
















 culturology
culturologySimilar presentations:

Asthma – an overview
1.
Asthma – an overview2.
Definition of asthma“A Chronic Inflammatory Disorder of the airways
… in susceptible individuals, inflammatory
symptoms are usually associated with widespread
but variable airflow obstruction and an increase in
airway response to a variety of stimuli.
Obstruction
is
often
Reversible,
either
spontaneously or with treatment.”
Diagnosis and natural history. Thorax 2003; 58 (Suppl I): i1-i92
3.
Adam and Eveand
Christopher Robin
4.
Eve is a 5-year old girl with:• Personal and family history of allergy
• Wheeze on laughing and exercise
• Severe attacks with colds
• Bronchodilator-responsive and dependent on inhaled
corticosteroid
• Persistent symptoms and PEF variability on a
depressed baseline
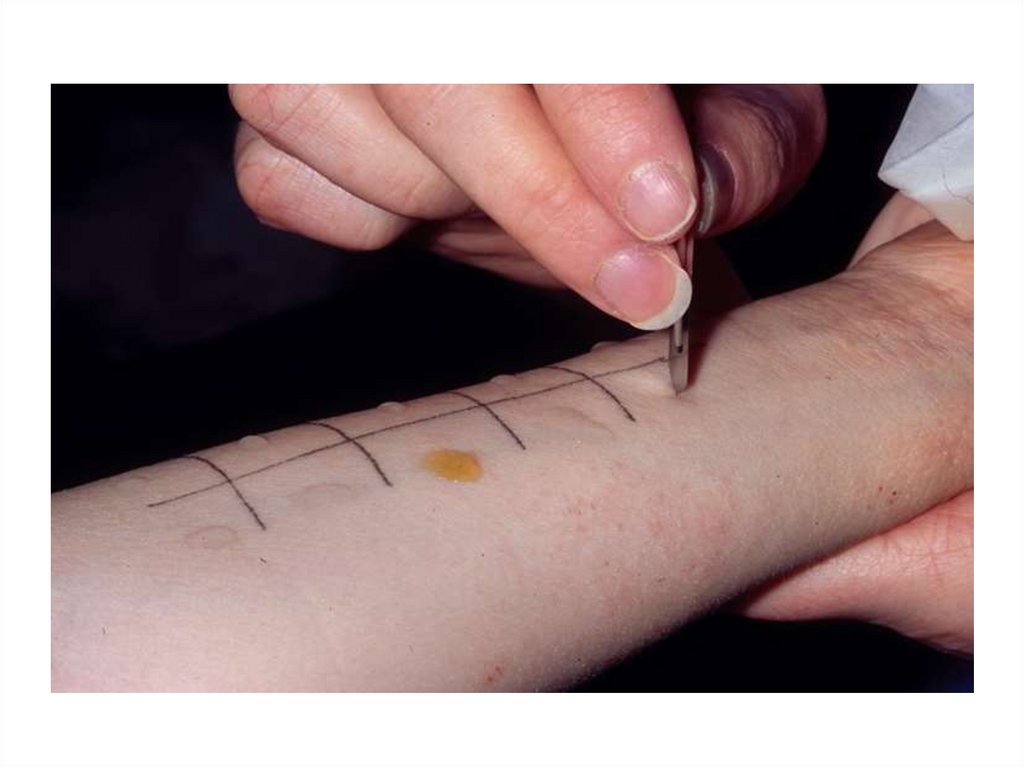
• Evidence of allergy
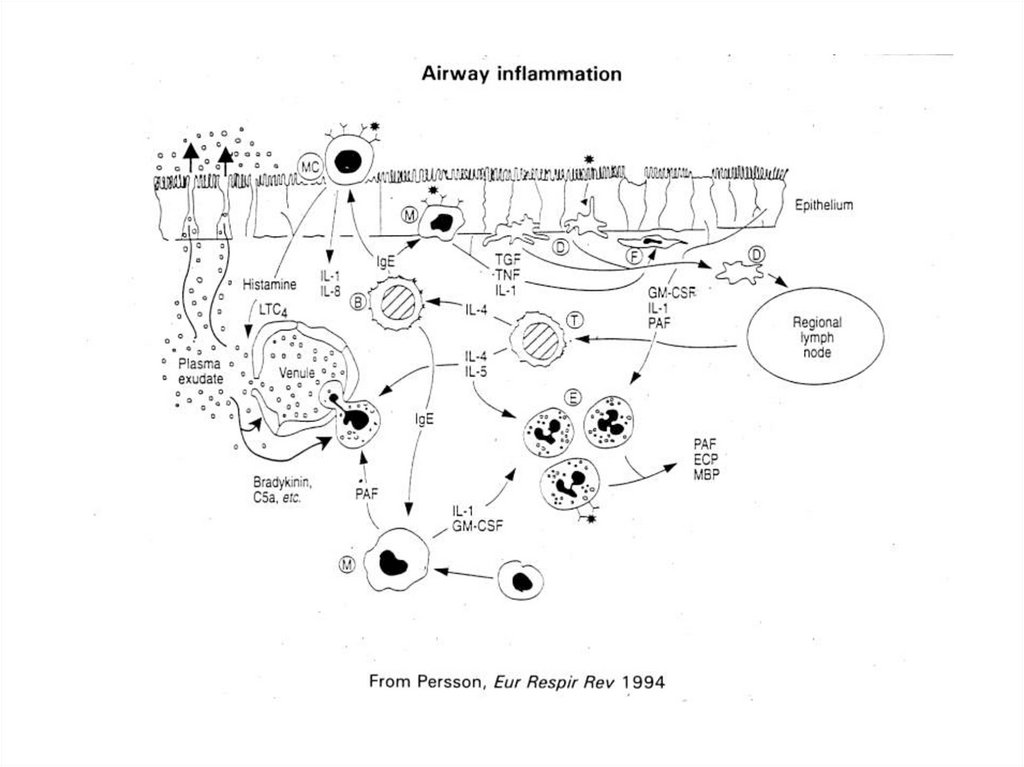
• Eosinophilic airway inflammation
• Evidence of allergy
• Eosinophil airway inflammation
5.
Adam is a 14-month old boy with:• A single, smoking non-allergic mother
• Multiple admissions to hospital with viral, episodic wheeze
• Poor response to nebulised ß agonist
• No symptoms between episodes
• No evidence of allergy
• No inflammation between episodes
6.
What is“Wheeze”?
7.
Flow limitation and wheezewall compliance
cross sectional
area
dissipation of energy
flutter
wheeze
8.
9.
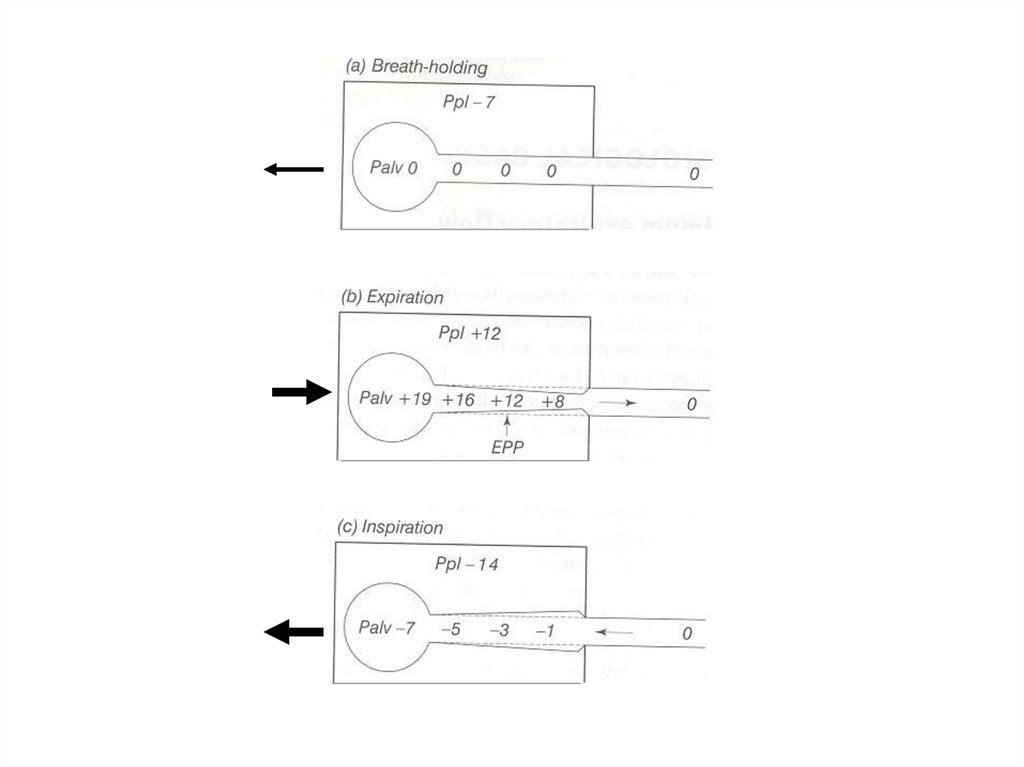
How can airway narrowingbe measured?
10.
11.
12.
13.
