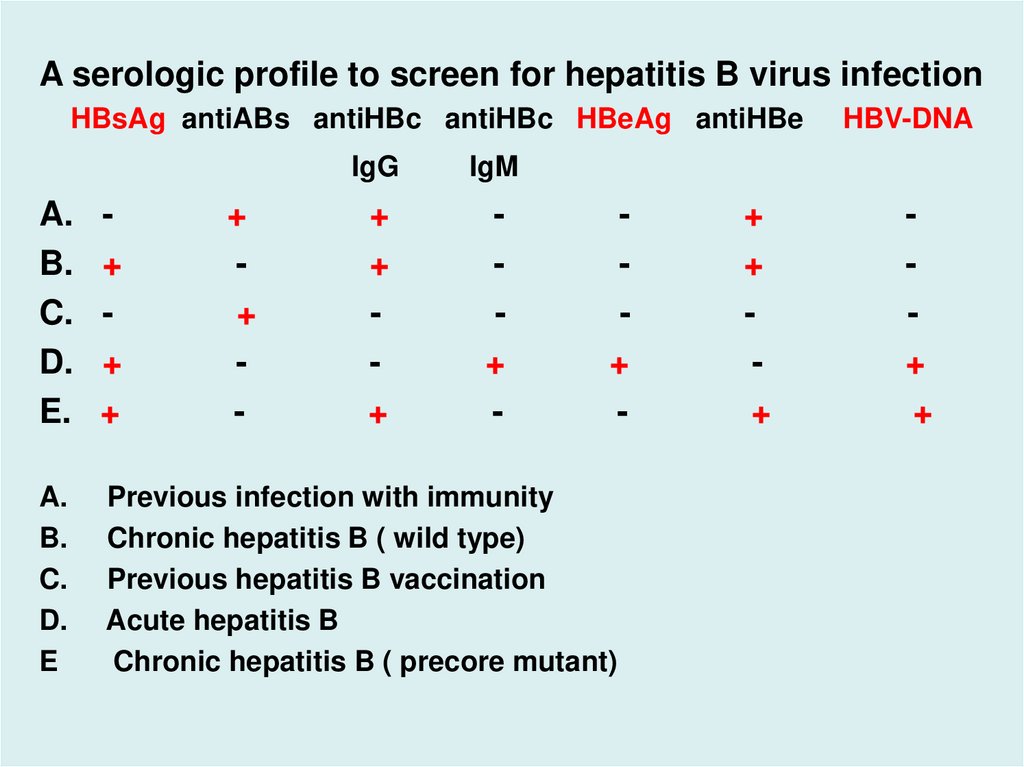
A serologic profile to screen for hepatitis B virus infectionHBsAg antiABs antiHBc antiHBc HBeAg antiHBe
+
+
-
IgG
IgM
+
+
+
+
-
A.
B.
C.
D.
E.
+
+
+
+
-
A.
B.
C.
D.
E
Previous infection with immunity
Chronic hepatitis B ( wild type)
Previous hepatitis B vaccination
Acute hepatitis B
Chronic hepatitis B ( precore mutant)
+
+
+
HBV-DNA
+
+
28.
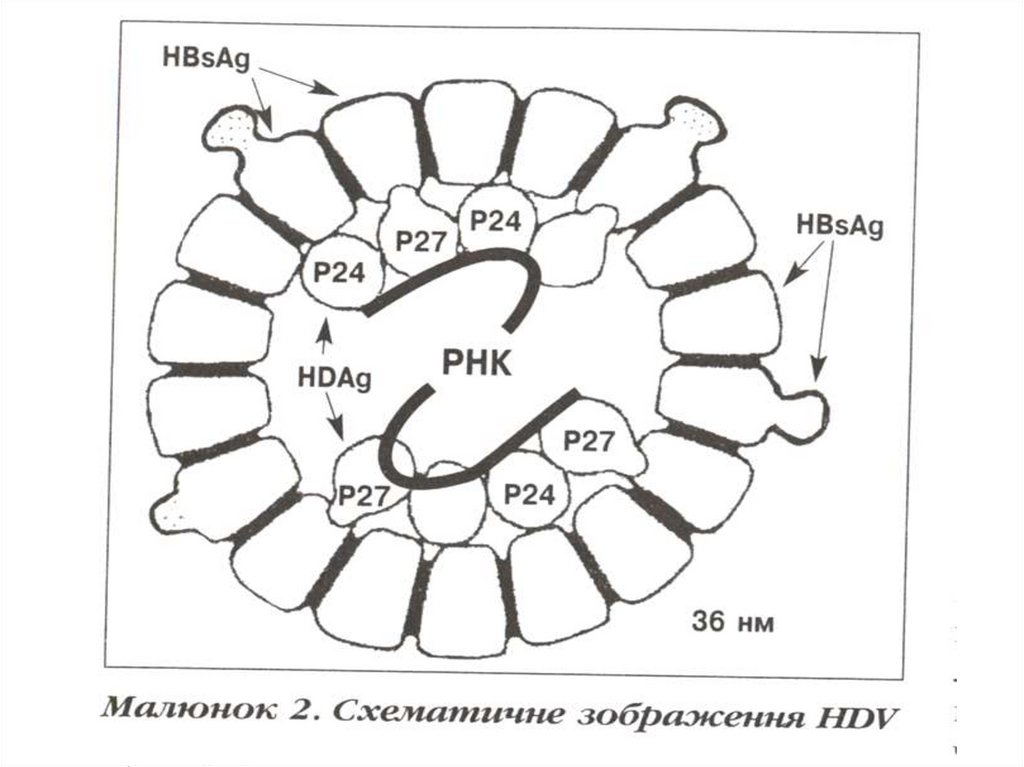
VIRAL HEPATITIS ДThe agent – RNA-virus by a size 28 - 39 nm with the
envelope consisting from HBs Ag.
