



















")


















































")
")











 medicine
medicine psychology
psychologySimilar presentations:










Classifications of psychiatric disorder
1. Classifications of psychiatric disorder
2. Normal vs Psychopathology
Mental health is defined as a state of well-being in which everyindividual realizes his or her own potential, can cope with the normal
stresses of life, can work productively and fruitfully, and is able to make
a contribution to
her or his community
The positive dimension of mental health is stressed in WHO's definition
of health as contained in its constitution: "Health is a state of complete
physical, mental and social well-being and not merely the absence of
disease or infirmity.“
Psychopathology is a term which refers to either the study of mental
illness or mental distress or the manifestation of behaviours and
experiences which may be indicative of mental illness or psychological
impairment
3. Purposes of Classification:
1.2.
3.
4.
To make generally acceptable diagnosis.
To facilitate communication between
psychiatrists, other doctors and professionals.
To make generalizations in treatment response,
course & prognosis of individual patients.
To make framework for research in psychiatry.
4. Hystory
The first attempt to classify such afflictions was by the Greek physicianHippocrates in 400 BC, who believed that mental illness stemmed from
imbalances of a person's black bile, yellow bile, phlegm, and blood. Different
imbalances resulted in particular symptoms which could be split into the
following categories: Mania, Melancholy, Phrenitis (brain inflamation), Insanity,
Disobedience, Paranoia, Panic, Epilepsy, and Hysteria.
Inspired by botanical taxonomy (the classification of plants), a French physician
called François Boissier de Sauvages de Lacroix published a system of
classifying illness in 1763. This classification included mental illnesses,
subdivided into four categories: 1) Hallucinations, 2) Morositates, 3) Deliria, and
4) Folies Anomales. Within these categories were some familiar symptoms
including induced vomiting, mania, amnesia, hypersexuality, panic, and
insomnia. Other symptoms, like "the uncontrollable impulse to dance" and
"non-aggressive delirium with accompanying sadness caused by the devil" are
a world away from the Western psychiatric manuals we know today.
5. Hystory
The 19th century saw more attempts to classify mental illness. InGermany, Karl Kahlbaum published his 'Classification of Psychiatric
Diseases and Mental Disturbances' (1863), positing a system which
classified mental illnesses by their symptoms. Rejecting the tradition of
labelling a symptom as a particular illness, he conceptualised
psychiatric diagnoses as clusters of symptoms: mania as a symptom of
a disorder instead of a disorder in itself. Kahlbaum employed many
terms that we still use today including Dysthymia, Cyclothymia,
Catatonia, Paranoia, and Hebephrenia. Inheriting Kahlbaum's ideas,
Emil Kraeplin, in the late 19th and early 20th century, proposed a
system in which a disorder was defined not only by the symptoms that
constitute it, but also by the patterns and course in which it presents.
Famously, he differentiated between Psychotic Disorders and Affective
Disorders, providing the foundations for what we now refer to as
Schizophrenia and Bipolar Disorder.
6.
Psychiatric DisordersOrganic
Non-Organic
Acute
Chronic
Others
Psychoses
Neuroses
Others
Delirum
Dementia
Alcohol …
Schizophrenia
Anxiety disorders
Personality dis.
Wernicke’s
Korsakoff
Head Injury
Mood disorders
Adjustment dis.
Sleep disorder
Etc….
Etc….
Dysthymia
Sex disorder
Dissociative dis.
Suicide
7. Neurosis and Psychosis
Psychosis:- unsatisfactory term
- refers broadly to severe forms of mental disorders such as:
a. organic mental diseases
b. schizophrenia
c. affective disorders
Characteristics:
- greater severity
- lack of insight
- patient’s inability to distinguish between subjective experience
and reality e.g. hallucinations, delusions.
8. Neurosis and Psychosis
Neurosis:- unsatisfactory term.
- Refers to mental disorders that are generally
less severe than psychosis.
Characteristics:
- Symptoms are closer to normal experience
e.g. anxiety.
9. History of the DSM
•In 1918, the American Medico-Psychological Association (presently the AmericanPsychological Association, or APA) issued the Statistical Manual for Use of
Institutions for the Insane. It did not catch on.
•In 1928, the American Psychiatric Association issued another edition but it was too
narrowly focused. It looked primarily at neuroses and psychoses.
•By World War II, the military had its own nomenclature system.