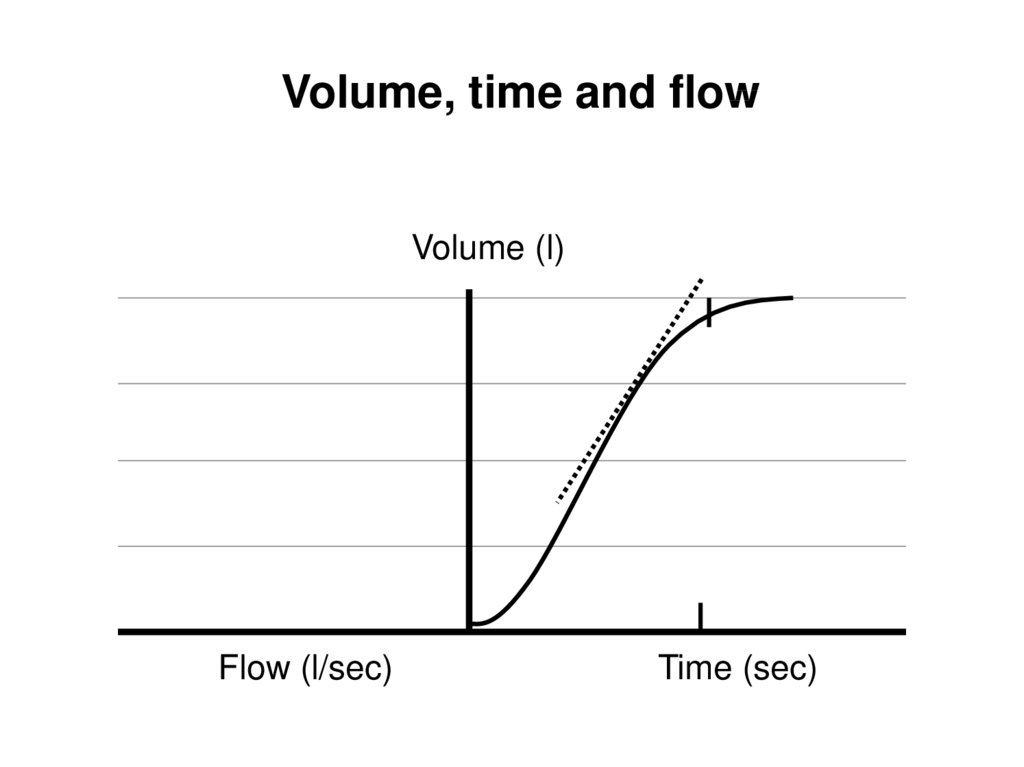
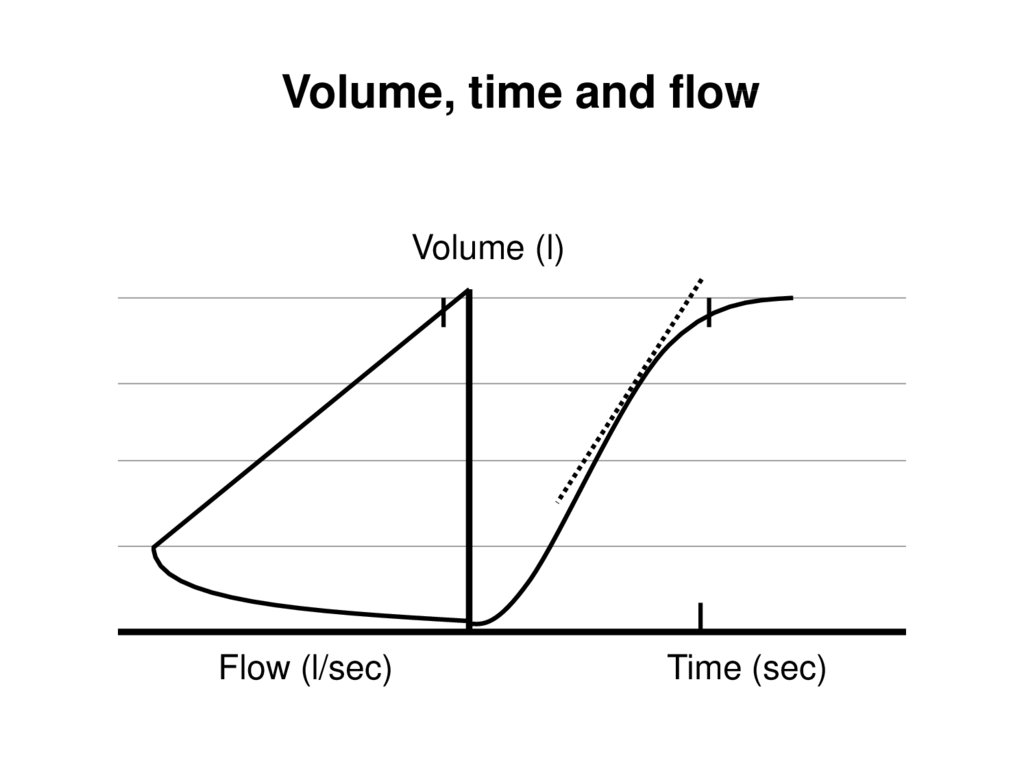
Volume, time and flowVolume (l)
Flow (l/sec)
Time (sec)
14.