RNA of the virus is surrounded HDV core Ag.
In a blood of the patients transmute in rodshaped
inbranched the form.
Is steady against warming, operation of acids and
proteinases, but fails by alkalis and nucleases.
HDV - is selected only from the patients infection HBV.
The monoinfection VHD is impossible!!!
Can cause disease only in a combination with VHB as
coinfection or superinfection
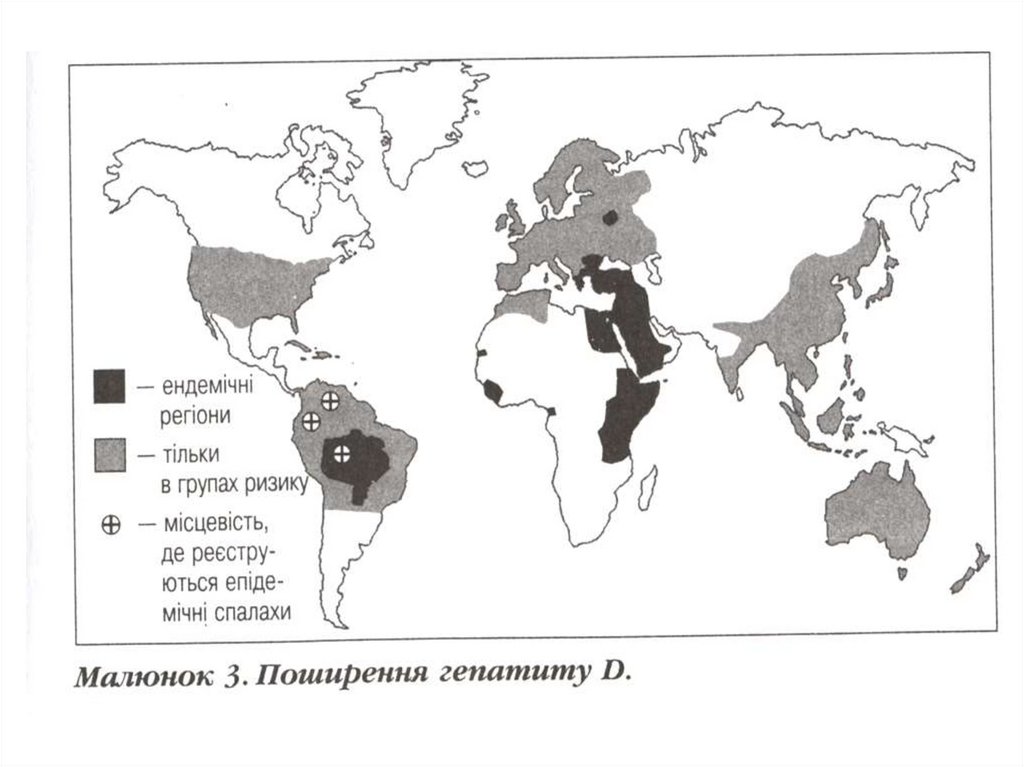
EPIDEMIOLOGY
- 15 million of carriers VHD are in the world. It is revealed:
- among carriers HBs Ag – in 9 % of cases
- and among the patients with chronic VH - in 10 - 30 % of
cases
29.
30.
31.