•The World Health Organization (WHO) issued the International Classification of
Diseases-6 (ICD-6); it contained a section on mental disorders but it needed
modification for use in the United States.
DSM-I-1952
DSM-II-1968
DSM-III-1980
DSM-III-R-1987
DSM-IV-1994
DSM-IV-TR-2000
DSM--52013
10. DSM-5—Diagnostic and Statistical Manual of Mental Disorders
The fifth edition of the Diagnostic andStatistical Manual of mental disorders (DSM5) is a guidebook utilized by physicians and
other healthcare professionals in the United
States as well as in many other nations of
the world. DSM-5 is a standardized volume
that details and classifies mental disorders
for the improvement of diagnosis, treatment,
and research in the psychiatry field.
11. Top 10 Most Significant Changes in the DSM-5
Top 10 Most Significant Changes in the DSM51.Overall “Mission Creep”
2. Discontinuation of the Multi-axial Diagnosis
3. Greater (bio)medical orientation
4. Inclusion of Section III: Emerging Measures & Models
5. Dimensionalizing Disorders (e.g. ASD, Schiz)
6. Reclassification & Re-combination of Disorders
7. Addition of Non-Substance Addictive Disorders
8. Movement towards “Clinical Utility” vs. “Validity”
9. Movement from Roman to Arabic Numbers
10. Designed to articulate with the ICD
12. DSM 5
• NEURODEVELOPMENTAL DISORDERS (Delirium,dementia, amnesic, and other cognitive disorders).
• SCHIZOPHRENIA SPECTRUM AND OTHER
PSYCHOTIC DISORDERS
• BIPOLAR AND RELATED DISORDERS
• DEPRESSIVE DISORDERS
• ANXIETY DISORDERS
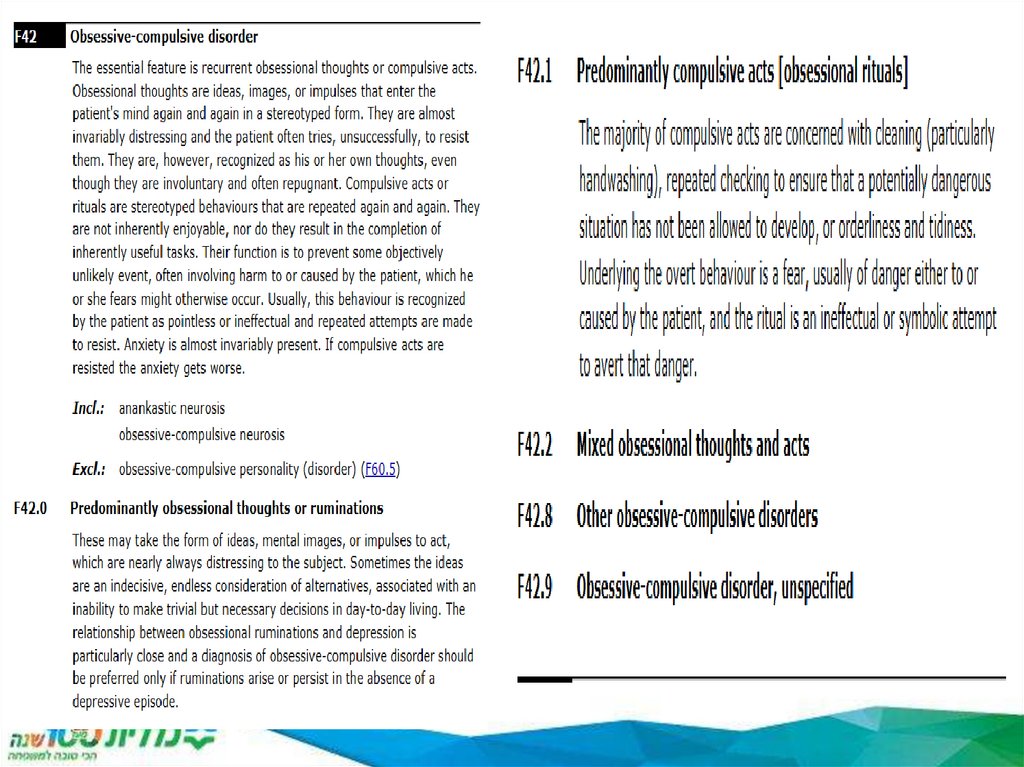
• OBSESSIVE –COMPULSIVE AND RELATED
DISORDERS
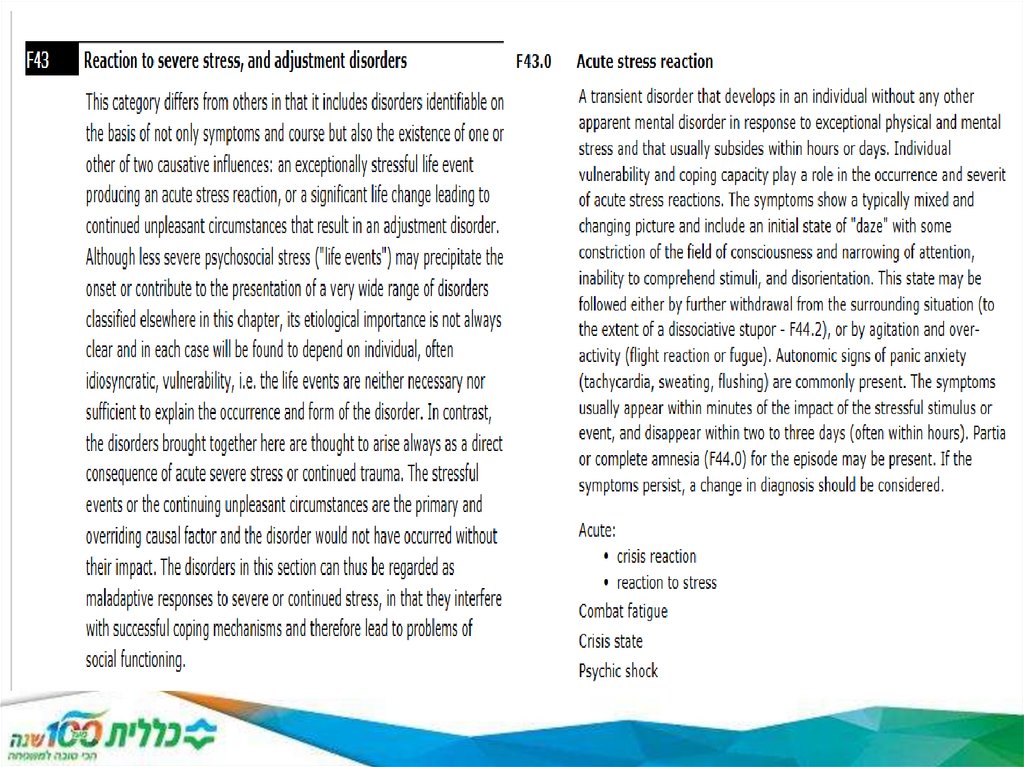
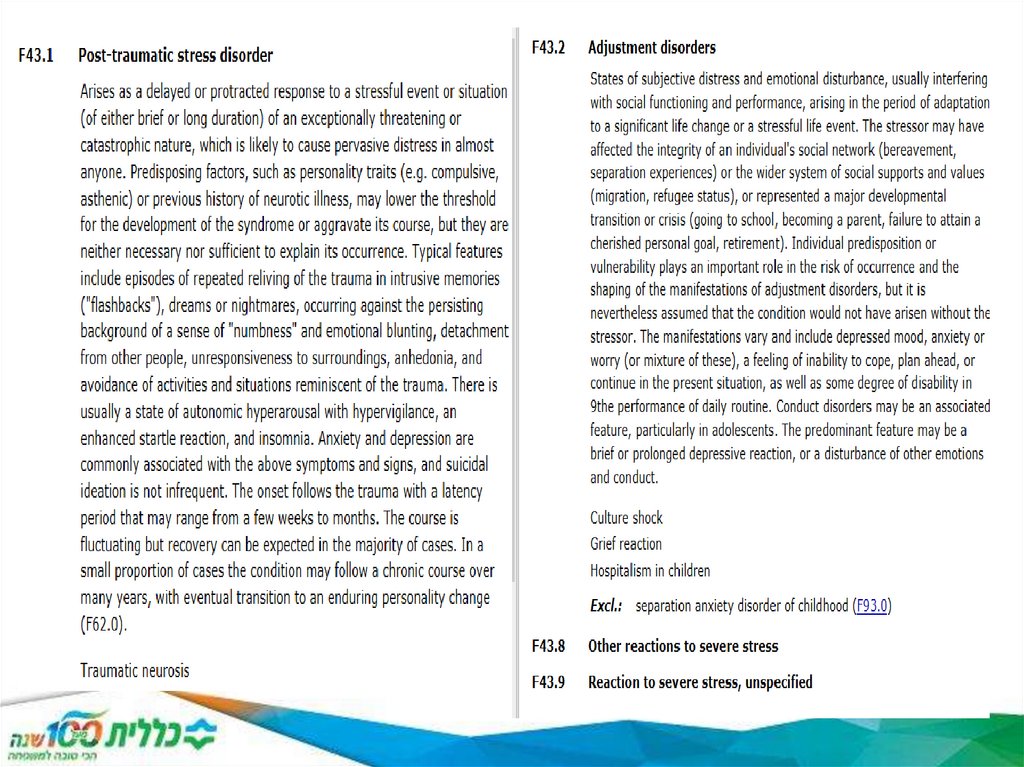
• TRAUMA AND STRESSOR RELATED DISORDERS
(anxiety disorders)
13. Hystory of the ICD
The first international classification edition, known as the International List ofCauses of Death, was adopted by the International Statistical Institute in 1893.