Volume, time and flowVolume (l)
Flow (l/sec)
Time (sec)
15.
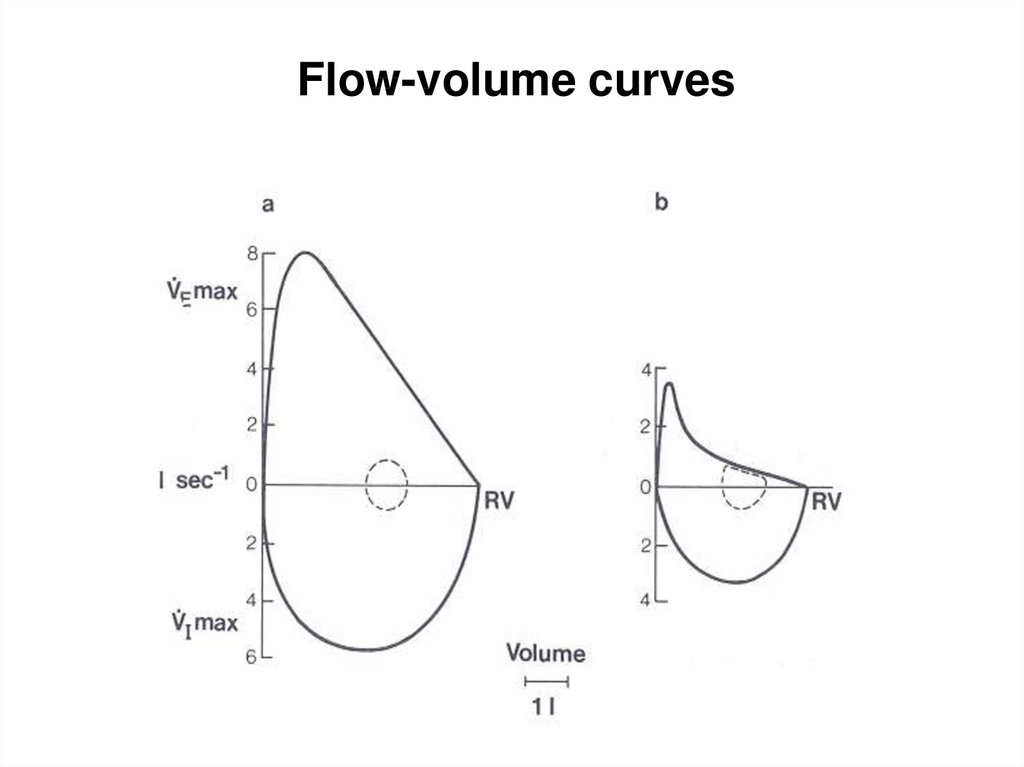
Flow-volume curves16.
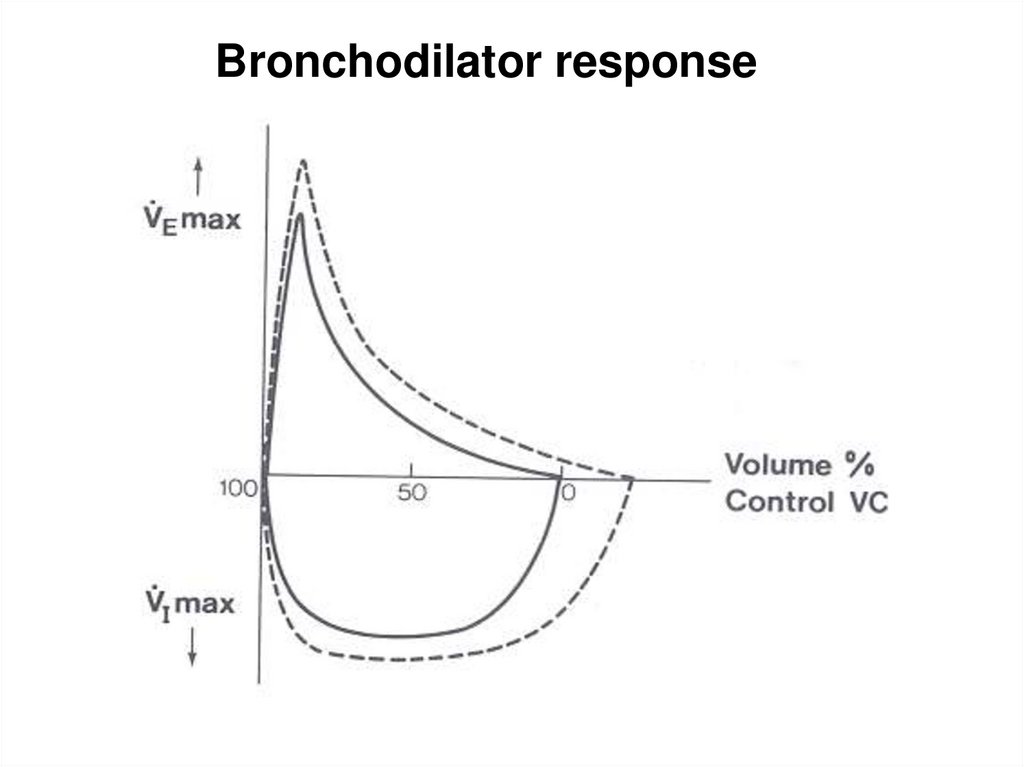
Bronchodilator response17.