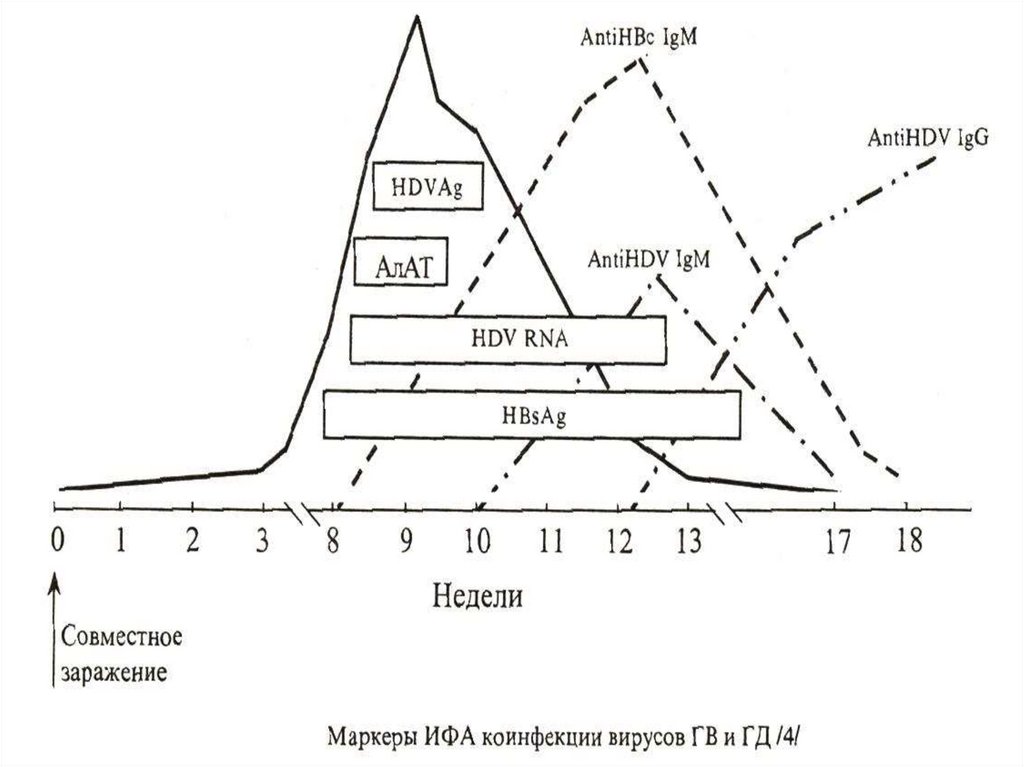
CLINIC. Incubation interval 80 days (40 - 200 days)Coinfection - simultaneous infection HBV and HDV.
Clinical manifestations of VHD differs from a VHB little, but
more often:
- high temperature from 3 to 5 days and long-lived 37,2 –
37,8 dg.С the one registers .
- more often complain of a pain in the right upper quadrant
- characteristicly two-undular current with peaking on 15 –
32 days of illness.
It more often revials among the recipients of a blood and
drug addicts.
Transform to a chronic hepatitis in 5 % of cases
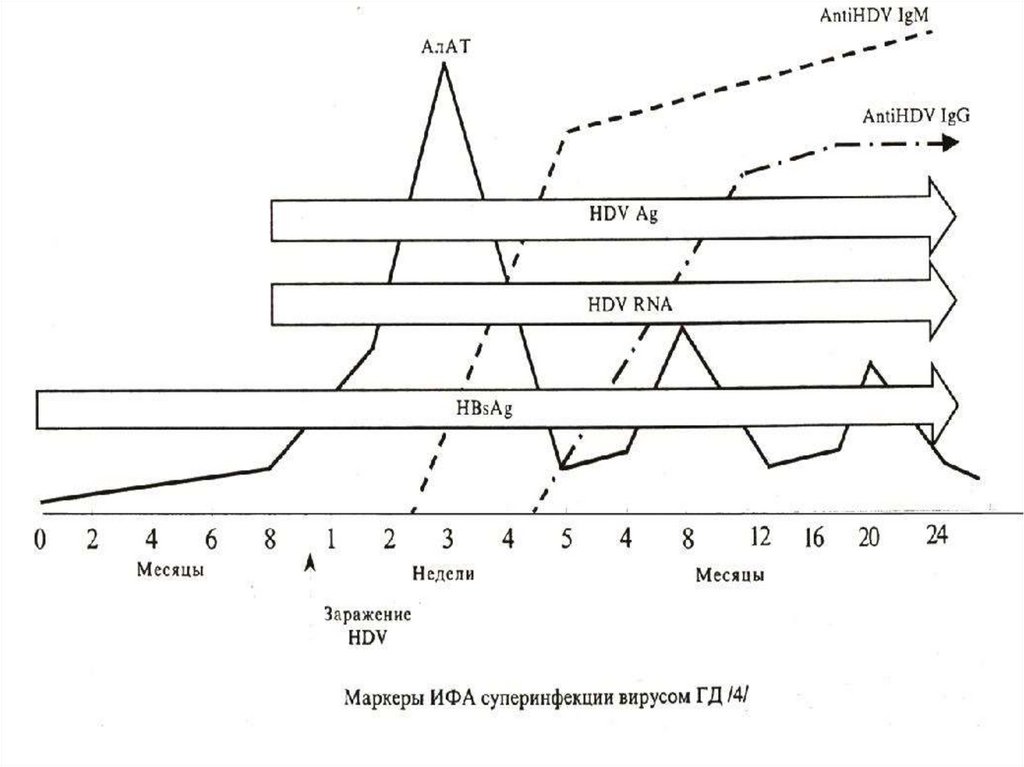
The superinfection develops for carriers HBsAg
After repeated hemotrasfusion and infection result aggravate a hepatitis with intensive reproduction of a virus
in hepatocytes.
