










































 medicine
medicineSimilar presentations:










Segmental Stability of The Cervical Spine
1.
Segmental Stability ofThe Cervical Spine
2.
Cervical SpineMuscles
3.
Neck FlexorsSuperficial
• Sternocleidomastoid
• Scalenes
• Supra-hyoid muscles
• Infrahyoid musles
–
–
–
–
Deep
Longus Colli
Longus Capitus
Rectus Capitus
Anterior
Rectus Capitus
Lateralis
4.
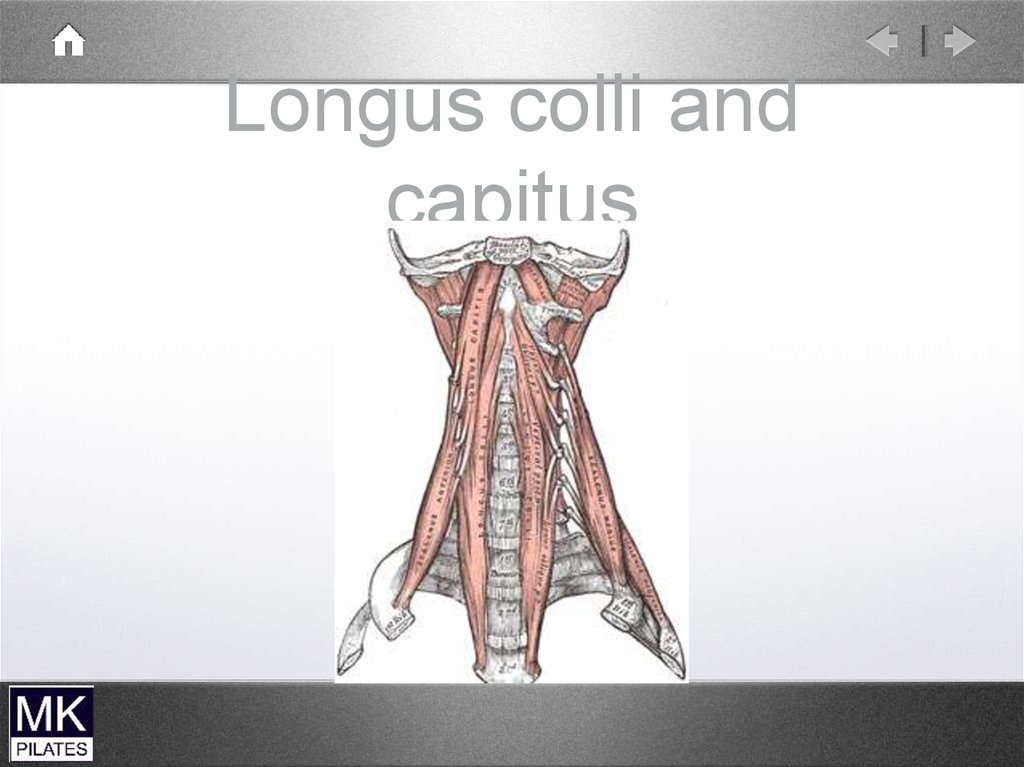
Deep neck flexorsDeep
Attach directly to the vertebrae
Single segments
Close to axis of rotation
Tonic activity
Support the spinal curve
5.
Longus colli andcapitus
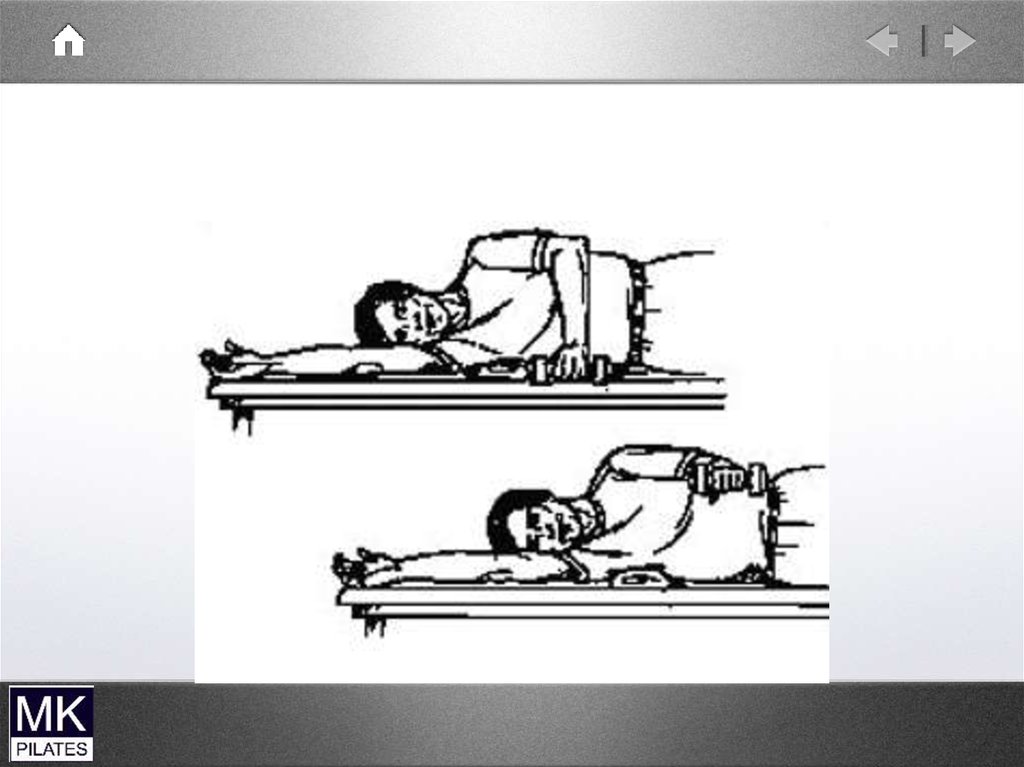
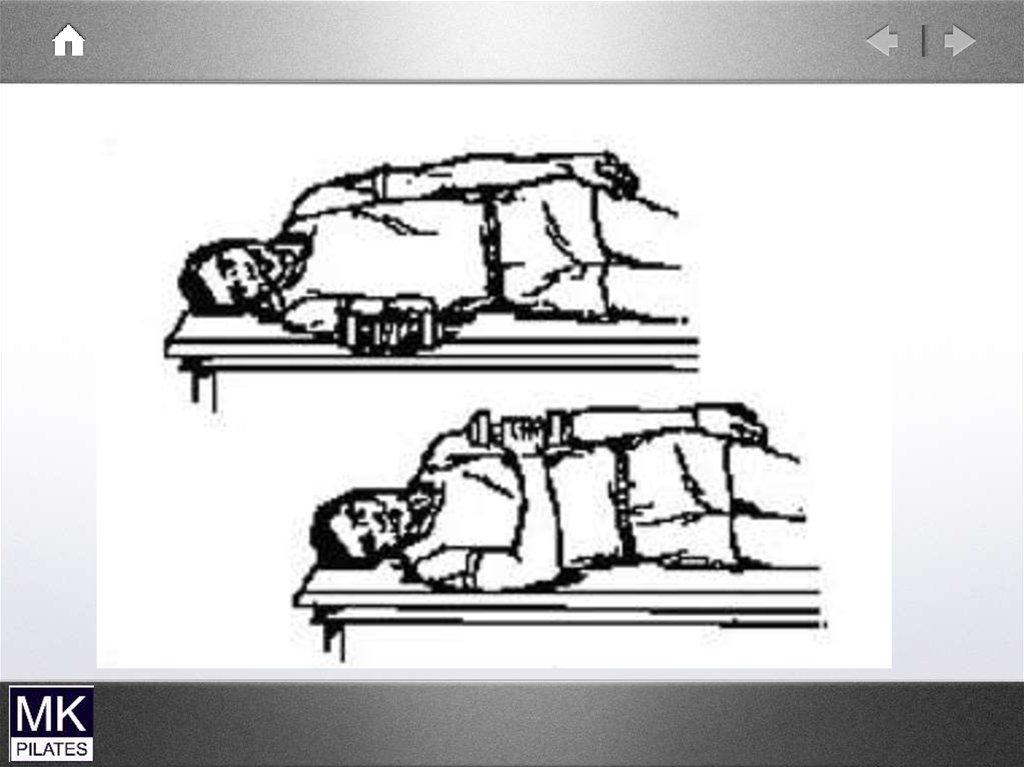
6.
Longus colli andcapitus
QuickTime™ and a
decompressor
are needed to see this picture.
7.
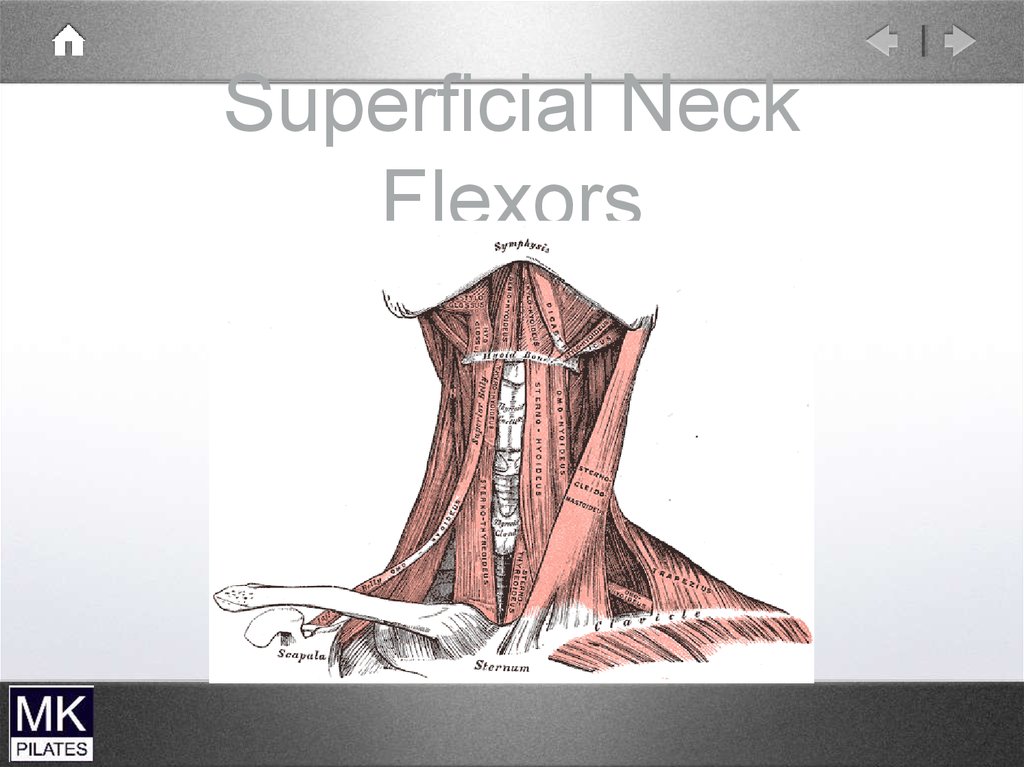
Superficial Neck
Flexors
Predominantly Mobilisers
Also lateral flexion and rotation
Hyoid muscles also control hyoid
movement (for speech and swallowing)
therefore only secondary cervical spine
mobilisers
8.
Superficial NeckFlexors
9.
ScalenesQuickTime™ and a
decompressor
are needed to see this picture.
10.
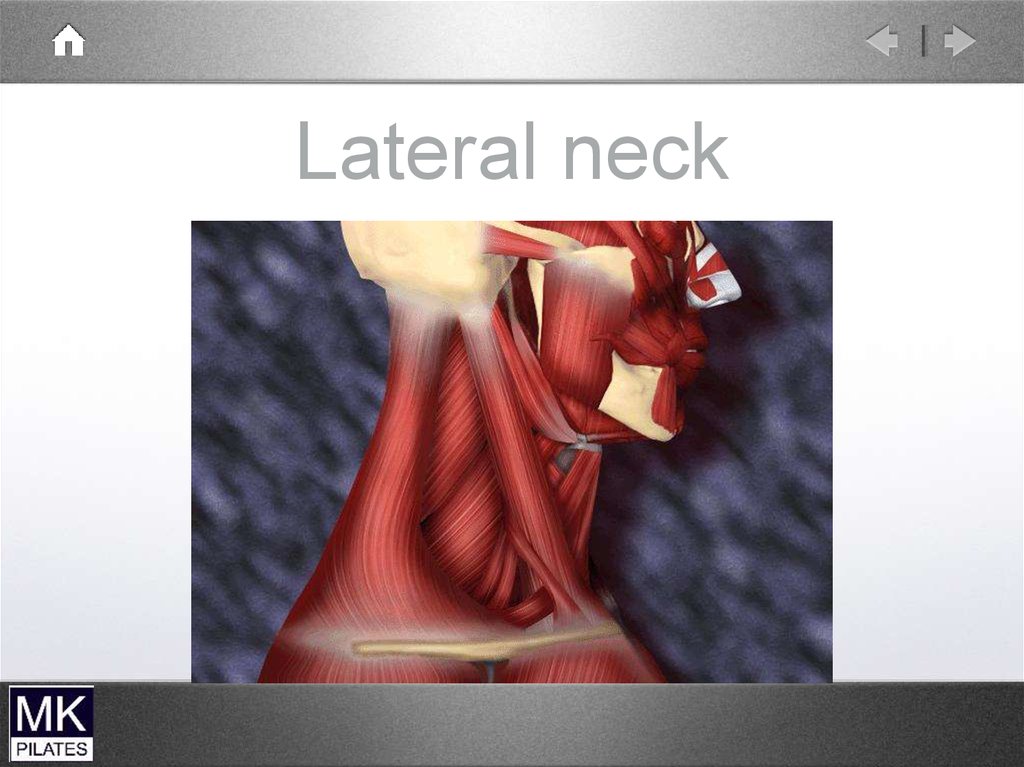
Lateral neck11.
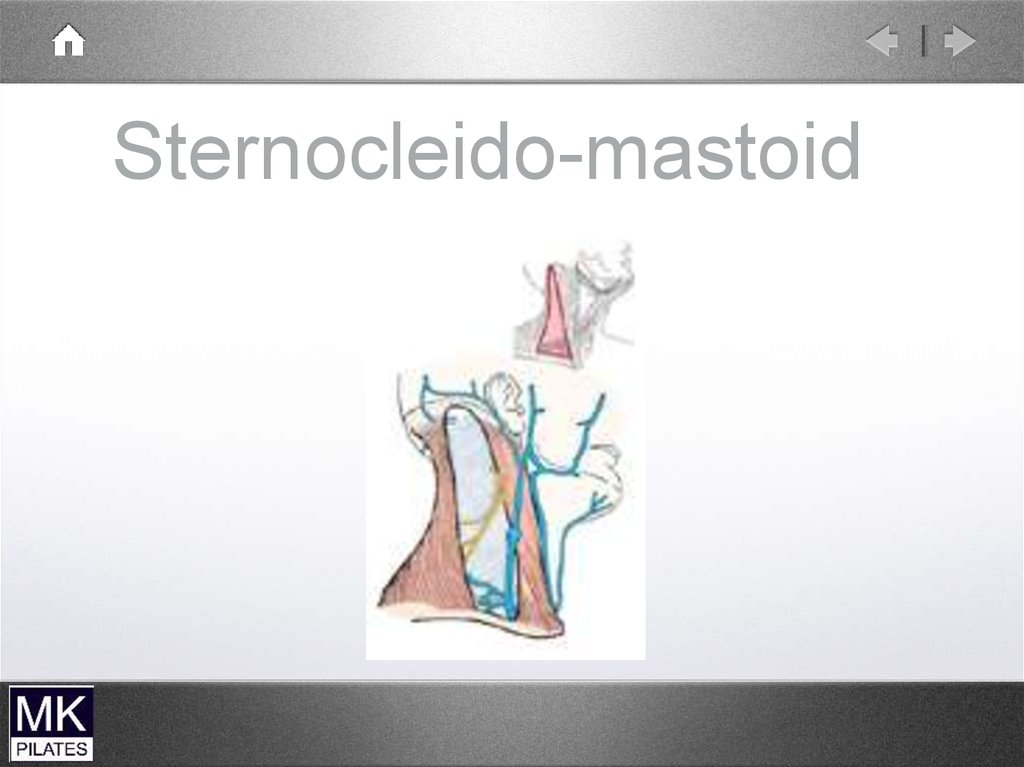
Sternocleido-mastoid12.