What’s bronchialresponsiveness?
(or hyper responsiveness: BHR)
18.
Trigger+
Bronchial
responsiveness
Airway
narrowing
Wheeze,
cough &
dyspnoea
19.
20.
21.
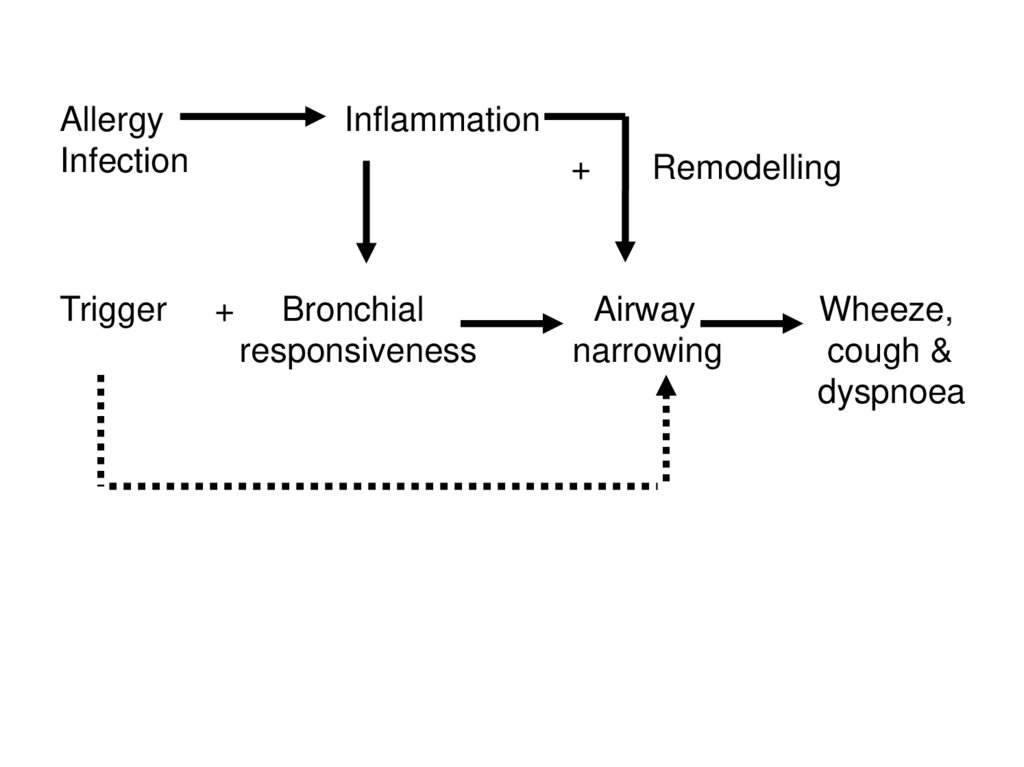