WHO was entrusted with the ICD at its creation in 1948 and published the 6th
version, ICD-6, that incorporated morbidity for the first time. The WHO
Nomenclature Regulations, adopted in 1967, stipulated that Member States use the
most current ICD revision for mortality and morbidity statistics. The ICD has been
revised and published in a series of editions to reflect advances in health and
medical science over time.
ICD-10 was endorsed in May 1990 by the Forty-third World Health Assembly. It is
cited in more than 20,000 scientific articles and used by more than 100 countries
around the world.
A version of ICD-11 was released on 18 June 2018 to allow Member States to
prepare for implementation, including translating ICD into their national languages.
ICD-11 was submitted to the 144th Executive Board Meeting in January 2019 and
the Seventy-second World Health Assembly in May 2019 and, following
endorsement, Member States will start reporting using ICD-11 on 1 January 2022.
14. ICD-10
ICD is the foundation for the identification of healthtrends and statistics globally, and the international
standard for reporting diseases and health conditions. It
is the diagnostic classification standard for all clinical and
research purposes. ICD defines the universe of
diseases, disorders, injuries and other related health
conditions, listed in a comprehensive, hierarchical
fashion that allows for:
easy storage, retrieval and analysis of health information
for evidenced-based decision-making;
sharing and comparing health information between
hospitals, regions, settings and countries; and
data comparisons in the same location across different
time periods.
15. Structural Differences ICD-10-CM Diagnoses
Structural Differences ICD-10-CM
Diagnoses
ICD-10-CM has three to seven digits:
• Digit 1 is alpha (A – Z, not case sensitive).
• Digit 2 is numeric.
• Digit 3 is alpha (not case sensitive) or numeric.
• Digits 4 – 7 are alpha (not case sensitive) or numeric.
• If there is a decimal, it is always after the 3rd character.
• ICD-9-CM has 14,025 codes, while ICD-10-CM has 68,069 codes.
2014 ICD-10-CM Code
F70
F31.2
F20.0
2014 ICD-10-CM Description
Mild intellectual disabilities.
Bipolar disorder, current episode manic
severe with psychotic features.
Paranoid schizophrenia.
DSM-5 Description
Intellectual disability (intellectual
developmental disorder), mild.
Bipolar I disorder, current or most recent
episode manic, with psychotic features.
ICD-9-CM Code
319
296.44
295.30
F20.9
Schizophrenia, unspecified.
Schizophrenia.
F11.221
Opioid dependence with intoxication
delirium.
Opioid Intoxication delirium, with moderate or
severe use disorder.
295.90
15
292.81
16. An Example of a Crosswalk Discrepancy
• A case of agoraphobia with panic disorder:• DSM-5 diagnosis of agoraphobia.
• ICD-10-CM crosswalk = F40.00, Agoraphobia,
unspecified.
• DSM-5 diagnosis of panic disorder.
• ICD-10-CM crosswalk = F41.0, Panic disorder
[episodic paroxysmal anxiety] without
agoraphobia.
• There is no DSM-5 category that combines
agoraphobia with panic disorder.
• In ICD-10-CM, F40.01 = Agoraphobia with
panic disorder.