Sternocleido-mastoidQuickTime™ and a
decompressor
are needed to see this picture.
13.
14.
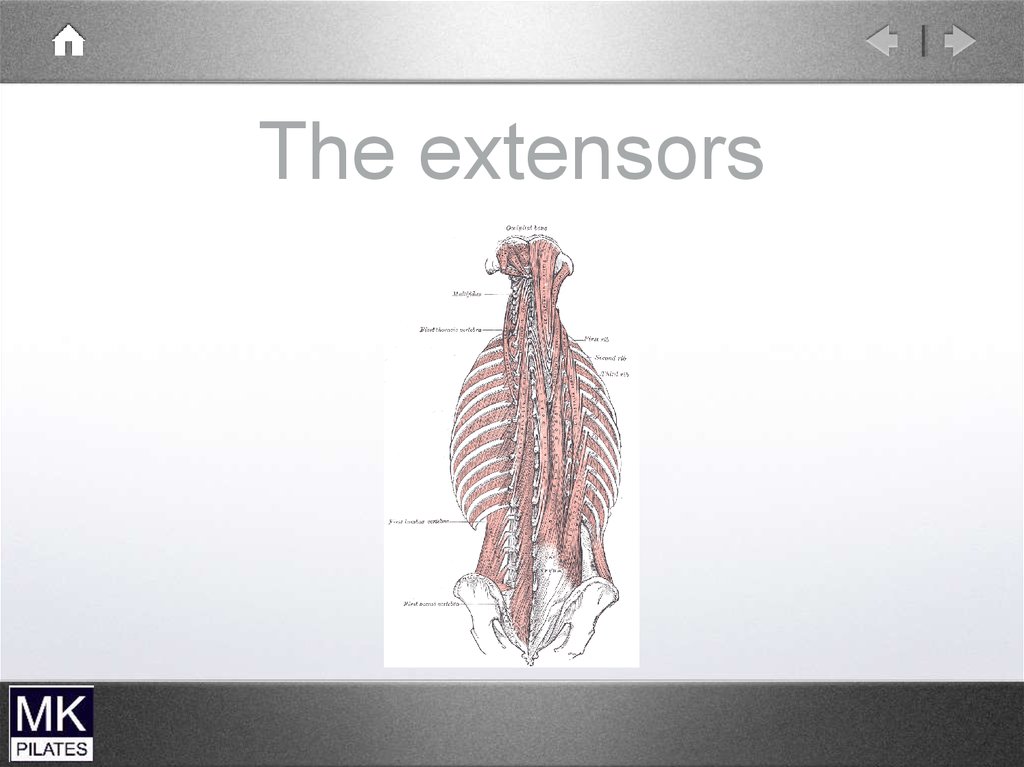
NeckExtensors
Deep Extensors
Spinales
Semispinalis
Rotators
Intertransversarii
Interspinales
• Suboccipital
extensors
Multifidus
Superficial Extensors
• Upper trapezius
• Levator scapulae
• Splenius
• Longisimus
15.
The extensors16.
Sub-OccipitalExtensors
(• upper
cervical
spine)
Rectus Capitus
posterior major
and minor
Occiput to C1 and C2
Obliquus capitus superior and inferior
Occiput to C1 and C1 to C2
Head on Neck Stabilisers
17.
Upper cervicalextensors
• Bilaterally upper cervical extension .
Mainly work to control excessive upper
cervical flexion.
Control excessive movement
• Eccentric activity
• Significant proprioceptive function
18.
Deep neck extensors( mid to low cervical
spine)
Eccentric action to control movement
Proprioceptive role
19.
Deep neck extensorsSegmental control of extension mid to
lower cervical spine
Limit and control excessive cervical
flexion and shear /translation forces
Unilaterally controls rotation and lateral
flexion
Proprioceptive role
20.
MobilityMuscles
• Splenius mastoid to C4-T3
Slenius cervicus TP C1-2 to Sp T4-6
Longissimus capitus Mastoid to TPC5-6
Iliocostalis cervicus TP C4-6 to ribs 3-6
Levator scapulae TP C1-4 to
superiormedial border of scapula
Lets just call them superficial extensors!!!
21.
Superficial ExtensorsUpper and lower cervical extension
Not segmental
Ipsilateral rotation and lateral flexion
without segmental control
22.
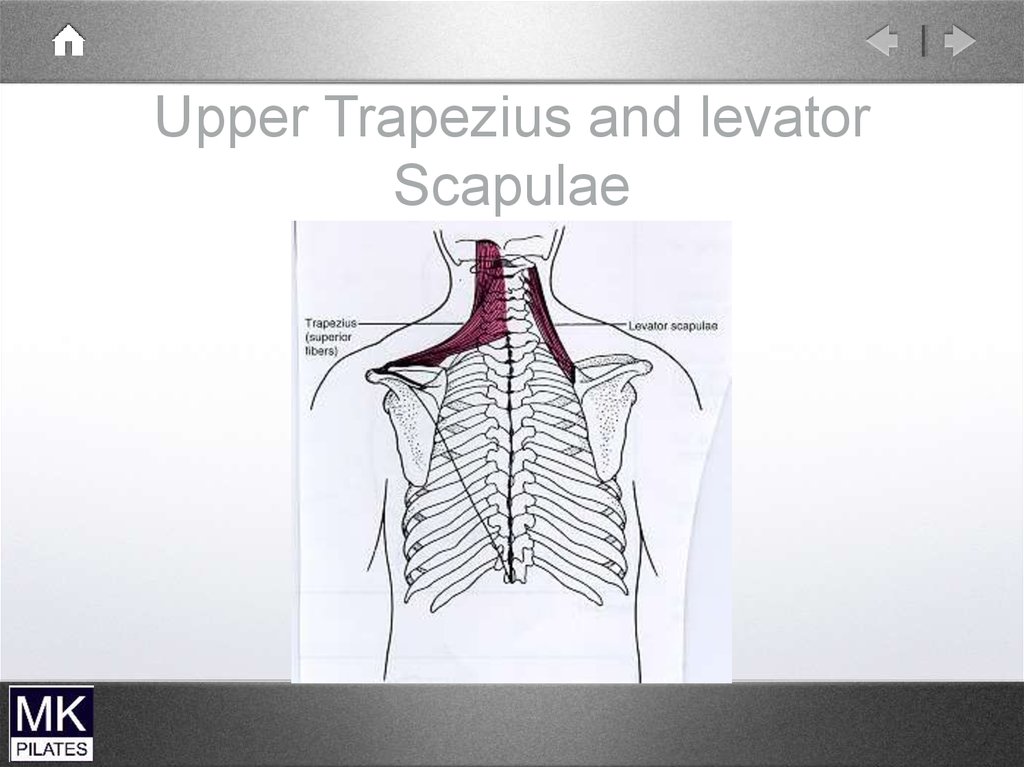
Upper Trapezius and levatorScapulae
23.
TrapeziusQuickTime™ and a
decompressor
are needed to see this picture.
24.
Levator Scapulae andUpper
Trapezius
• Mainly
mobility of
scapula
Can also produce Neck extension and
lateral flexion but not their prime role
No segmental control
problematic if become short and stiff
25.
Ideal Neck PosturePlane of neck and jaw should
be different not one continuous
line
Plumb line drawn down centre
of neck should be neutral or
within 10 degrees of forward
inclination
Plumb line from ear lobe
should fall just in front of
clavicle
Look for creases and
assymmetries
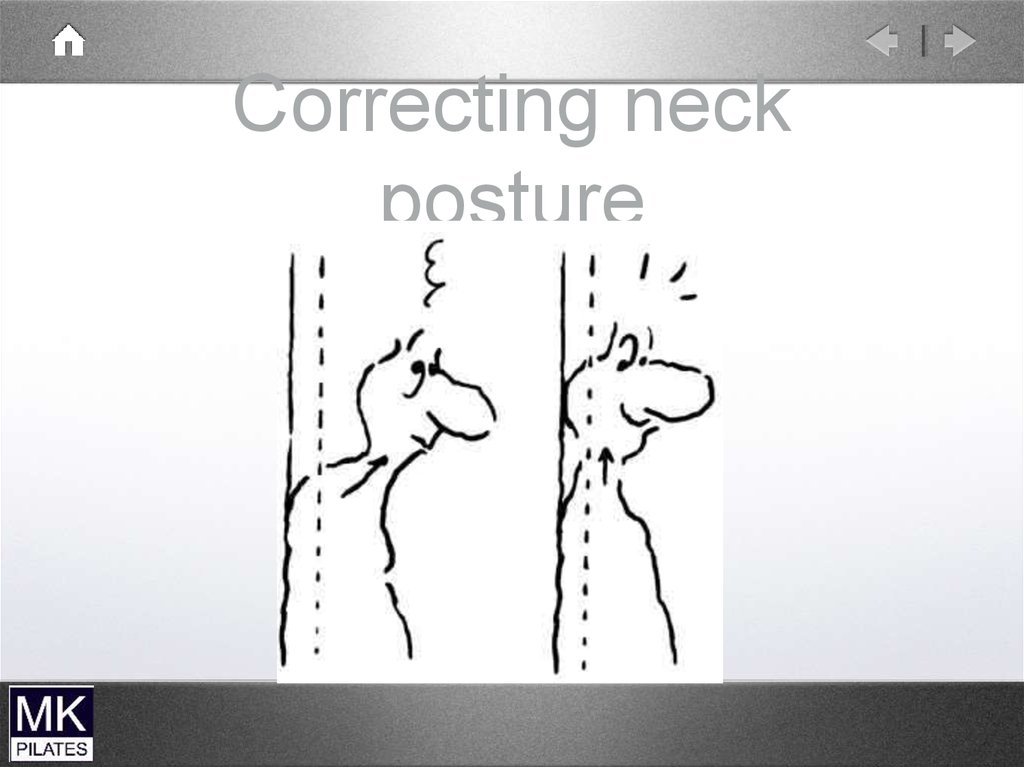
26.
Common Posturetypes
Chin Poke ( upper cervical spine)
Forward head ( lower cervical spine)
Forward head with chin poke
Can also get a hinge or mid cervical
collapse
27.
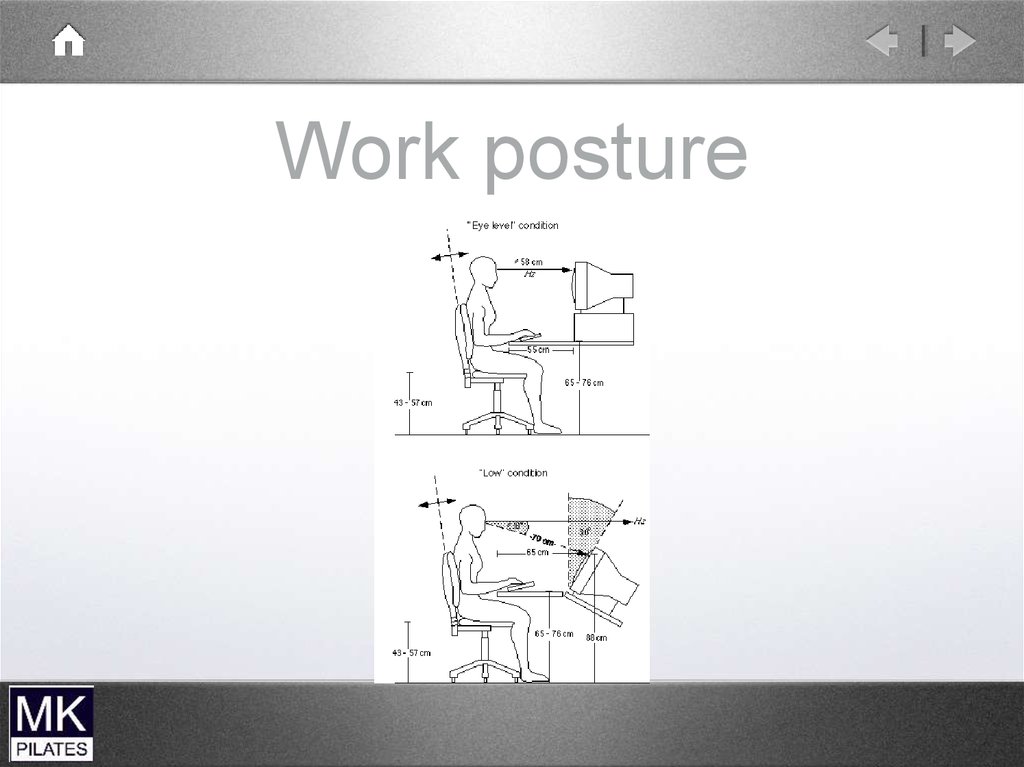
Work posture28.
Chin Pokeupper cervical spine
Short/overactive muscles
-Sterno cleido mastoid-suboccipital
extensors
Weak /lengthened muscles
-deep neck flexors
29.
Chin Poke30.
Forward Head
lower cervical spine
Short overactive muscles
-scalenes
Weak/lengthened muscles
-Deep neck flexors
- Deep neck extensors
31.
32.