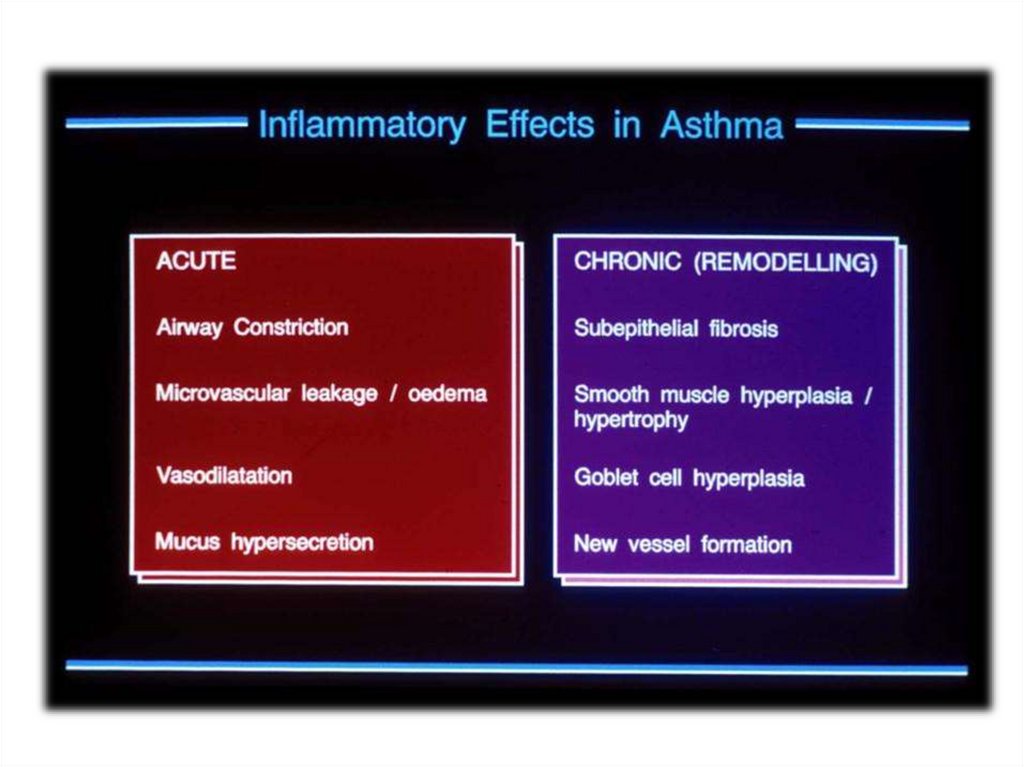
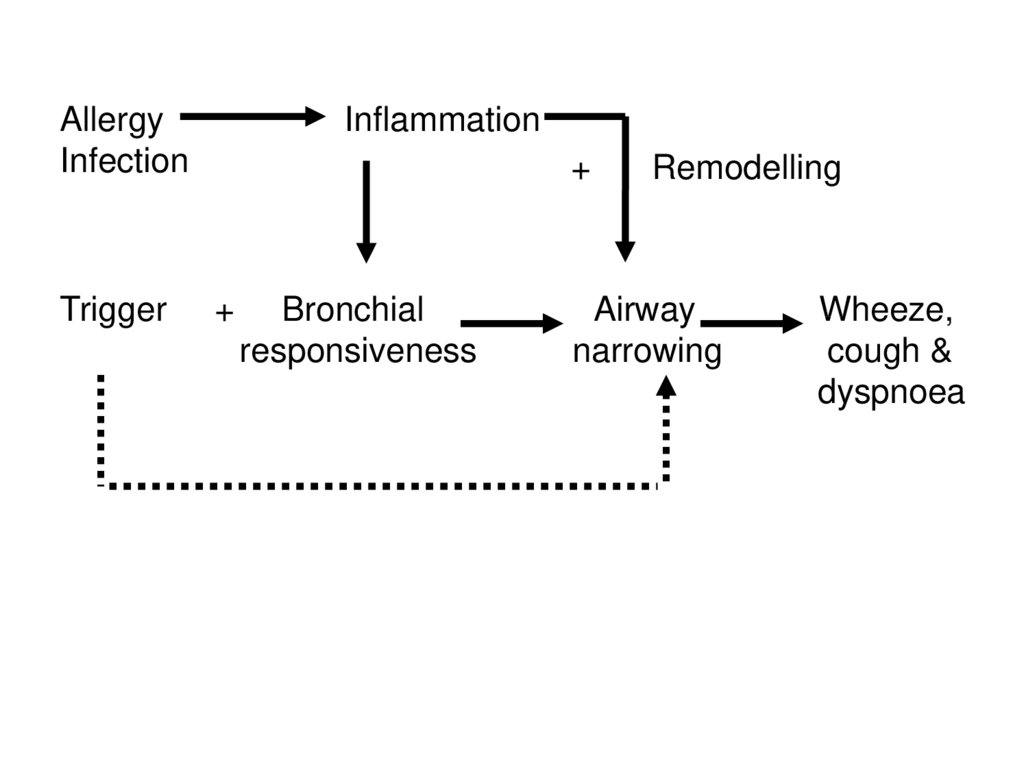
AllergyInfection
Trigger
Inflammation
+
+
Bronchial
responsiveness
Remodelling
Airway
narrowing
Wheeze,
cough &
dyspnoea
22.
23.
24.
25.