32.
The severe current is registered for 60 % of the patientswith creation fulminant of the forms of disease.
More than 70 % becomes chronic carriers HDV,
Proceeding more hardly, than at VHB (frequently with a
hydropic - ascitic syndrome)
Passes in a cirrhosis for 60-70 % of the patients!!
CLINICAL CRITERIA VHD:
- Average age of the patients
- Hemotransfusion or carriage HBs Ag
- Acute beginning, short preicteric period with arthralgias
and allergies
- Aggravation of symptoms of the patients about
appearance icteruses
33.
34.
35.
- pain in the right upper quadrant in initial period- hepatospleenomegalia
- high and long-lived hyperbilirubinemia
- appearance of a hydropic - ascitic syndrome at
superinfections
- clinico-enzymatic peakings at coinfection
- severe current for 60 % of the patients and often
outcomes In a chronic hepatitis for 70 % at a
superinfection
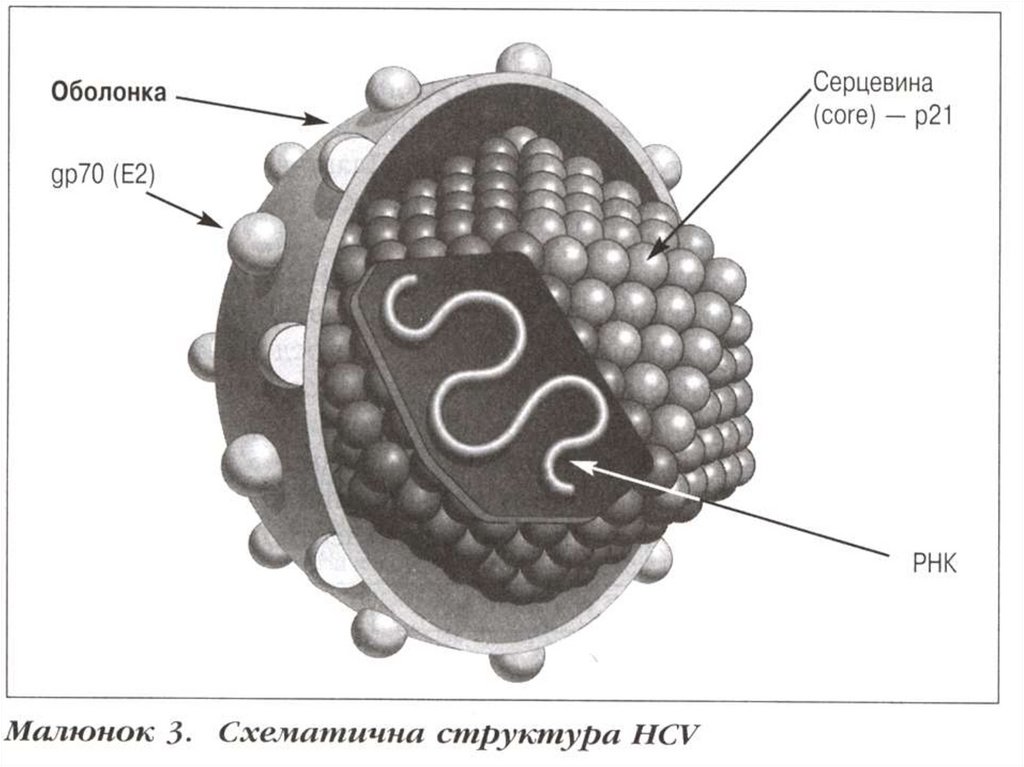
VIRAL HEPATITIS С:
The agent - cover spherical virus, size 35-50 нм.
(F. Togaviridae, G. Flavivirus.), Inside is one-filamentous
RNA (+), is covered by protein C.
36.
37.
38.
39.
40.