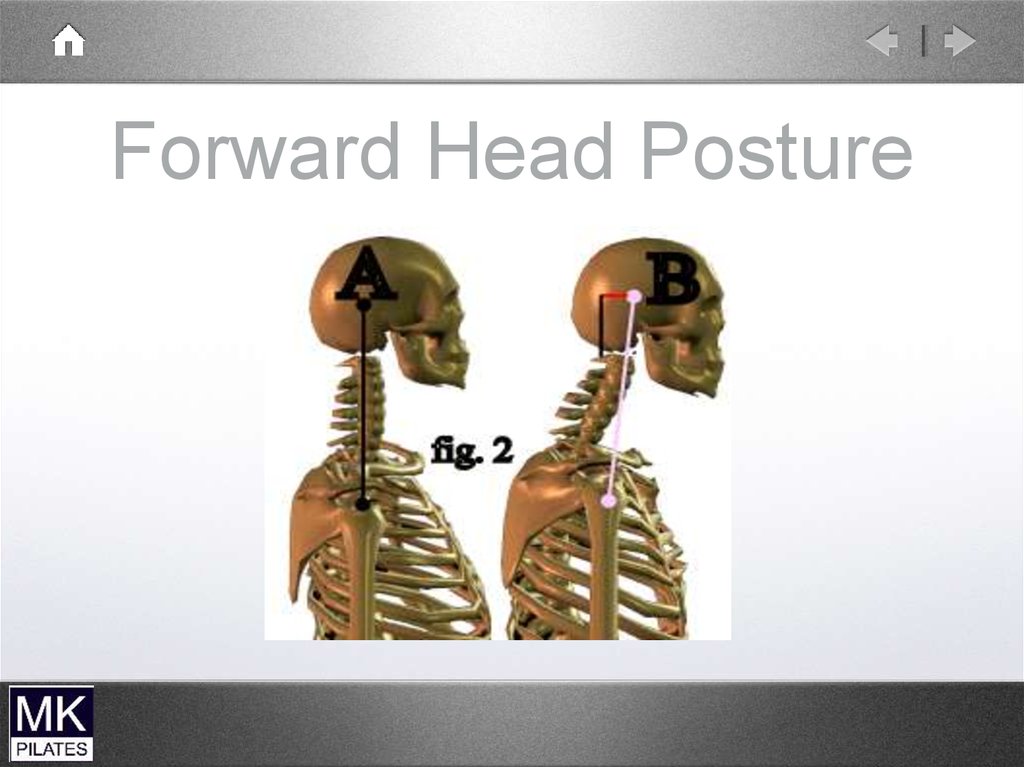
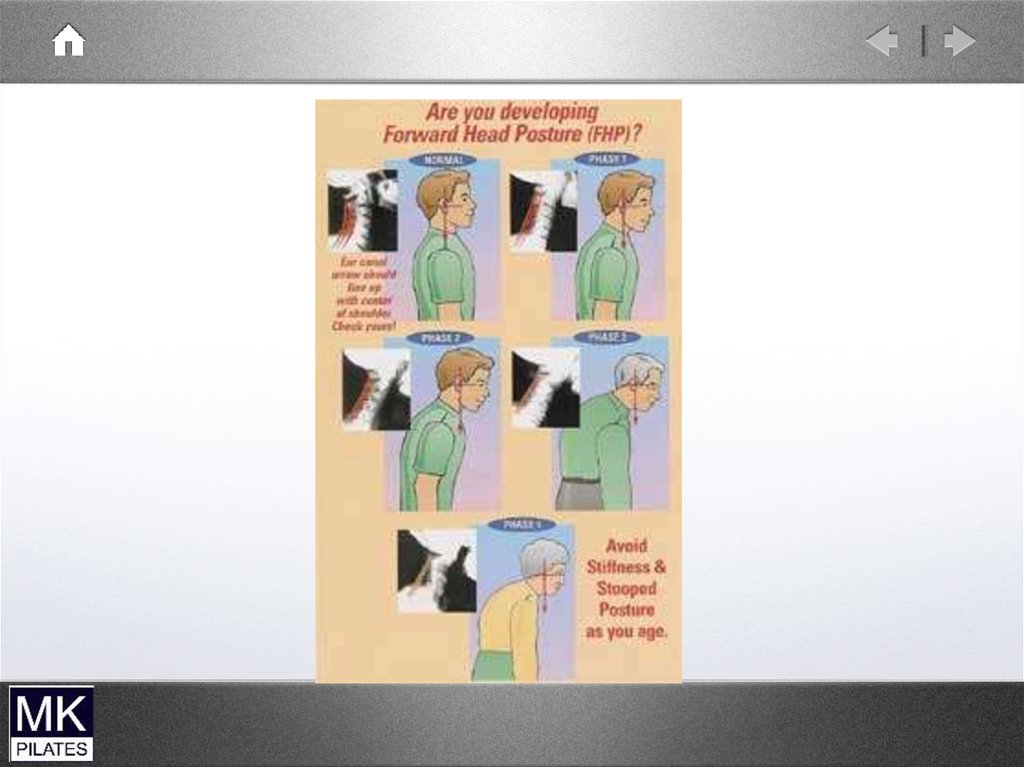
Forward Head Posture33.
34.
35.
Make best use of office space36.
Occupational therapy for patients can be usedcreatively to ease the A&C shortages
37.
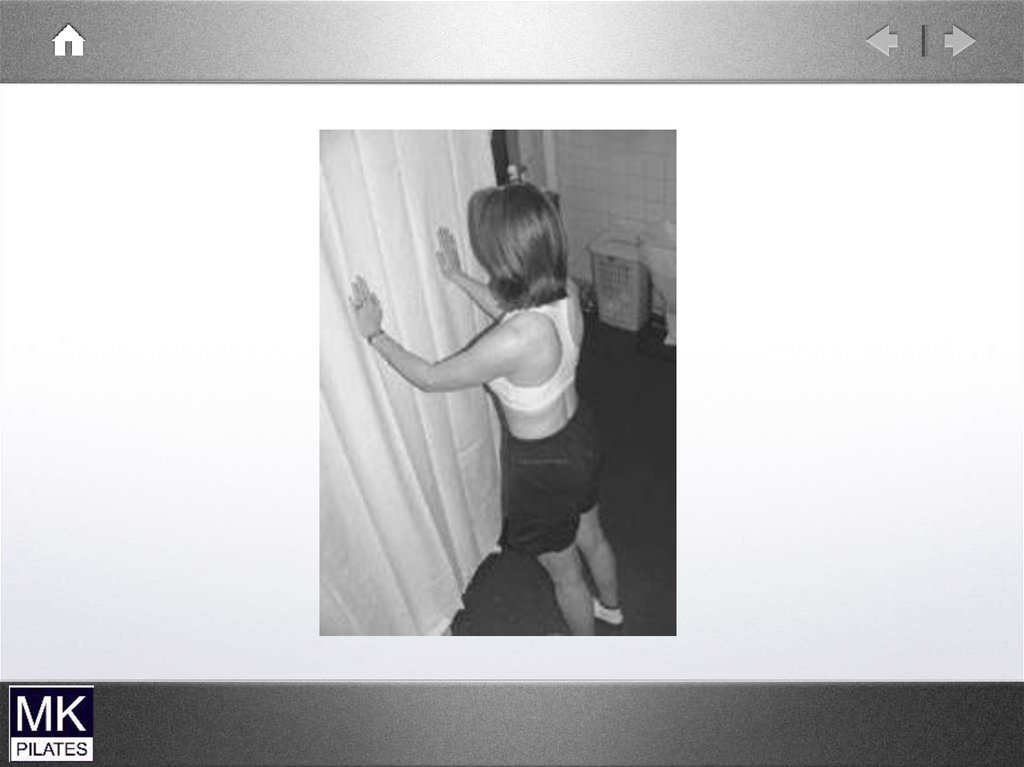
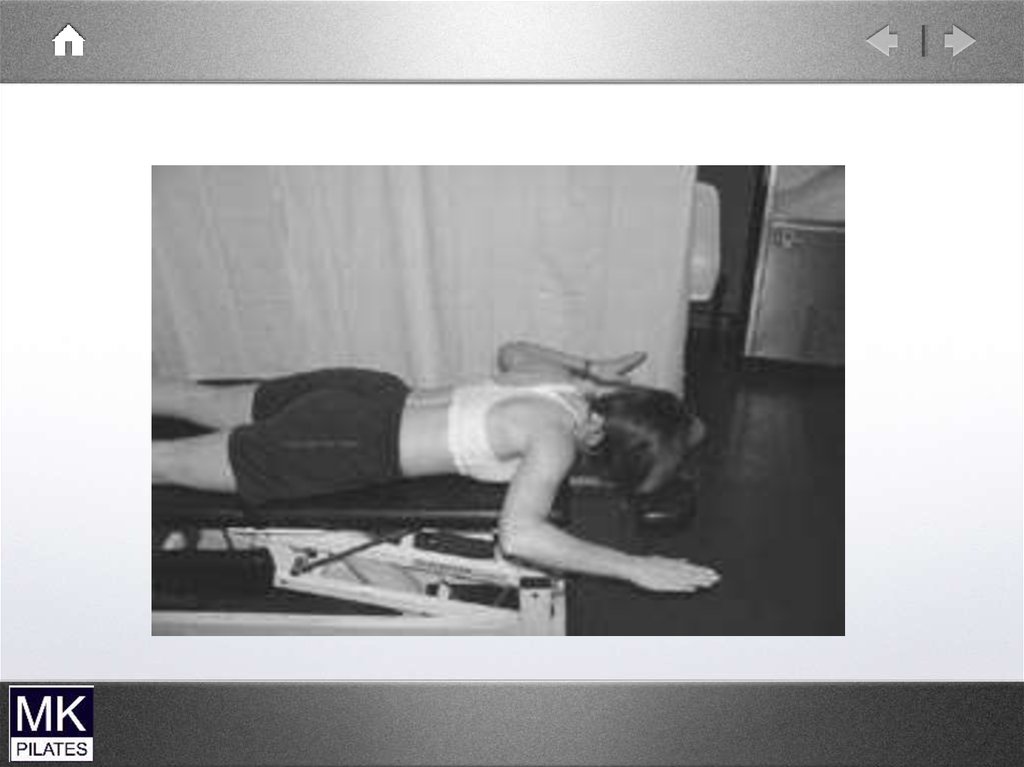
Correcting neckposture
38.
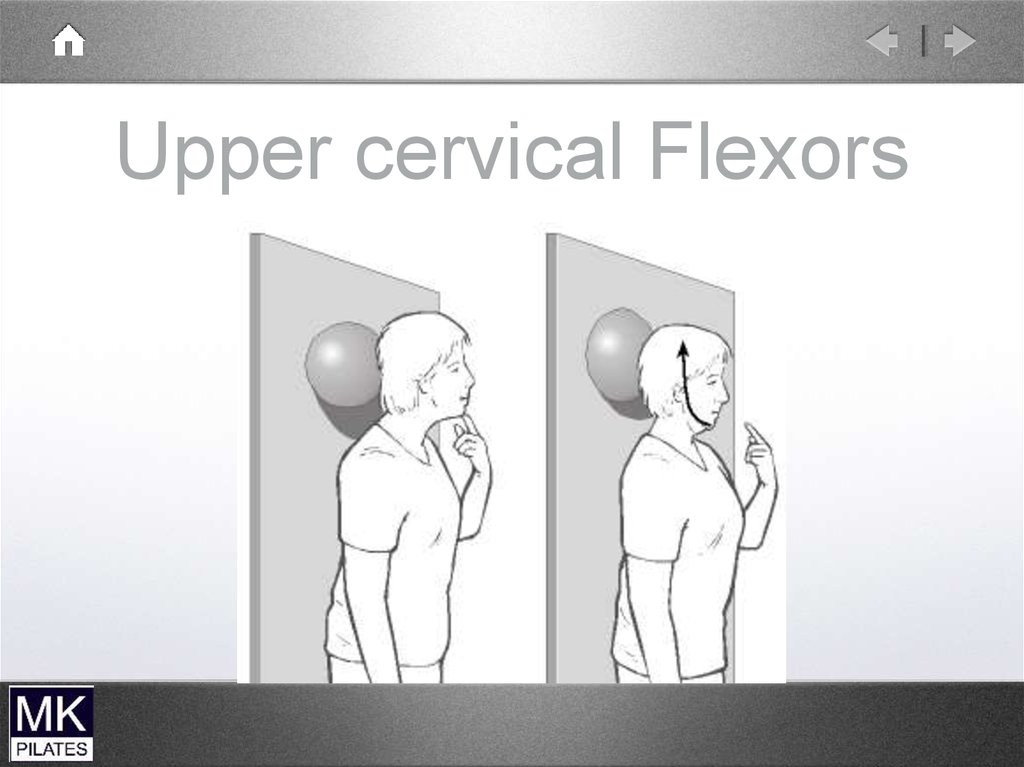
Upper cervical Flexors39.
40.
Cervical flexion testsupineLead with chin…..dominant sternocleidomastoid
Over flexion upper cervical spine
…overactive scalenes
Clenching of teeth…hyoid muscles
41.
42.
The Shoulder Complex43.
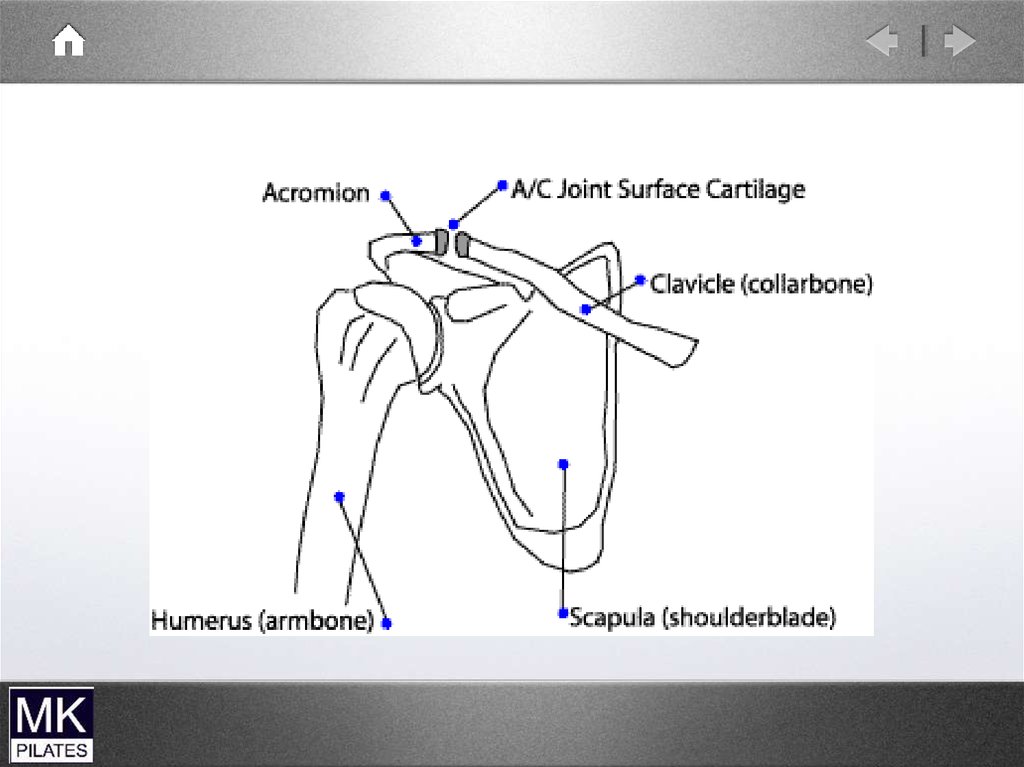
4 joints• The glenohumeral joint
• The acromioclavicular joint
• The Sternoclavicular joint
• The Scapulothoracic articulation
44.
45.
46.
Typical synovial joint47.