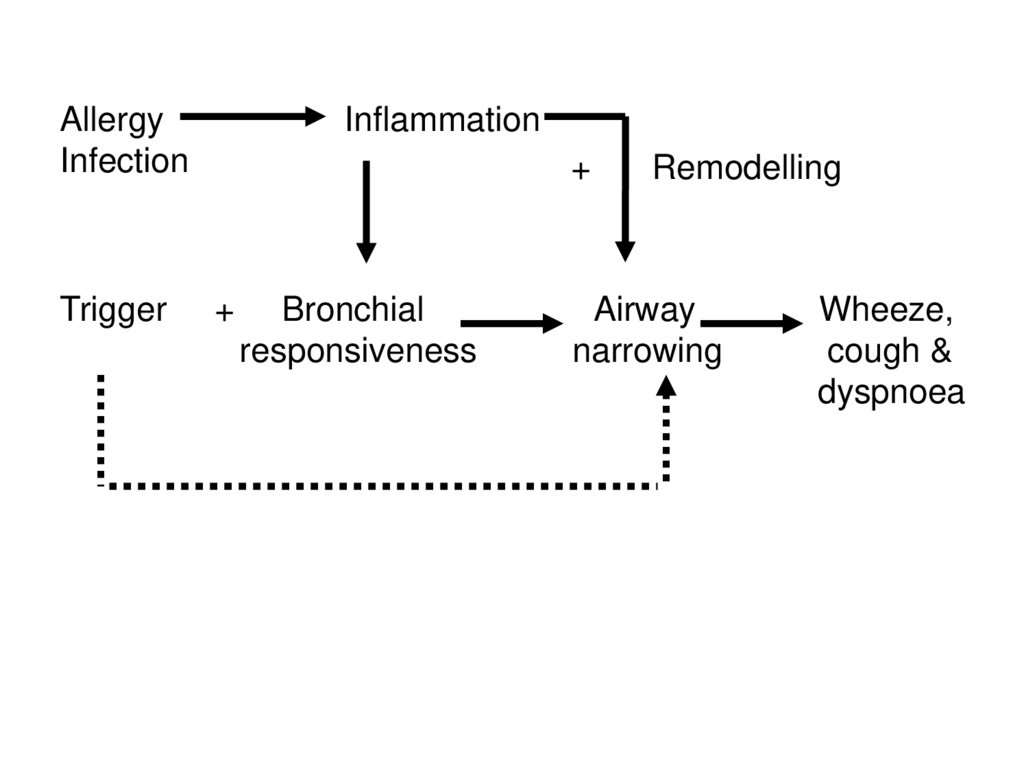
AllergyInfection
Trigger
Inflammation
+
+
Bronchial
responsiveness
Remodelling
Airway
narrowing
Wheeze,
cough &
dyspnoea
26.
27.
28.
29.
AllergyInfection
Trigger
Inflammation
+
+
Bronchial
responsiveness
Remodelling
Airway
narrowing
Wheeze,
cough &
dyspnoea
30.
Triggers• Allergen (pollen, cat…)
• Air pollution (smoke…)
• Infection (URTI)
• Exercise, etc.
31.
32.
Asthma history questionnaire• age of onset of symptoms
• pattern of symptoms
• amount of disturbance to everyday life,
schooling etc.
• definite association with precipitating factors
- allergic, infective, emotional, exercise,
environmental
• family background and other illnesses
• previous treatment
- appropriateness and technique
- response
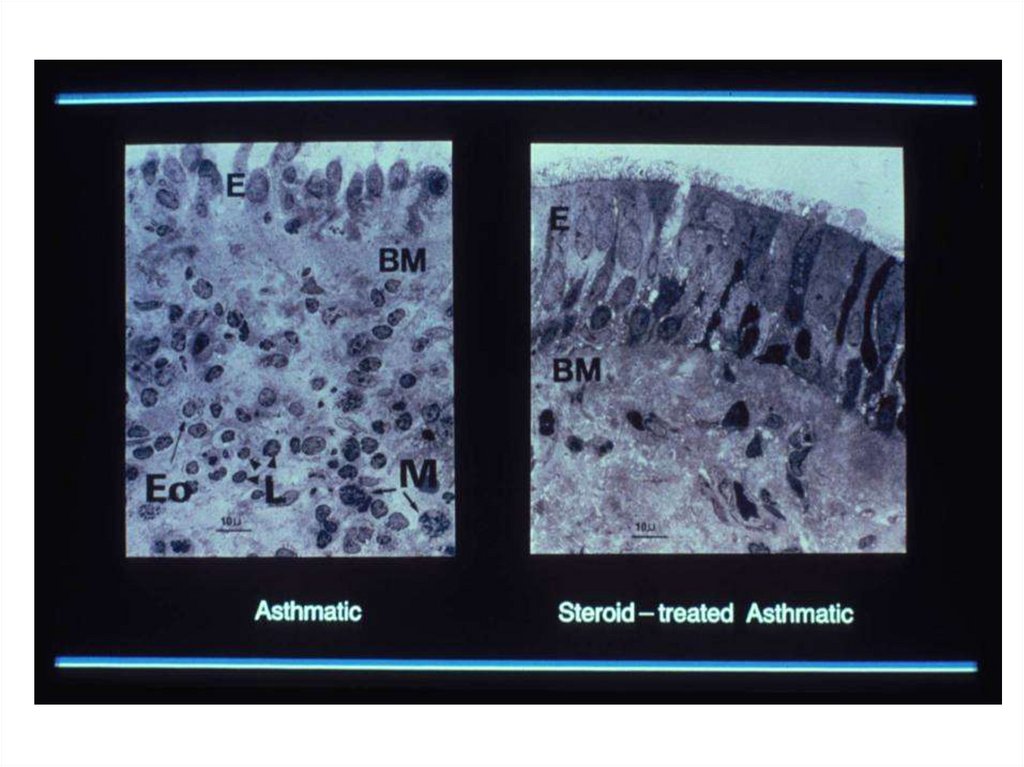
33.