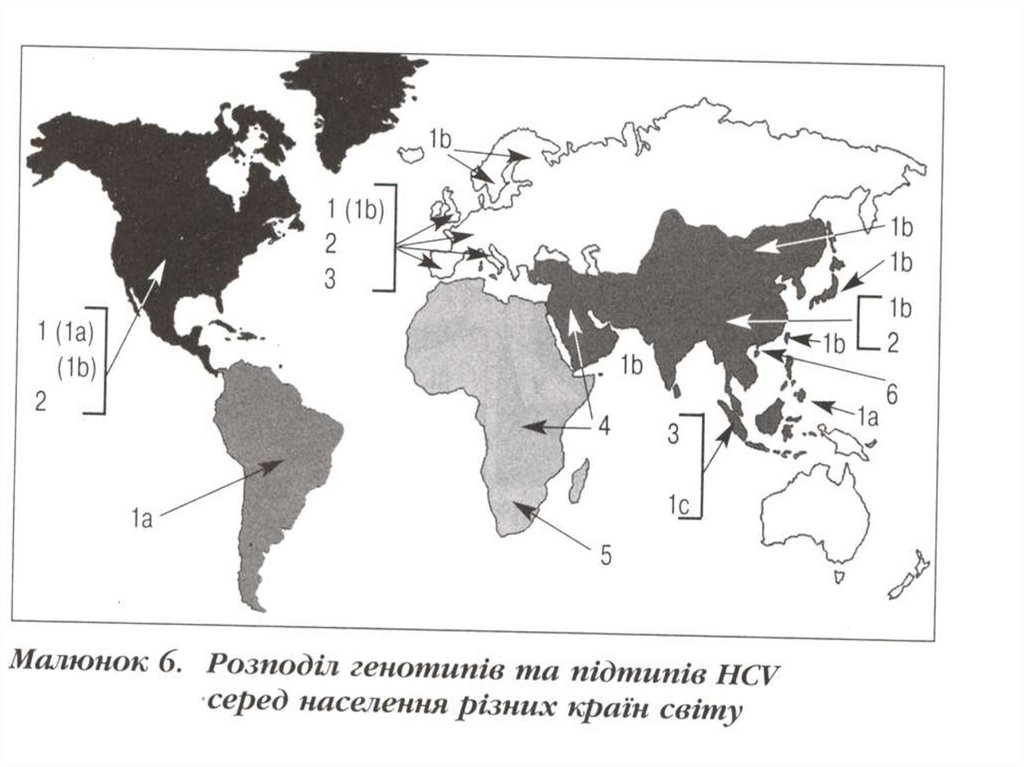
On a surface are posed glycoproteins Е. 6 genotypes of avirus are known. Is sensitive by fatty-solvent, 60 dg С
maintains - 30 minutes, boiling - 2 minutes
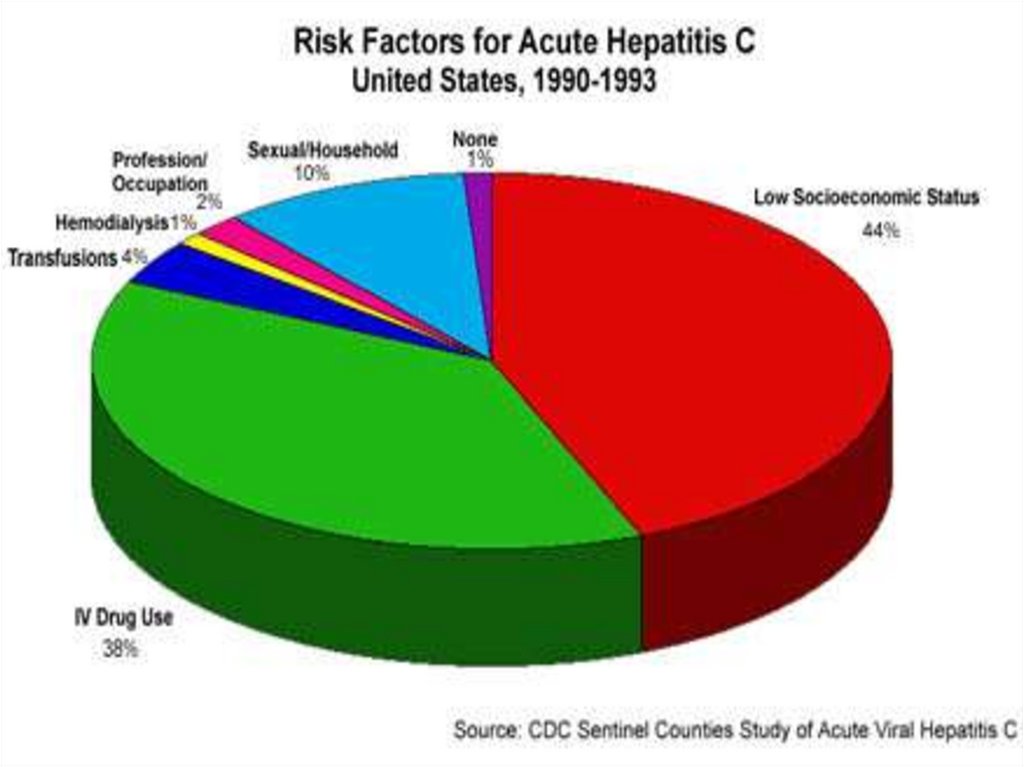
EPIDEMIOLOGY:
- is similar VHB, but is very seldom transmitted upright and
sexual way. it is posttrasfusion a hepatitis in 50 -60 %.
Mainly is average age of the patients. The data on quantity
in the world of carriers is great, but the figures are
contradictory (100 - 500 millions of man)
CLINIC.