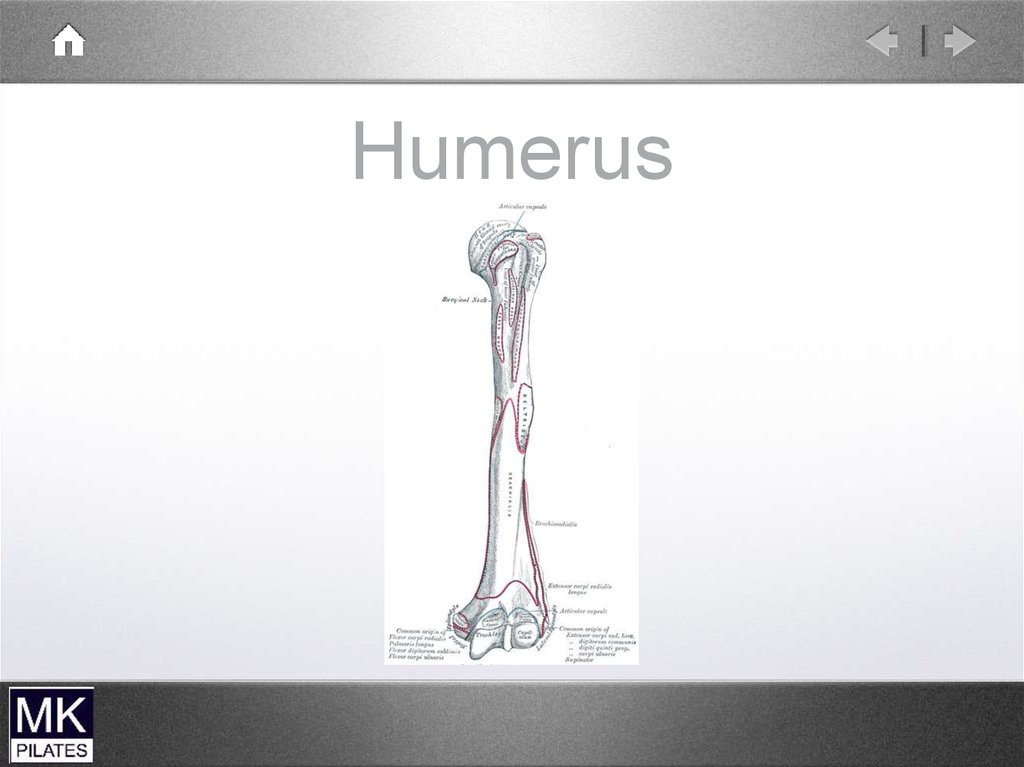
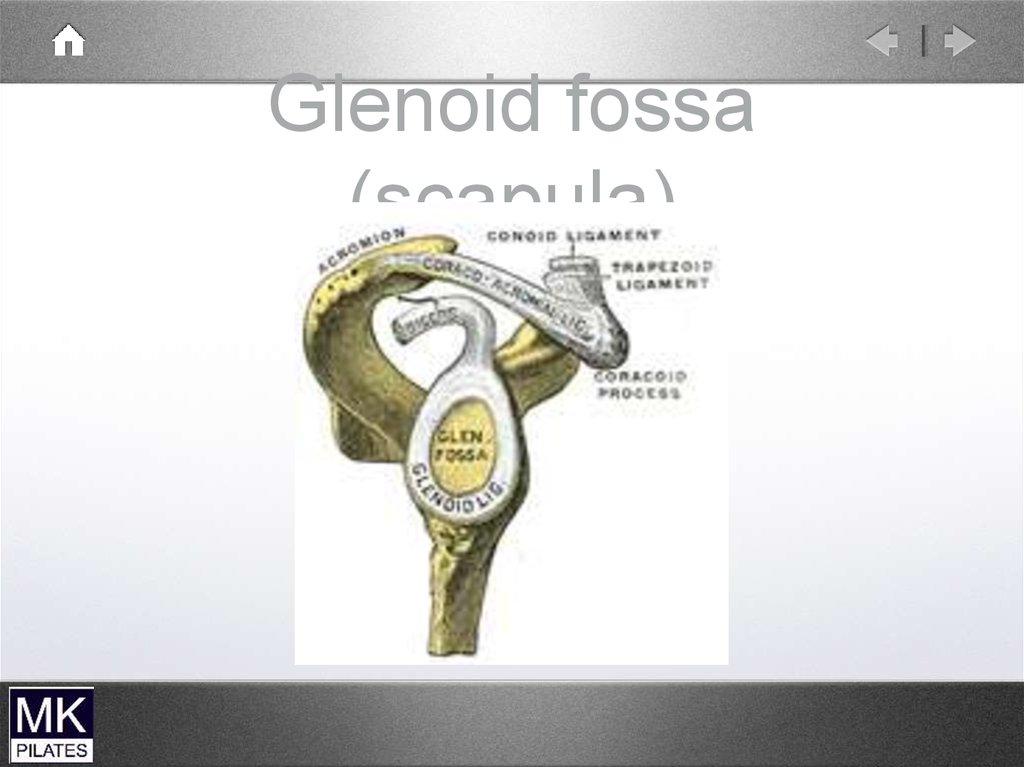
The glenohumeral jointBall and socket synovial joint
Large humeral head
Small glenoid fossa
Stability sacrificed for mobility
48.
Humerus49.
Glenoid fossa(scapula)
50.
The shoulder51.
Gleno-humeral movement• Flexion
• Extension
• Internal (medial) Rotation
• External (lateral) Rotation
• Abduction
• Adduction
52.
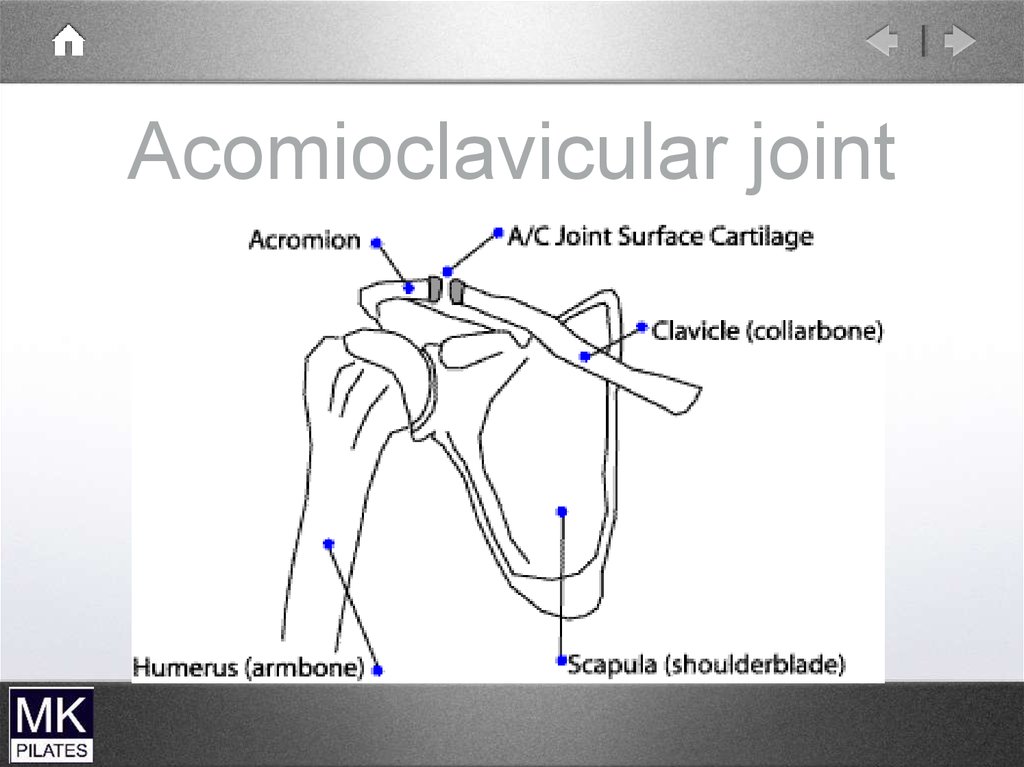
The Acromioclavicular jointSmall plane joint
The lateral end of the clavicle and the
acromion process of the scapula
Joins the scapula to the clavicle
Small gliding movements through
shoulder elevation
Rotation of scapular around clavicle
53.
Acomioclavicular joint54.
Acromioclavicular joint sprainFall onto point of shoulder.
Sprain or disruption of the acromioclavicular ligaments
Grade 1 to 3
Step deformity with grade 3
55.
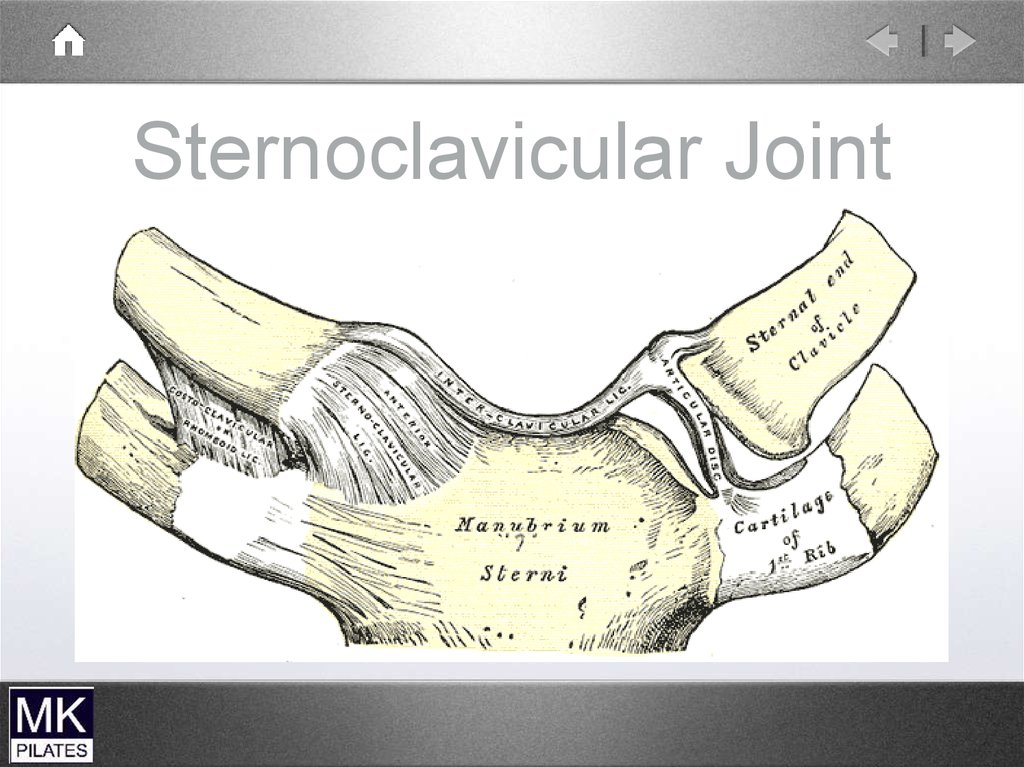
The Sternoclavicular joint• Small fibrous plane joint
• Between the medial end of the clavicle
and the sternum
This attaches the shoulder complex to
the trunk
Gliding Movements and rotation of the
clavicle on the sternum
Allows end range elevation
56.
Sternoclavicular Joint57.
The Scapulothoracic articulationNot a true synovial joint
Allows the scapula to glide around the
thoracic wall
Keeps the glenoid in contact with the
humerus
Supported only by muscles
58.
59.
Scapulohumeral
rhythm
During 180 degrees of arm elevation
2:1 ratio of humeral to scapula movement
-120 degrees glenohumeral
- 60 degrees scapulothoracic
Occurs in 3 phases
60.
Phase 1
abduction
- 30 degrees GH
Scapulohumeral
- minimal scapula
movement rhythm
Phase 2 and 3
- 90 degrees of GH
abduction
- 60 degrees of scapula
rotation
Phase 3
the scapula
rotation of the
clavicle
- mainly elevation of
and posterior
61.
62.
63.
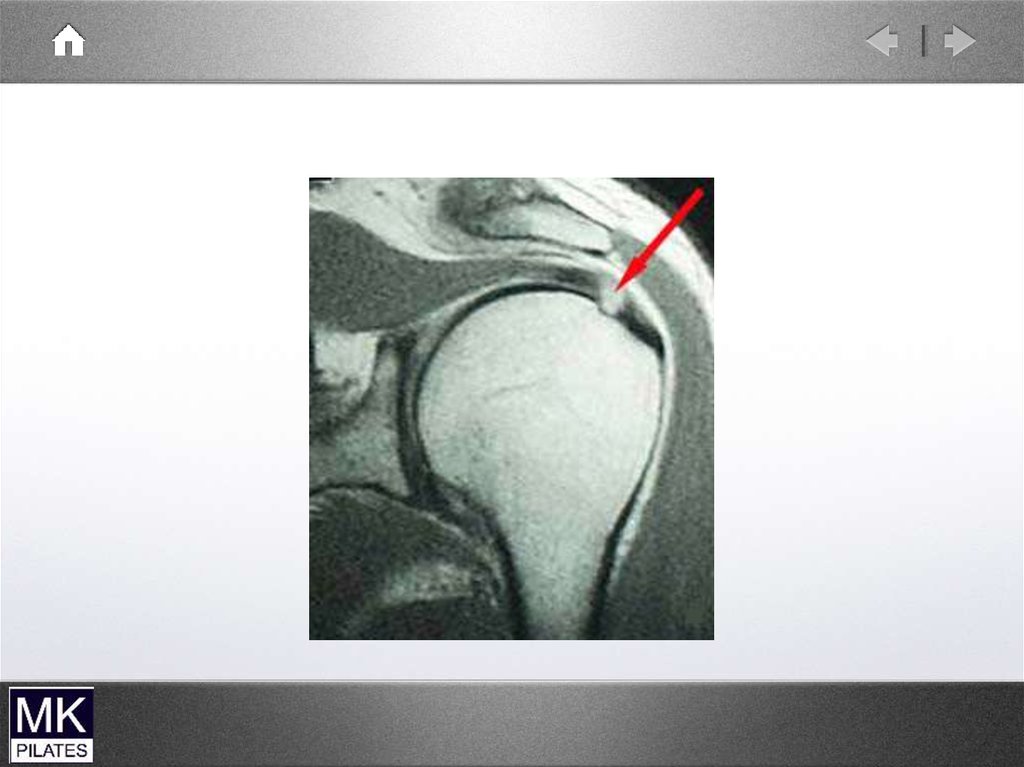
Rotator cuff MRI64.
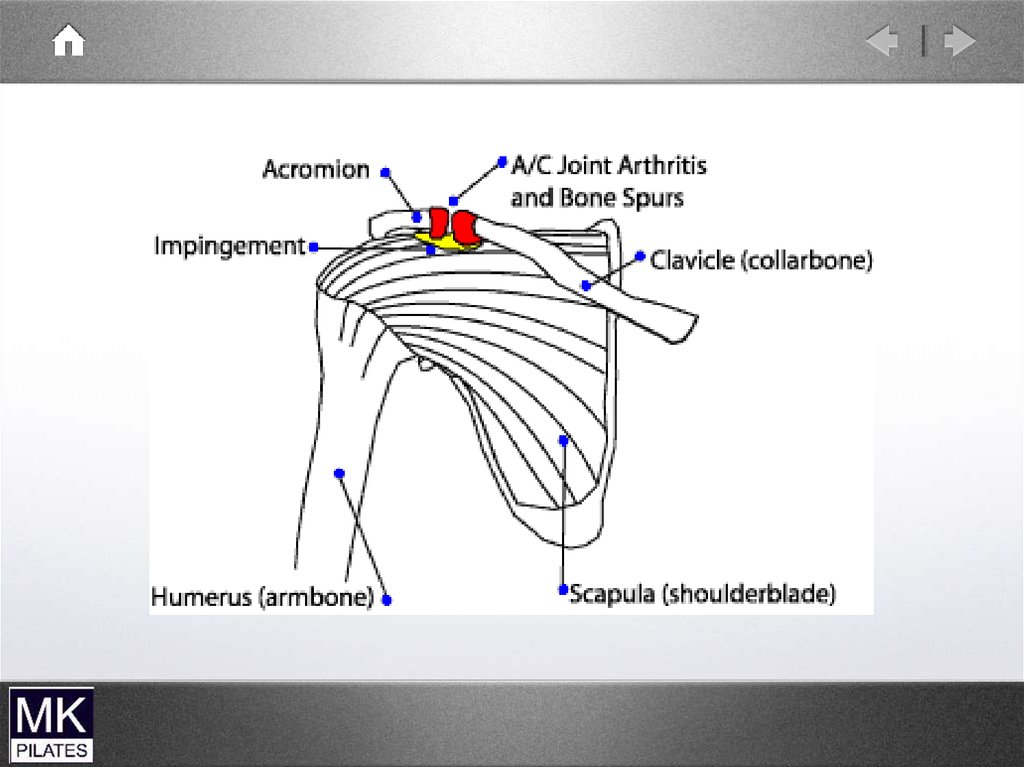
ImpingementSyndrome
Structures between the humerus and the
acromion can become compressed and
pinched during elevation of the arm. The
space is at its narrowest between 70 and
120 degrees.