34.
35.
36.
37.
Chronic Wheeze: Non-AsthmaticCystic fibrosis (host-defence)
Bronchiectasis
Foreign body aspiration
Congenital airway disease
Recurrent aspiration syndrome
other!!
38.
The British Thoracic SocietyScottish Intercollegiate Guidelines Network
British Guideline on the
Management of Asthma
A national clinical guideline
Thorax 2003; 58 (Suppl I): i1-i92
39.
40.
Asthma controlAsthma control means:
• minimal symptoms during day and night
• minimal need for reliever medication
• no exacerbations
• no limitation of physical activity
• normal lung function (FEV1 and/or PEF >80% predicted or best)
Pharmacological management. Thorax 2003; 58 (Suppl I): i1-i92
41.
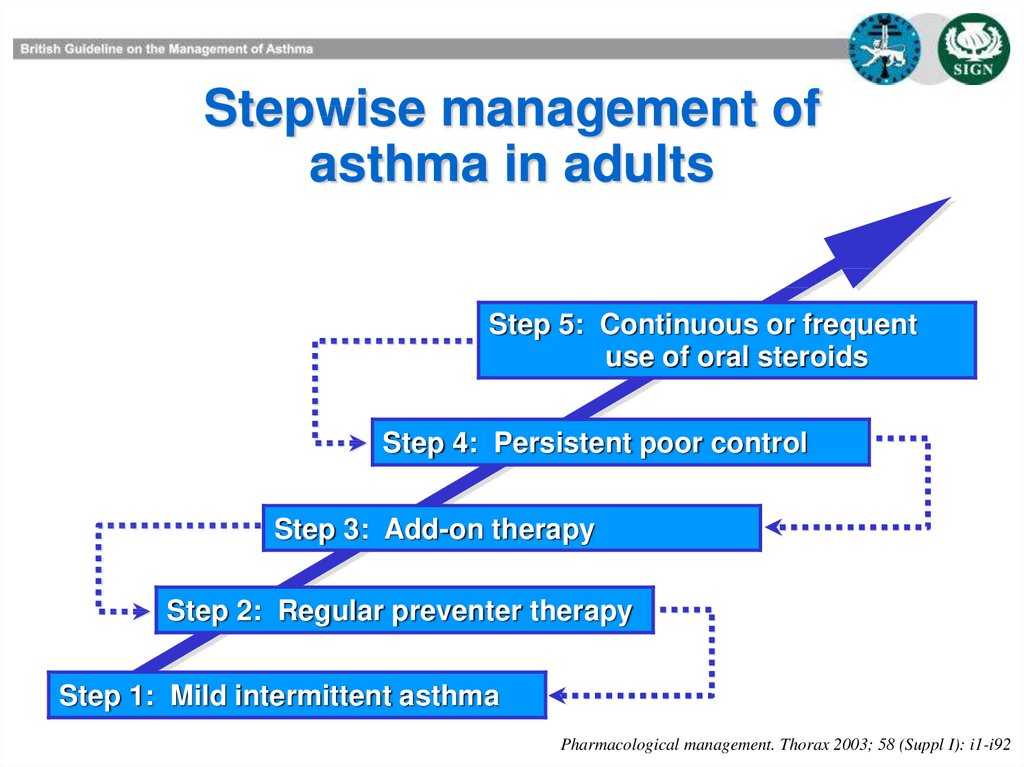
Stepwise management ofasthma in adults
Step 5: Continuous or frequent
use of oral steroids
Step 4: Persistent poor control
Step 3: Add-on therapy
Step 2: Regular preventer therapy
Step 1: Mild intermittent asthma
Pharmacological management. Thorax 2003; 58 (Suppl I): i1-i92
42.
43.
44.
45.
46.
47.
Summary• outline of asthma
• fill in the details
British Guidelines
British Thoracic Society
• pharmacology of drugs
48.
Anyquestions?