An incubation 42 days (14 - 60 days)
Beginning step-by-step. Principal syndromes are dyspeptic
and astheno-vegetative. With appearance of an icterus the
state is aggravated, but is less significant, than at VHB.
41.
CLINICAL CRITERIA VHC:- average age of the patients
- In an anamnesis hemotrasfusions or contact to the ill
patient
- step-by-step beginning
- aggravation of symptoms with appearance of an icterus
- moderate increase of a bilirubin and liver
- transition in 50 - 80 % of cases in the chronic form with
the subsequent flaccid current ( “affectionate”
the murderer)
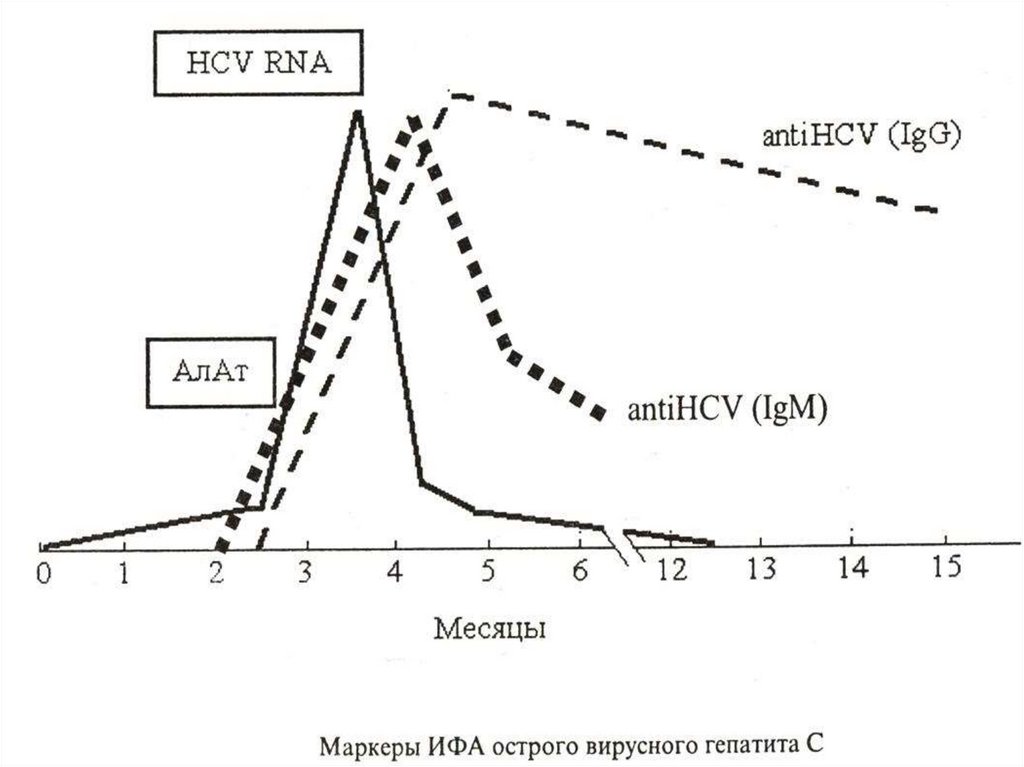
- antibodies occurs late, in 5 years of an antibody
do not influence to replication of a virus
- It are found out of antibodies- ELISA and RNA- PCR
42.
43.
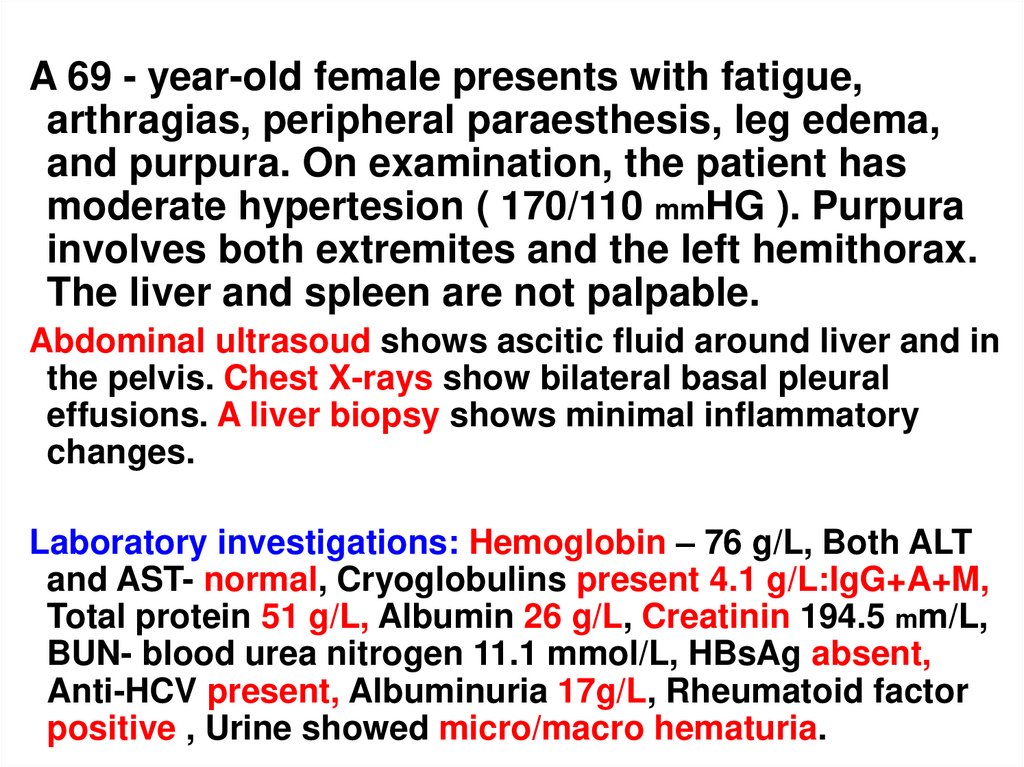
A 69 - year-old female presents with fatigue,arthragias, peripheral paraesthesis, leg edema,
and purpura. On examination, the patient has
moderate hypertesion ( 170/110 mmHG ). Purpura
involves both extremites and the left hemithorax.