• Supraspinatus tendon
• Long head of biceps
• Sub-acromial bursa
65.
66.
Biomechanical risk factorsInternal rotation of the shoulder during
elevation
Secondary impingement due to reversed
scapulohumeral rhythm
Short 2 joint muscles
67.
Bone spur68.
X-ray sub-acromialspur
69.
70.
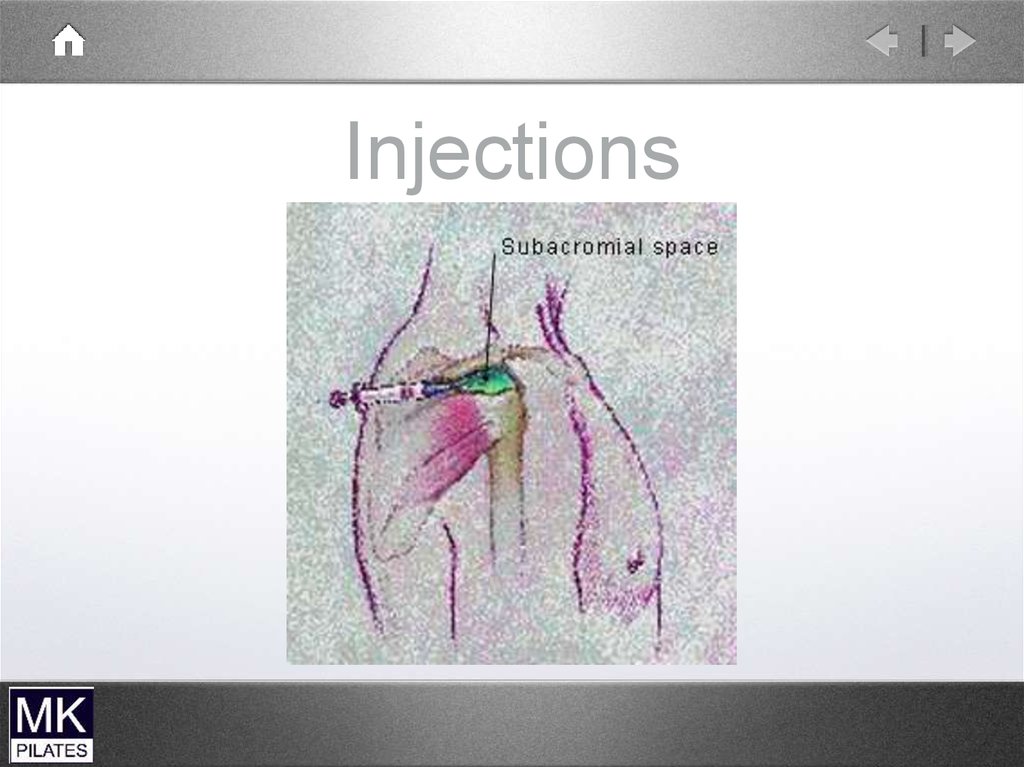
Injections71.
Glenohumeral
Excessive translation
of the large humeral head on
Instability
the relatively small glenoid due to
- Damaged ligaments
- Poor muscle control
Unidirectional (anterior or posterior)
Multidirectional (global)
Instability tests
Need to improve dynamic control
72.
Gleno-humeraldislocation
73.
Frozen ShoulderFrozen shoulder is characterised by
progressive pain and stiffness in the
glenohumeral joint
Can be idiopathic or following injury
3 stages all lasting about 6 months
74.
Frozen Shoulderstages
• Stage 1 Progressive and severe pain. Little
stiffness
• Stage 11 Plateau in pain and increasing
stiffness
• Stage 111 Little pain. Shoulder very stiff
75.
Fractured clavicle76.
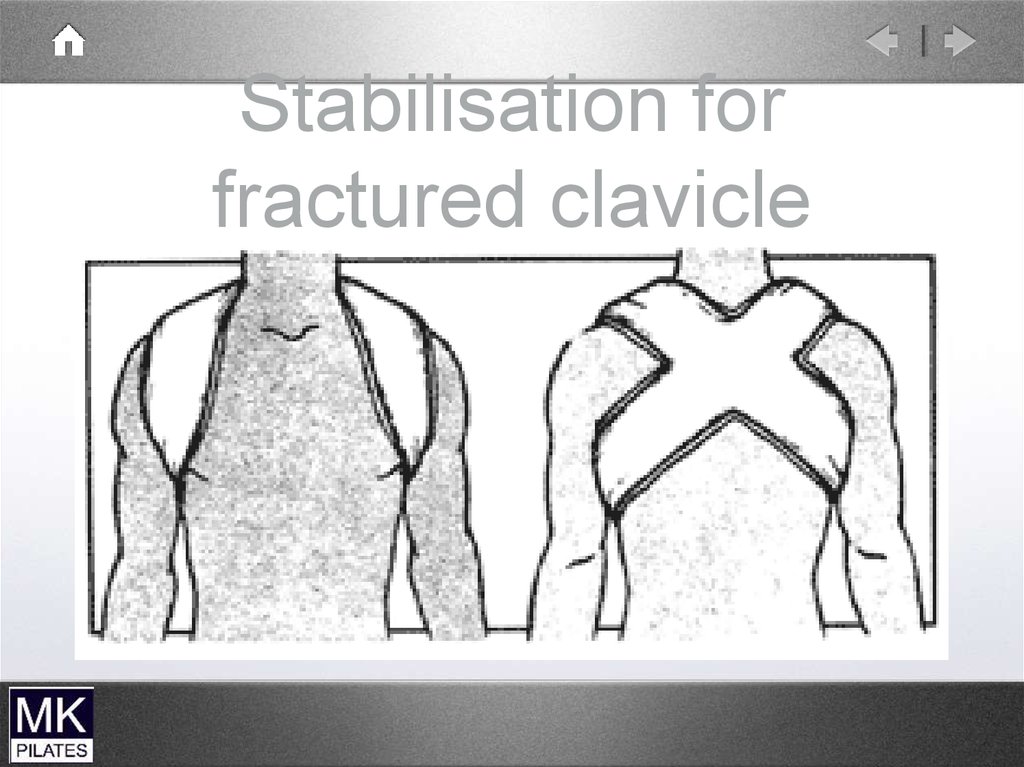
Stabilisation forfractured clavicle
77.
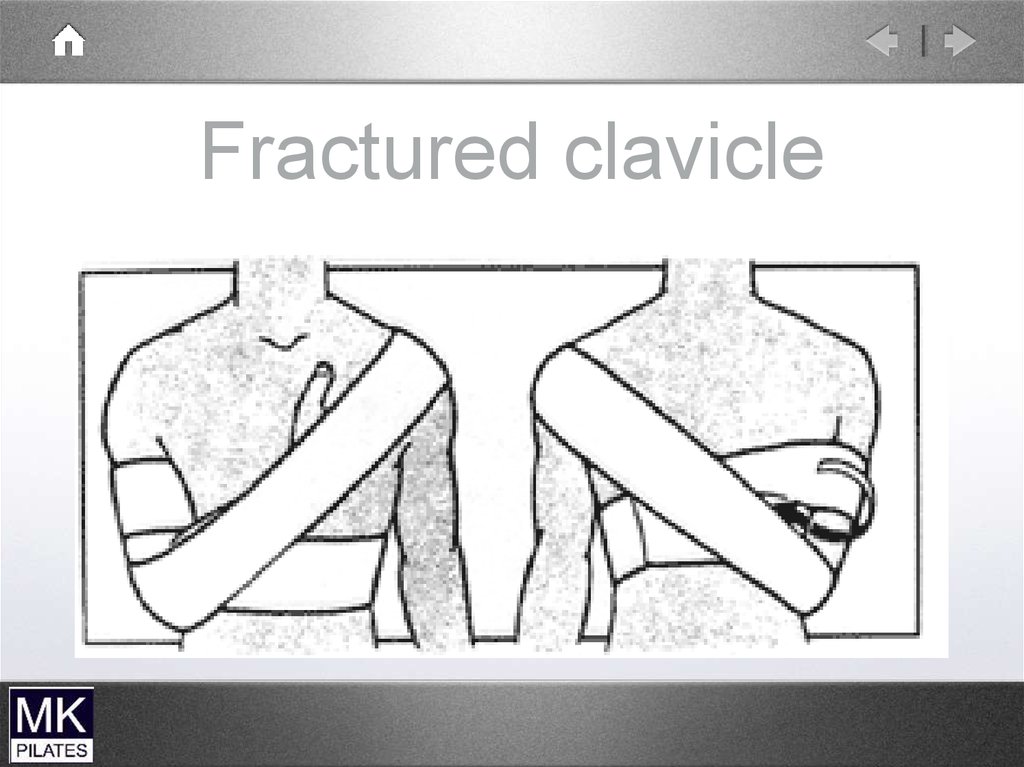
Fractured clavicle78.
79.
Shoulder musclestability
80.
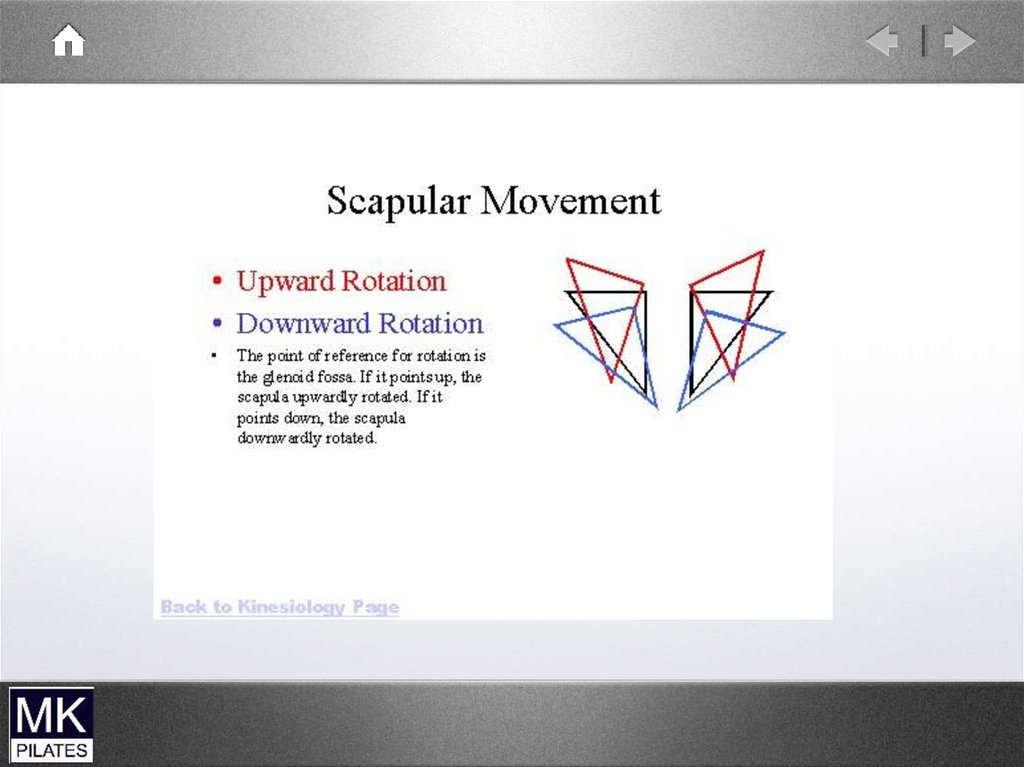
Role of The ScapulaProvides base for muscle attachment
Allows the glenoid to upwardly rotate therefore
allowing a greater range of shoulder movement
Elevation/depression
Abduction/adduction
Upward and downward rotation
81.
Trunk to HumerusLatissimus Dorsi
Pectoralis Major
82.
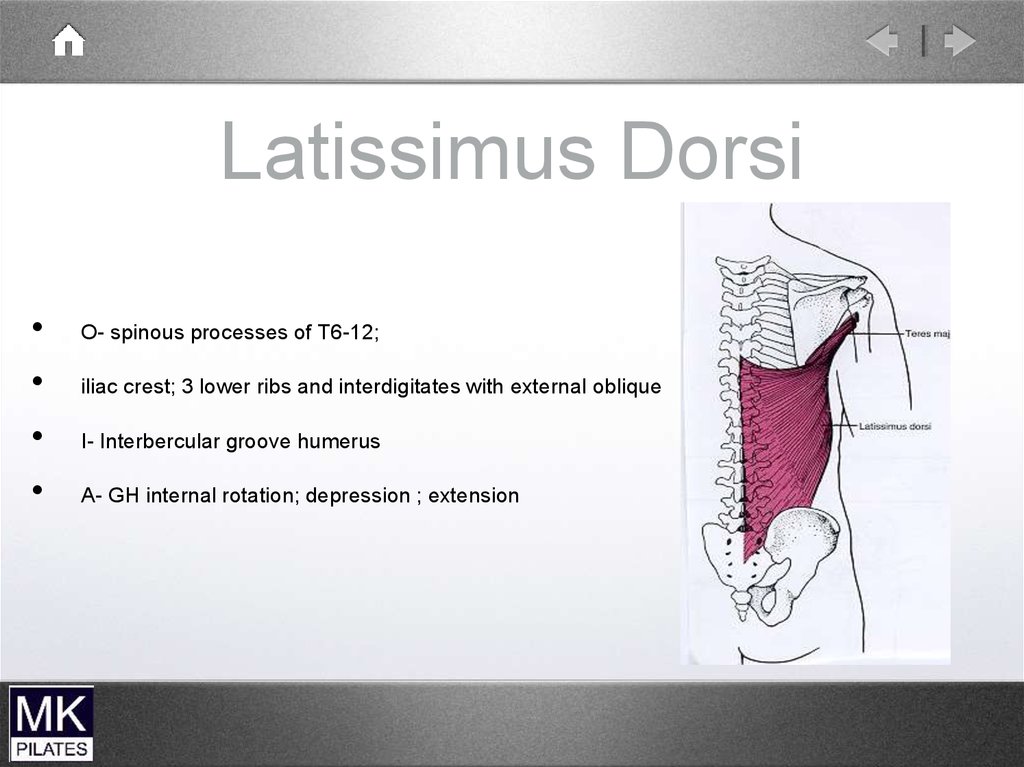
Latissimus DorsiO- spinous processes of T6-12;
iliac crest; 3 lower ribs and interdigitates with external oblique
I- Interbercular groove humerus
A- GH internal rotation; depression ; extension
83.
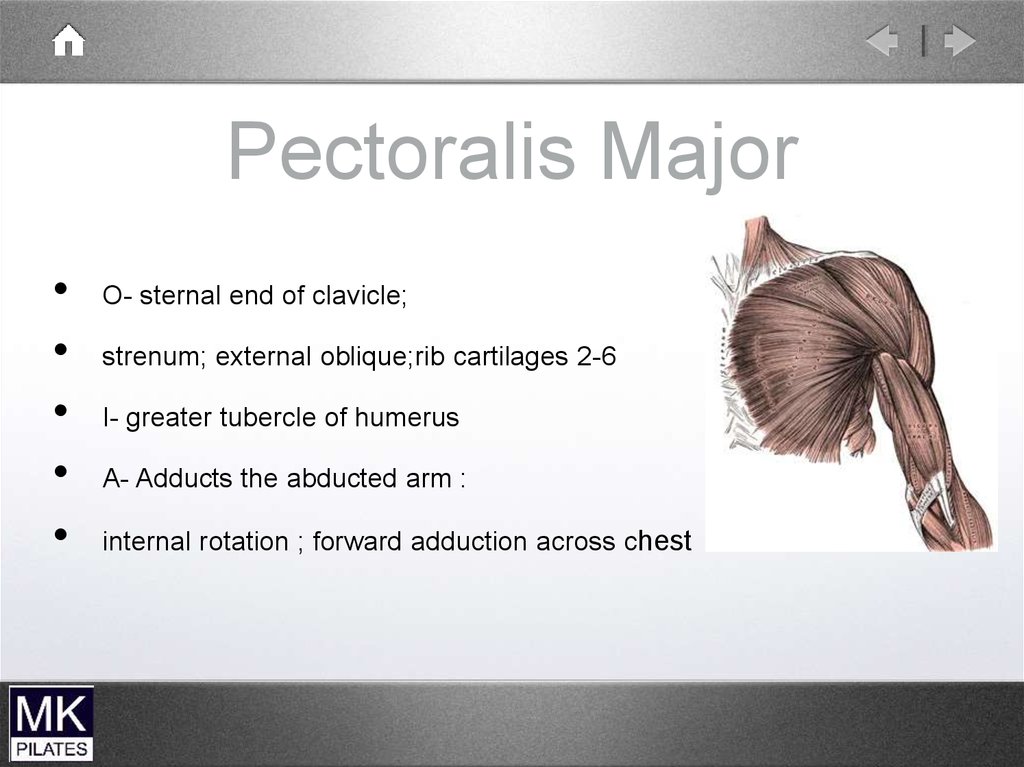
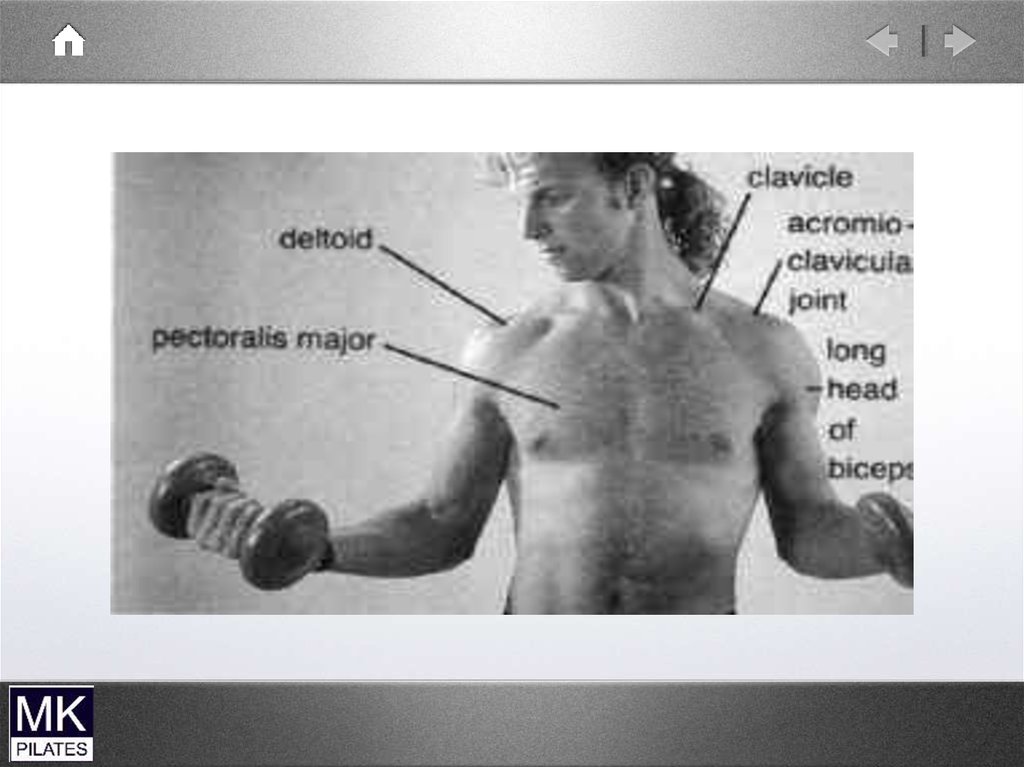
Pectoralis MajorO- sternal end of clavicle;
strenum; external oblique;rib cartilages 2-6
I- greater tubercle of humerus
A- Adducts the abducted arm :
internal rotation ; forward adduction across chest
84.
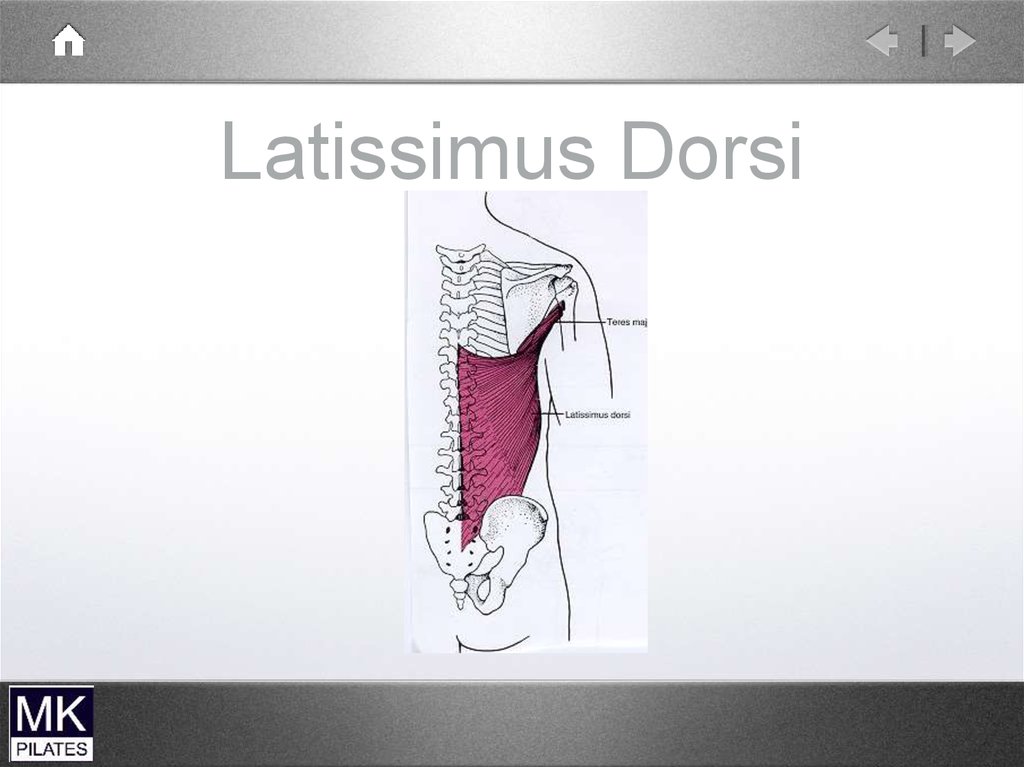
Latissimus Dorsi85.
Trunk to Shoulder ComplexPectoralis Minor
Trapezius
Levator Scapula
Rhomboids
Serratus Anterior
86.
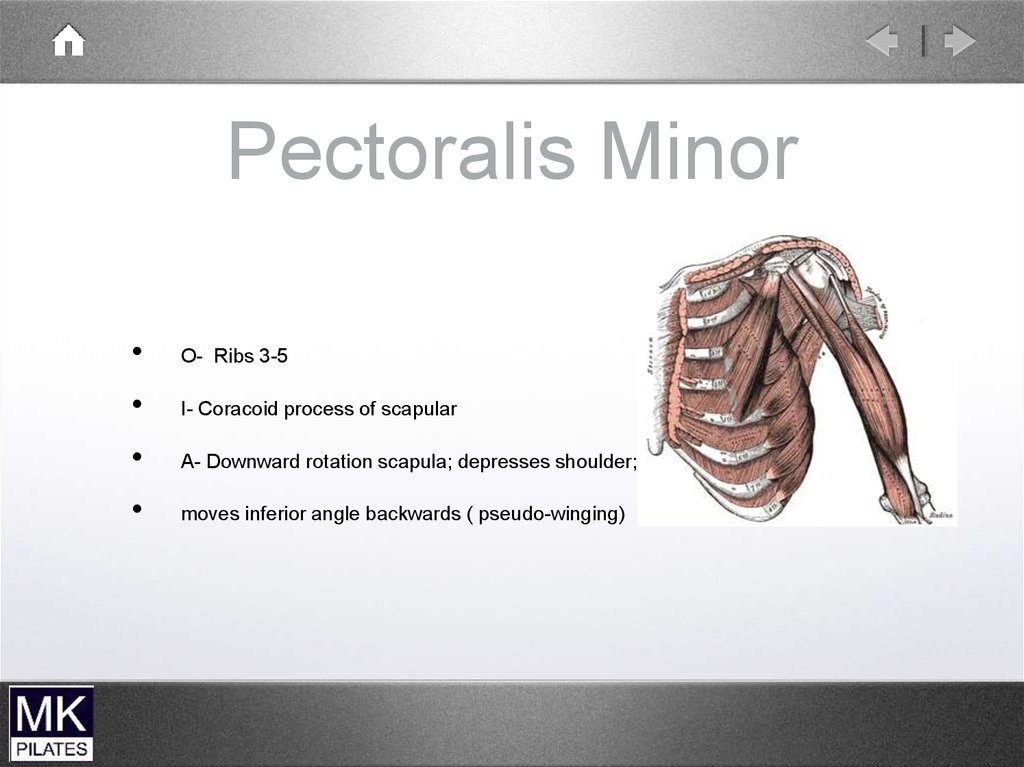
Pectoralis MinorO- Ribs 3-5
I- Coracoid process of scapular
A- Downward rotation scapula; depresses shoulder;
moves inferior angle backwards ( pseudo-winging)
87.
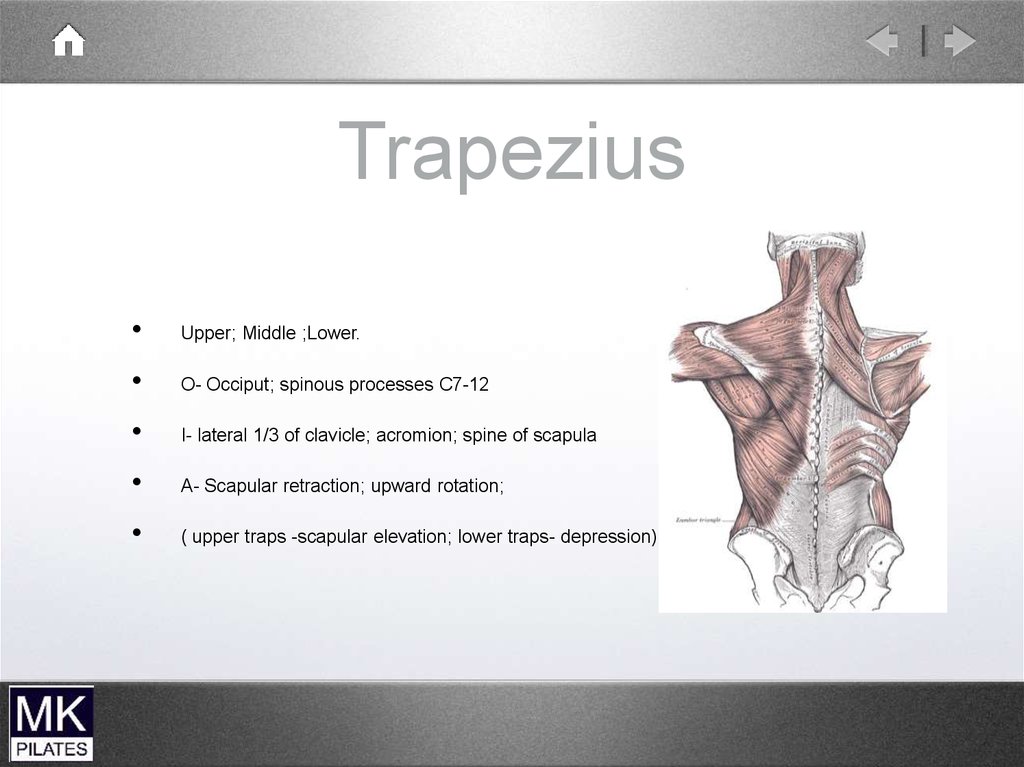
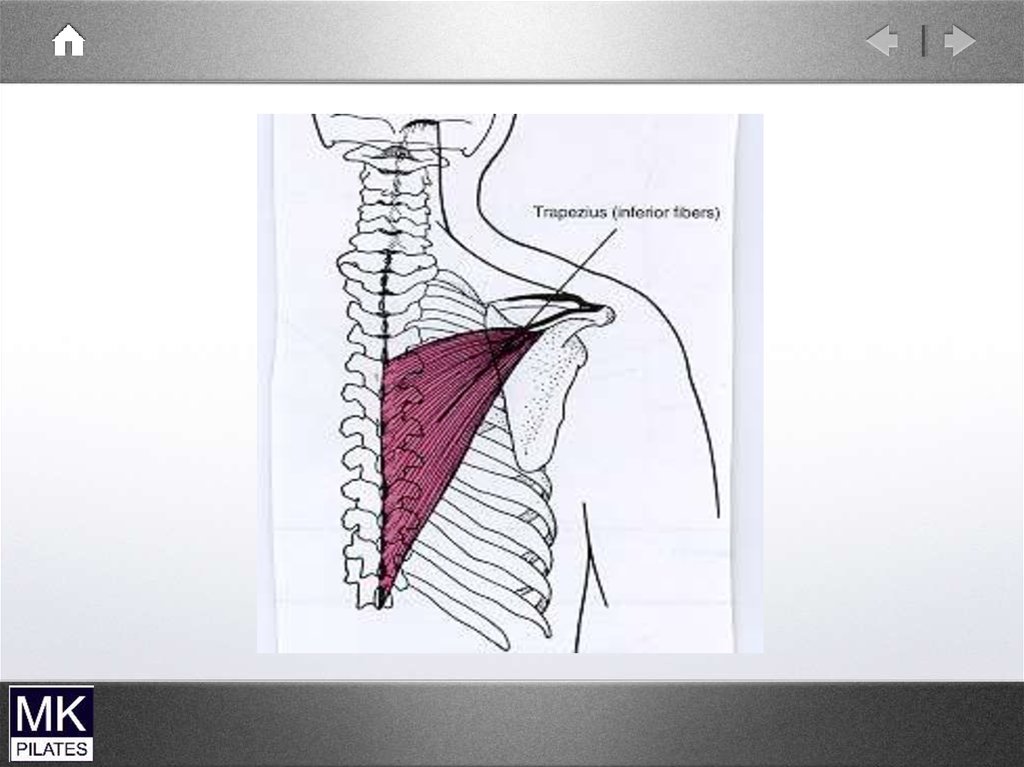
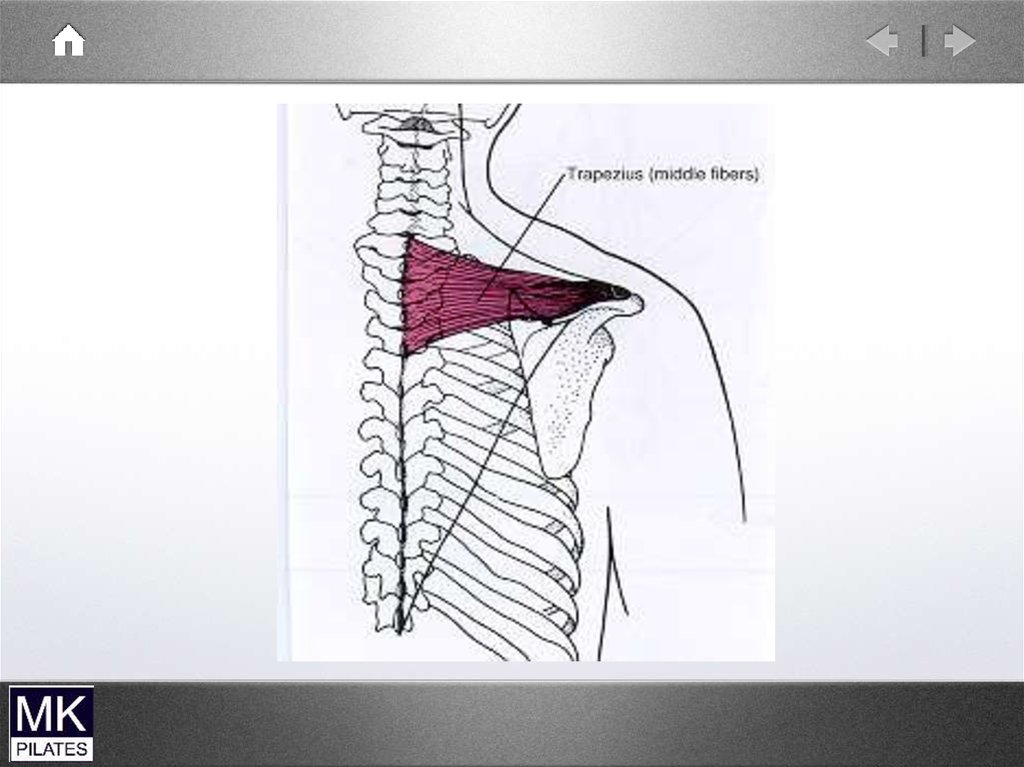
TrapeziusUpper; Middle ;Lower.