The liver and spleen are not palpable.
Abdominal ultrasoud shows ascitic fluid around liver and in
the pelvis. Chest X-rays show bilateral basal pleural
effusions. A liver biopsy shows minimal inflammatory
changes.
Laboratory investigations: Hemoglobin – 76 g/L, Both ALT
and AST- normal, Cryoglobulins present 4.1 g/L:IgG+A+M,
Total protein 51 g/L, Albumin 26 g/L, Creatinin 194.5 mm/L,
BUN- blood urea nitrogen 11.1 mmol/L, HBsAg absent,
Anti-HCV present, Albuminuria 17g/L, Rheumatoid factor
positive , Urine showed micro/macro hematuria.
44.
1. A 48 – year-old male developed an attack of angina forwhich he underwent a thorough investigation.
Biochemical liver tests revealed an ALT of 184 U/L, AST
of 104 U/L, and a positive anti – HCV test result. He
denied risk factors for hepatitis. His wife was anti-HCV
negative but his brother was found to be anti-HCV
positive. Both of his parents died of cause unrelated to
hepatitis. The liver was not palpable. His abdominal
ultrasound was normal.
A liver biopsy shown: enlaged portal tracts with predominantly
lymphocytic infiltration. Lymphocytes are arranged in a follicle-like
structure. The limiting plate is preserved. Bile ducts are slightly
elongated. Liver cells are arraged in regular one-cell-thick plates.
Laboratory investigations:
Bilirubin – 13.68 mmol/L, Prothrombin time – 12.2 seconds,
Platelet count 215 x 10 in 9 dg./L, Ferritin – 620 ng/mL, Albumin 43 g/L, Cryoglobolins – absent, Tissue antibodies – absent, HB SAg
– absent, HCV-RNA type 1b - 1.850 x 10 in 6 dg. genomes /mL.
45.
TREATMENTThe mild forms - bed rest, diet N5, hepatoprotections,
vitamin therapy, PO desintoxication, antioxidants
Moderate forms: therapy as mild form + follow-up amplifies
desintoxication, the glucocorticoids (at VHB are more
often)
The severe forms:
- antiviral drugs (interferons, vidarabin, lamivudin,( is rare)
- immunodepretion drugs at VHB (antilymphocytic
Immunoglobulin, glucocorticoids etc.)
- antiferment drugs and antifibrinolytic drugs
-Intensifying desintoxication (exception of a diet of a
protein)
46.
Hemosorption, enterosorbents , streptomycin 2- 4 gr PO,drugs of a levulose etc.
At encephalopathy – glutamic an acid, glutargin, sodium a
hydroxybutyrate)
Thrombocytopenia a hemorrhagic syndrome
(vitamin C (antiscorbutic factor) and vitamin K ( antihemor
-rhagic factor) acidum aminocapronicum, etamsylatum
sodium
Coagulopathy and hemorrhagic syndrome – at 1st stage DIC
heparinum for 1000 U/HOUR IV
For decrease of a hypoxia of tissues (oxygenium, calcium
pangamat, cytochrome C 10 мг/kg)
For improvement of a metabolism (spleninum, riboxinum,
orotat of a potassium, cocarboxylase etc.)
47.
For unloading a small circle of a circulation - lasixum,euphyllinum, sulfocamphocainum, cardiac glycosides
At an inefficiency of treatment – makes of a liver grafting
PROPHYLAXIS
-To keep general purpose standards precautions by
operation with the biological preparations
To test a donor blood, bodies, semen
-Vaccinal prevention from VHB and VHD (Engerix B etc.)
in a dose 20 mkg with an interval 0 - 1 - 6 months
Sanitary - educational operation
48.