O- Occiput; spinous processes C7-12
I- lateral 1/3 of clavicle; acromion; spine of scapula
A- Scapular retraction; upward rotation;
( upper traps -scapular elevation; lower traps- depression)
88.
89.
90.
Levator ScapulaeO- C1-4
I- vertebral border of scapula
A- scapular elevation; scapular elevation
91.
RhomboidsMajor and Minor
O- spinous processes C7 to T5
I- root of spine of scapula
A- Downward rotation of scapula;
retraction of scapula
92.
Serratus AnteriorO- Fleshy digitations from upper 9 ribs
I- Medial border of scapula (interdigitates with external oblique)
A- Protraction of scapula;
Force couple with traps -upward rotation of scapula
(interdigitates with external oblique)
93.
• SupraspinatusScapula to Humerus
• Infraspinatus
• Teres Minor
• Subscapularis
• Deltoid
• Coracobrachialis
• Teres Major
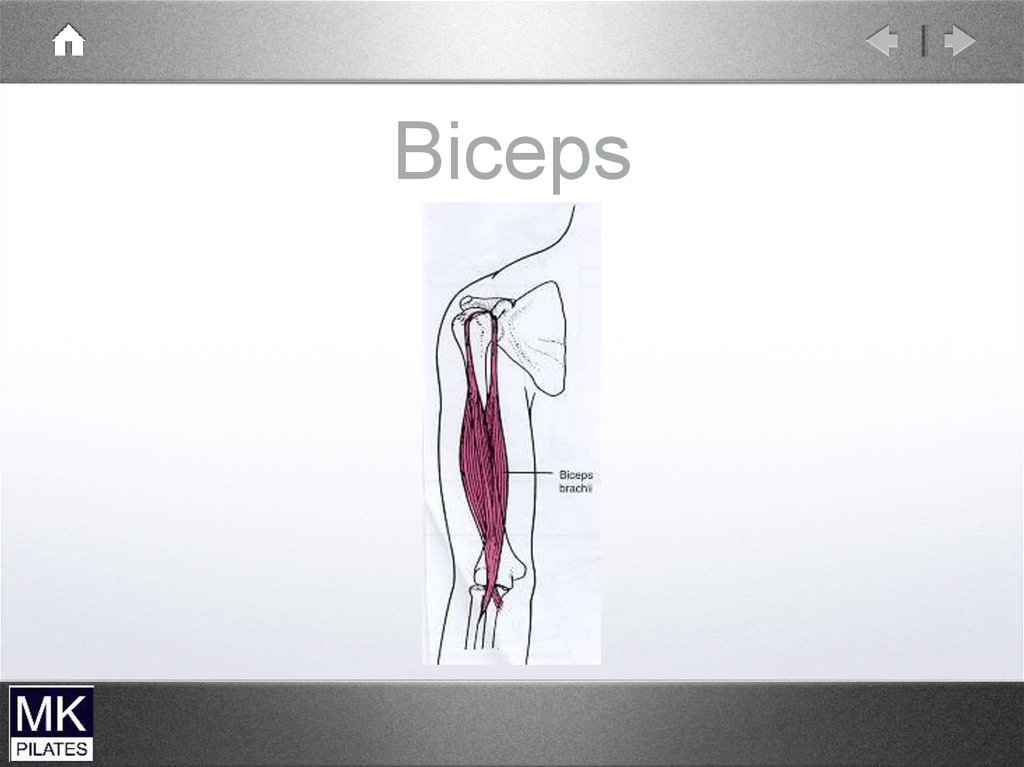
• Biceps (long head)
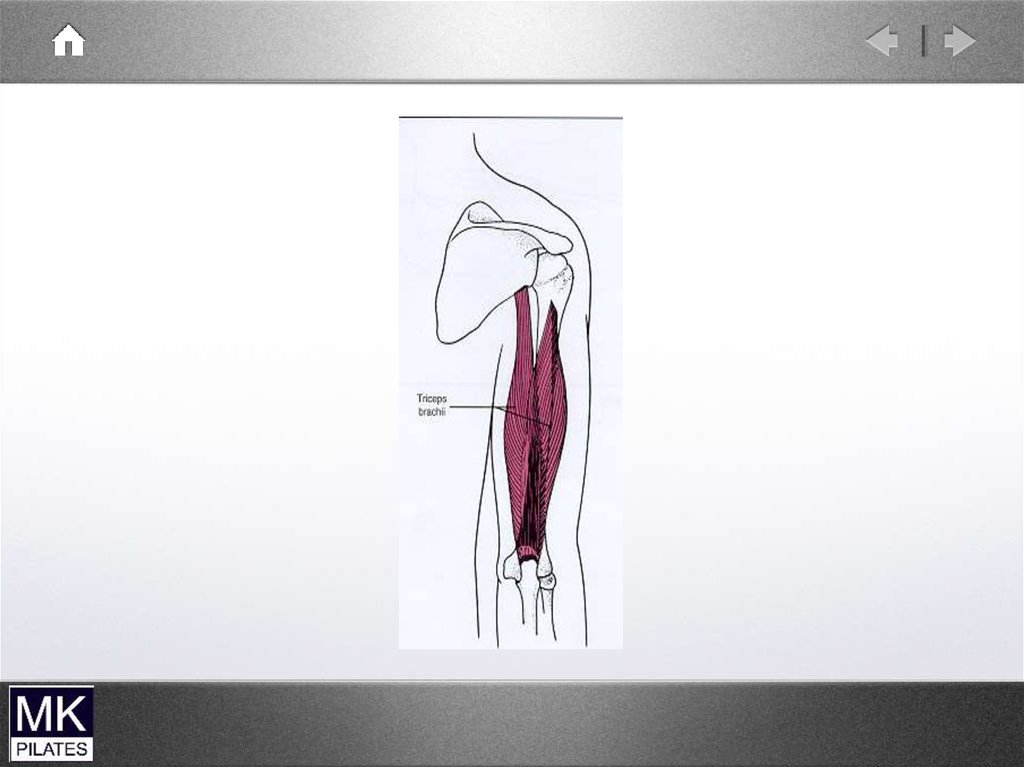
• Triceps(long head)
94.
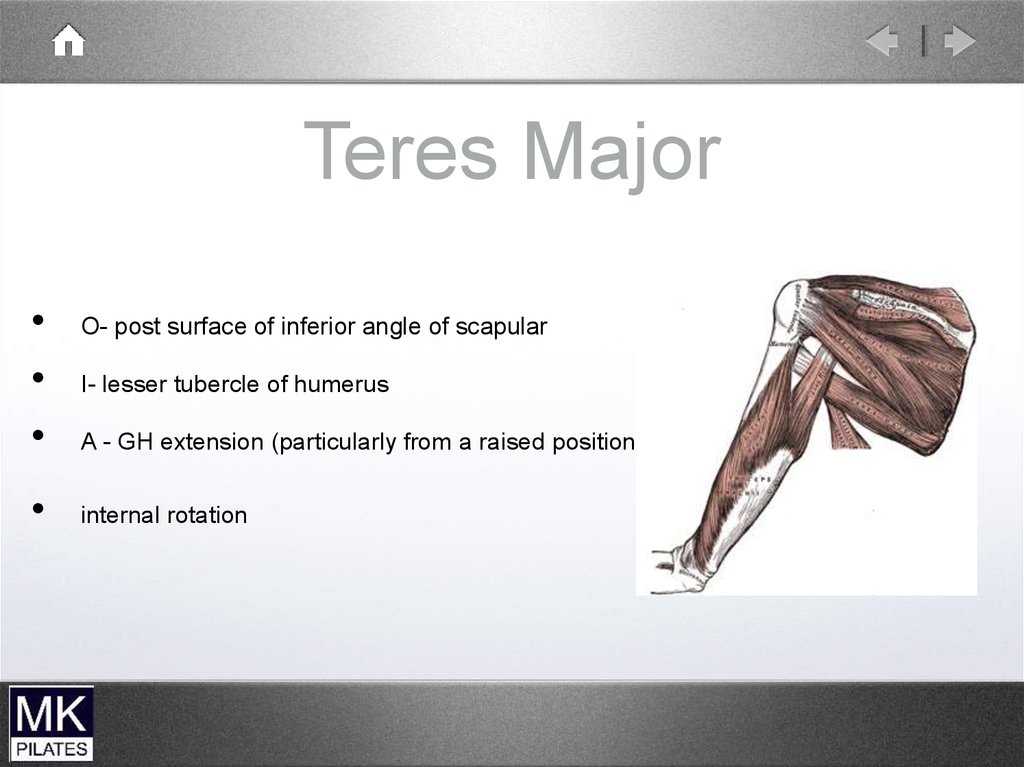
Teres MajorO- post surface of inferior angle of scapular
I- lesser tubercle of humerus
A - GH extension (particularly from a raised position)
internal rotation
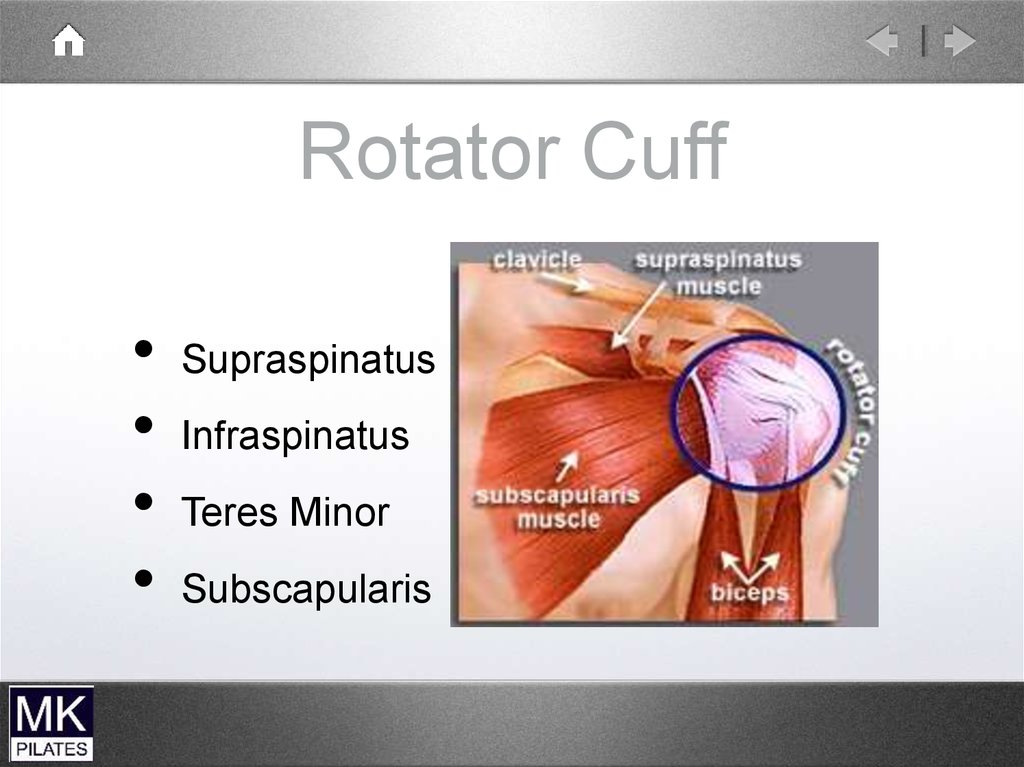
95.
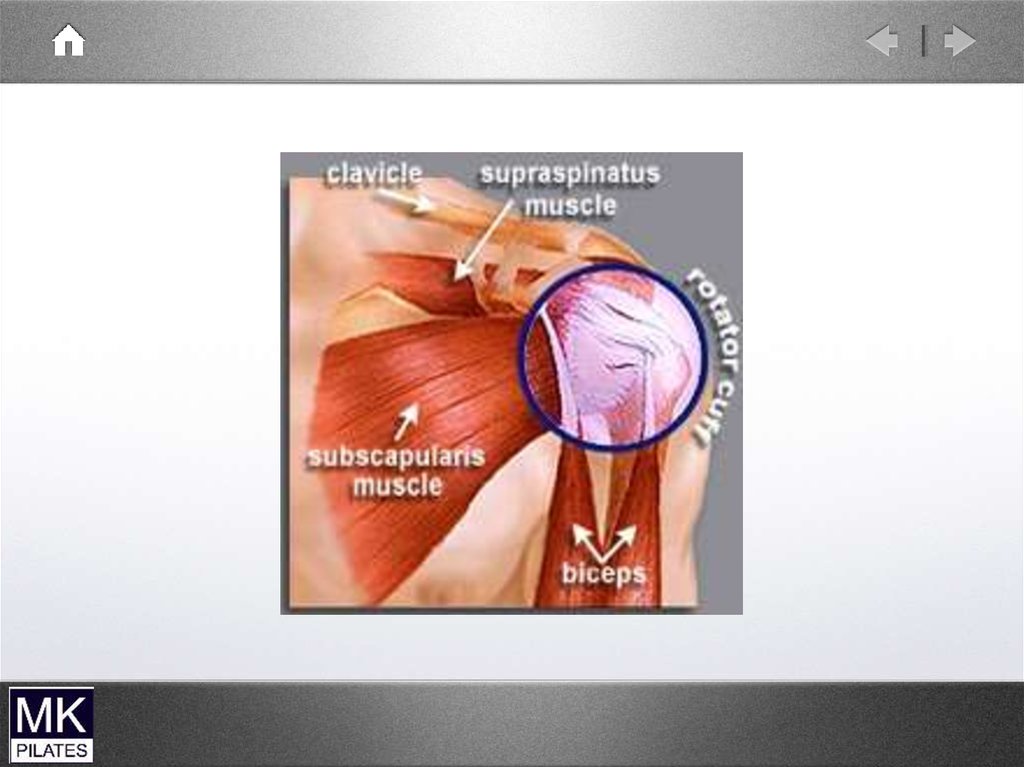
Rotator CuffSupraspinatus
Infraspinatus
Teres Minor
Subscapularis
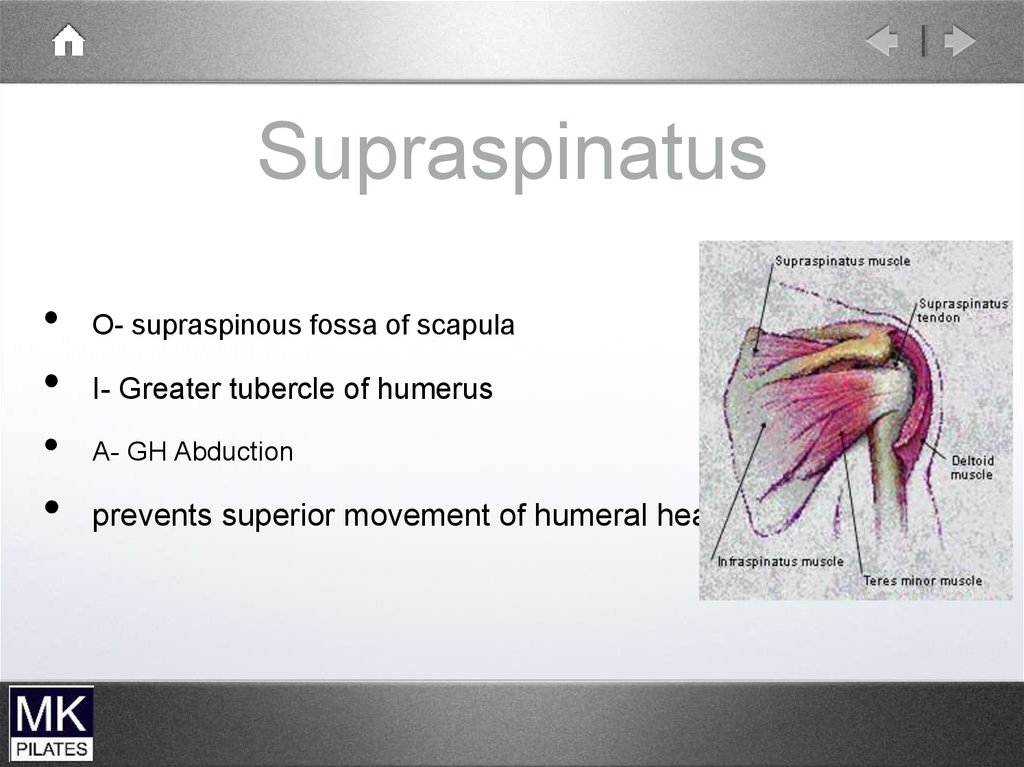
96.
SupraspinatusO- supraspinous fossa of scapula
I- Greater tubercle of humerus
A- GH Abduction
prevents superior movement of humeral head
97.
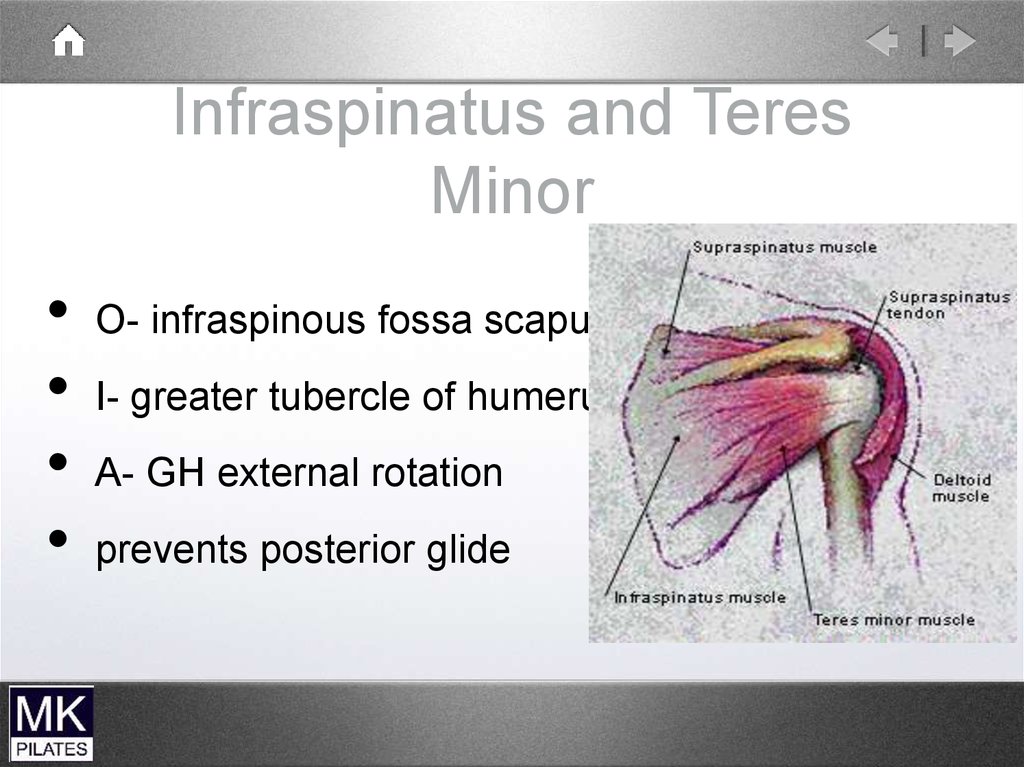
Infraspinatus and TeresMinor
O- infraspinous fossa scapula
I- greater tubercle of humerus
A- GH external rotation
prevents posterior glide
98.
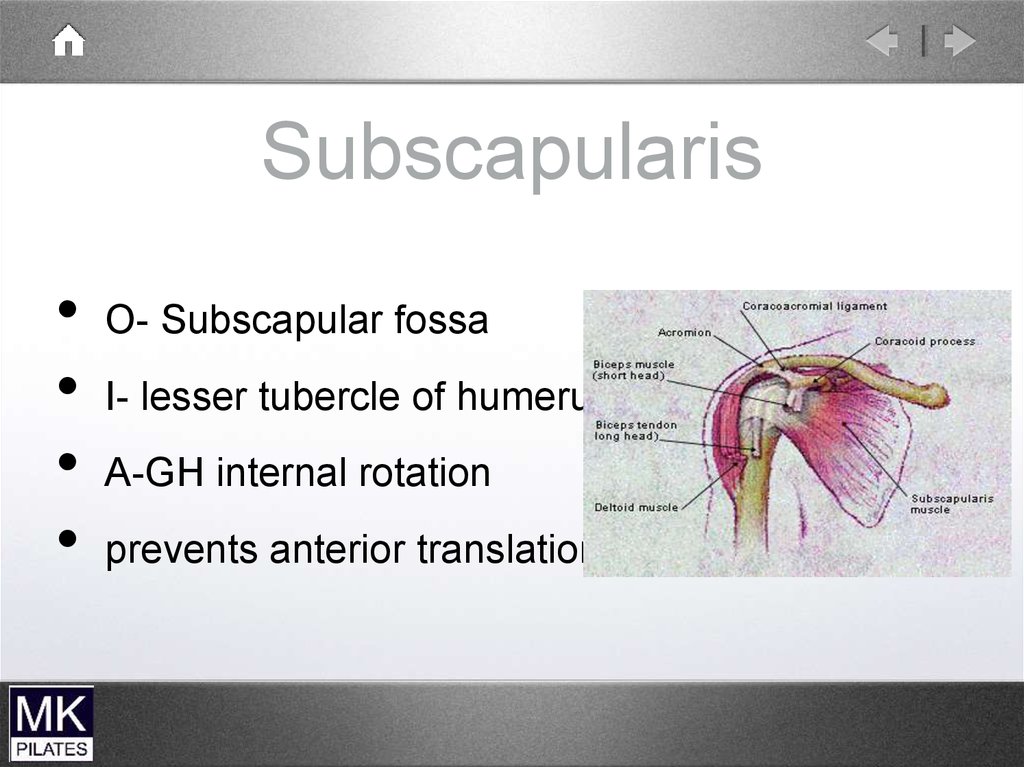
SubscapularisO- Subscapular fossa
I- lesser tubercle of humerus
A-GH internal rotation
prevents anterior translation
99.
100.
101.
Biceps102.
Levator scapulae and uppertrapezius
103.
Scapular stabilisers
Serratus anterior
protracts the scapula
upward rotation of the glenoid
Trapezius
Upper and Middle fibres retract and upwardly
rotate
Lower fibres upward rotation of glenoid and
counterbalance lateral pull of serratus anterior
104.
Scapula Mobility• Levator Scapulae
-scapula elevation
Muscles
-glenoid downward rotation
Pectoralis minor -glenoid downward
rotation
-pseudo winging
Rhomboids -scapula elevation and
retraction
-glenoid downward rotation
105.
Glenohumeral StabilitySupraspinatus - abduction
- resists anterior translation
Infraspinatus and Teres Minor
- external rotation
- resist posterior translation
Subscapularis
-medial rotation
resists anterior translation
-
106.
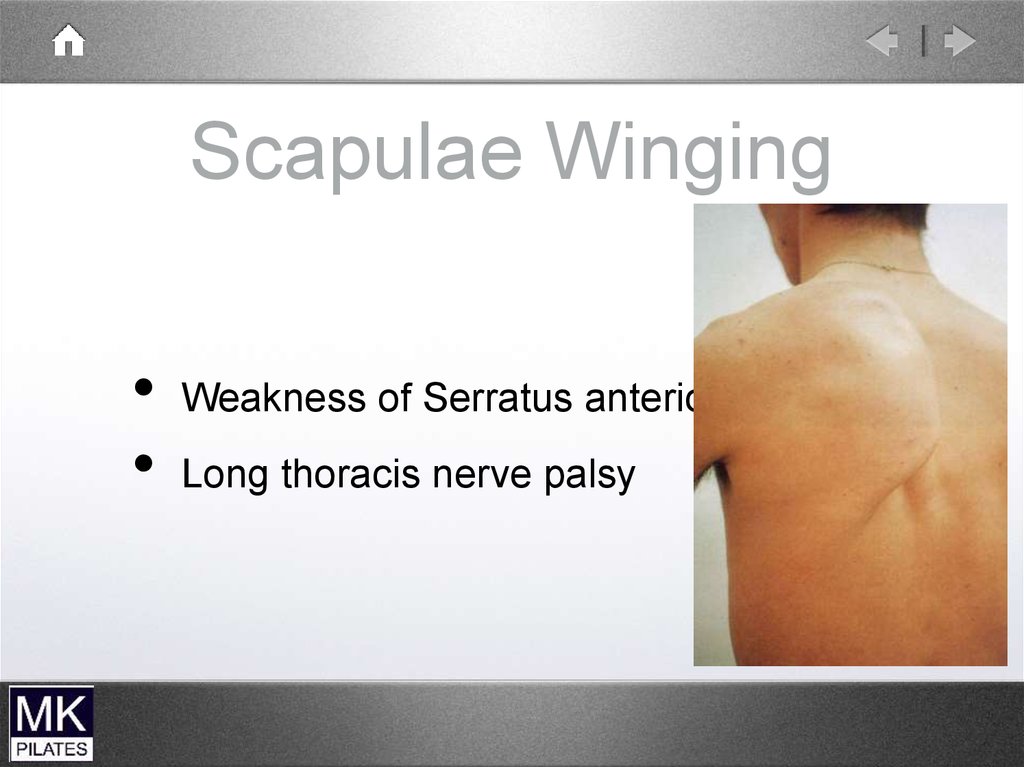
Scapulae WingingWeakness of Serratus anterior
Long thoracis nerve palsy
107.
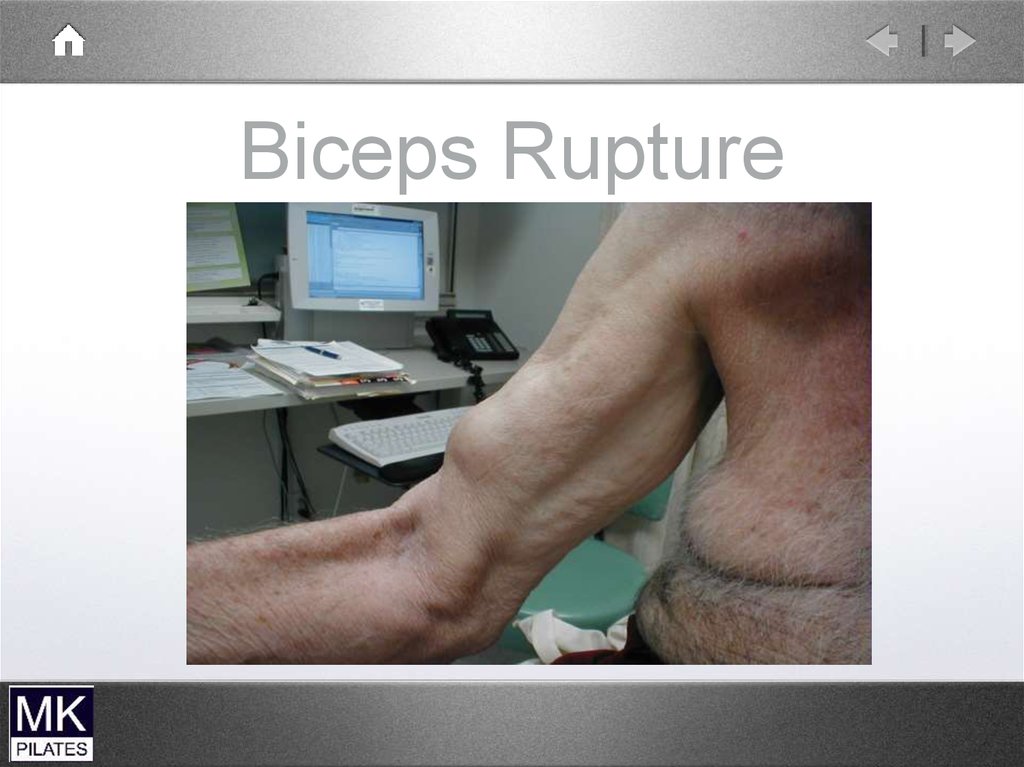
Biceps Rupture108.
109.
110.
111.
112.
113.
114.
115.
116.
The to do list gets longer117.
And at some point we’ve all hadenough – pity it’s 9am on Monday!