49.
1. A 48 – year-old male developed an attack of angina for which heunderwent a thorough investigation. Biochemical liver tests
revealed an ALT of 184 U/L, AST of 104 U/L, and a positive anti –
HCV test result. He denied risk factors for hepatitis. His wife was
anti-HCV negative but his brother was found to be anti-HCV
positive. Both of his parents died of cause unrelated to hepatitis.
The liver was not palpable. His abdominal ultrasound was normal.
A liver biopsy shown: enlaged portal tracts with predominantly
lymphocytic infiltration. Lymphocytes are arranged in a follicle-like
structure. The limiting plate is preserved. Bile ducts are slightly
elongated. Liver cells are arraged in regular one-cell-thick plates.
1.
2.
3.
Laboratory investigations:
Bilirubin – 13.68 mmol/L, Prothrombin time – 12.2 seconds, Platelet count
215 x 10 in 9 dg./L, Ferritin – 620 ng/mL, Albumin - 43 g/L, Cryoglobolins
– absent, Tissue antibodies – absent, HB SAg – absent, HCV-RNA type
1b - 1.850 x 10 in 6 dg. genomes /mL.
What is the diagnosis?
Comment on the virological data?
Should this patient be treated?
50.
• 251.
52.
53.
54.
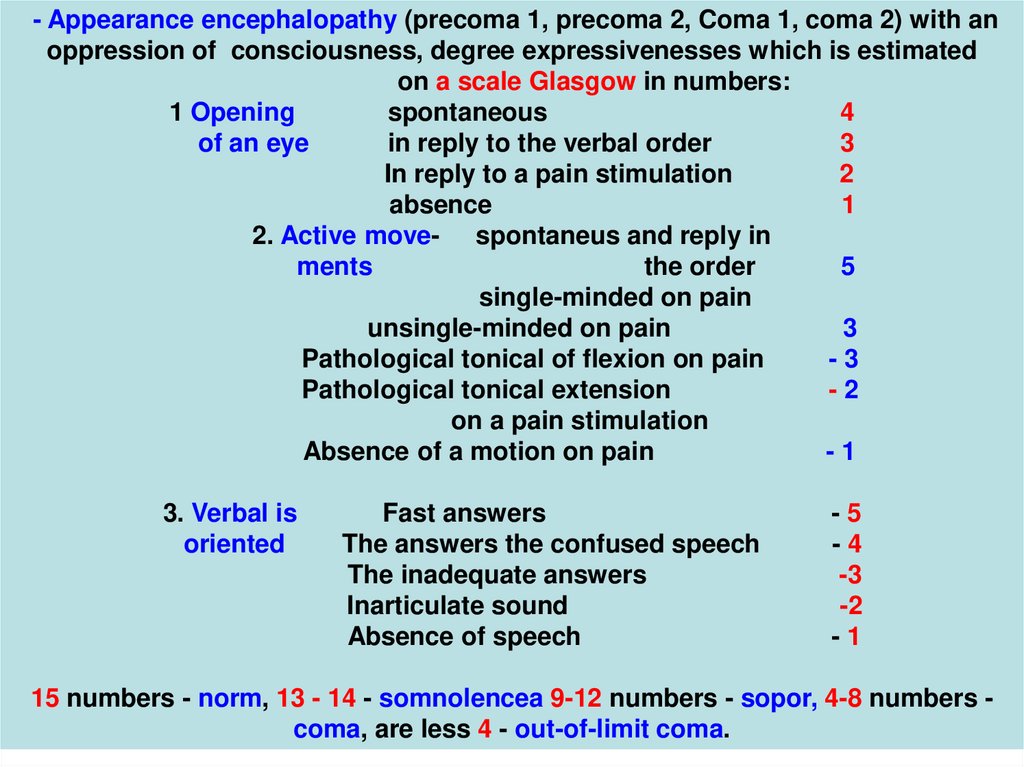
- Appearance encephalopathy (precoma 1, precoma 2, Coma 1, coma 2) with anoppression of consciousness, degree expressivenesses which is estimated
on a scale Glasgow in numbers:
1 Opening
spontaneous
4
of an eye
in reply to the verbal order
3
In reply to a pain stimulation
2
absence
1
2. Active move- spontaneus and reply in
ments
the order
5
single-minded on pain
unsingle-minded on pain
3
Pathological tonical of flexion on pain
-3
Pathological tonical extension
-2
on a pain stimulation
Absence of a motion on pain
-1
3. Verbal is
oriented
Fast answers
The answers the confused speech
The inadequate answers
Inarticulate sound
Absence of speech
-5
-4
-3
-2
-1
15 numbers - norm, 13 - 14 - somnolencea 9-12 numbers - sopor, 4-8 numbers coma, are less 4 - out-of-limit coma.