16
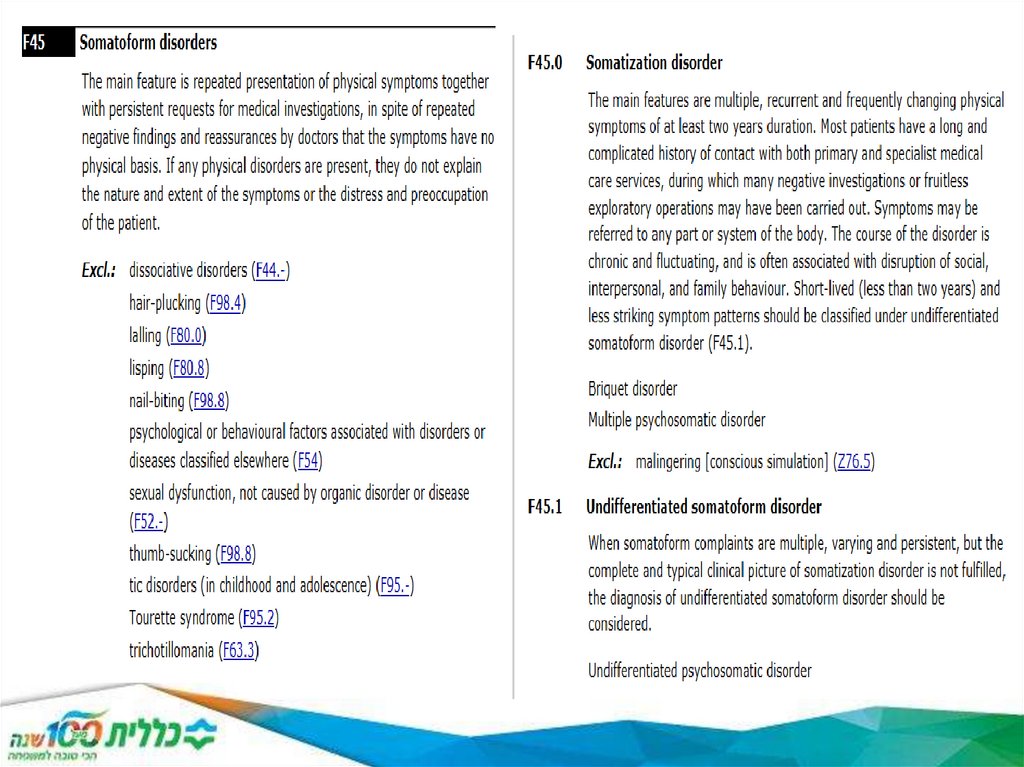
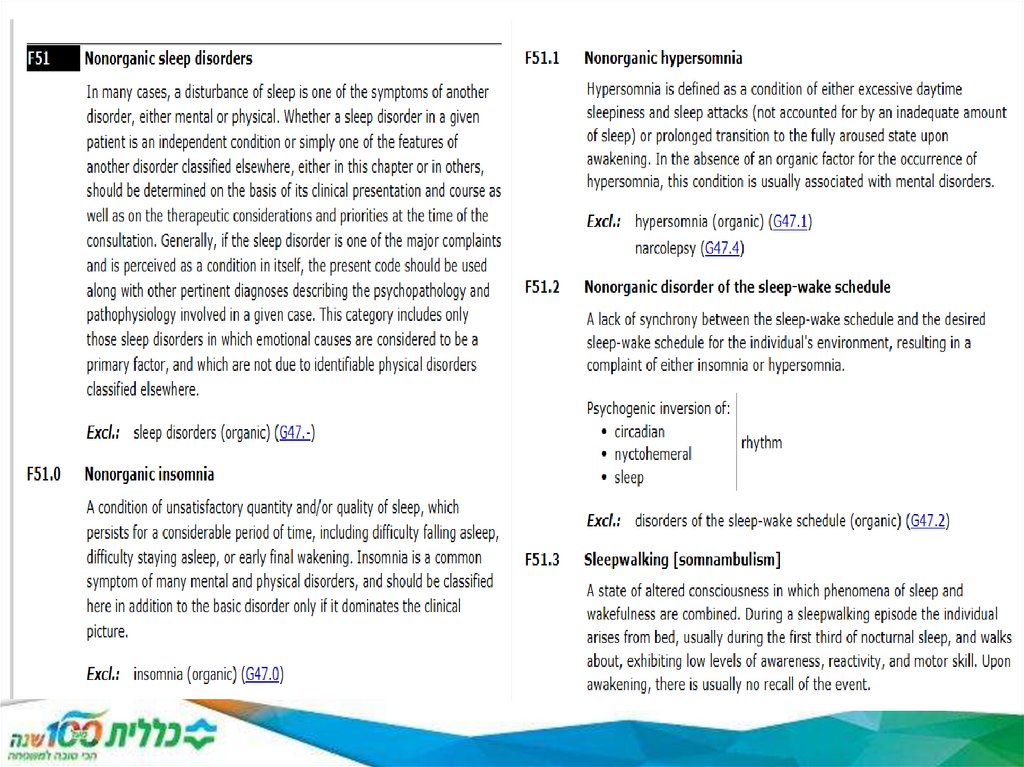
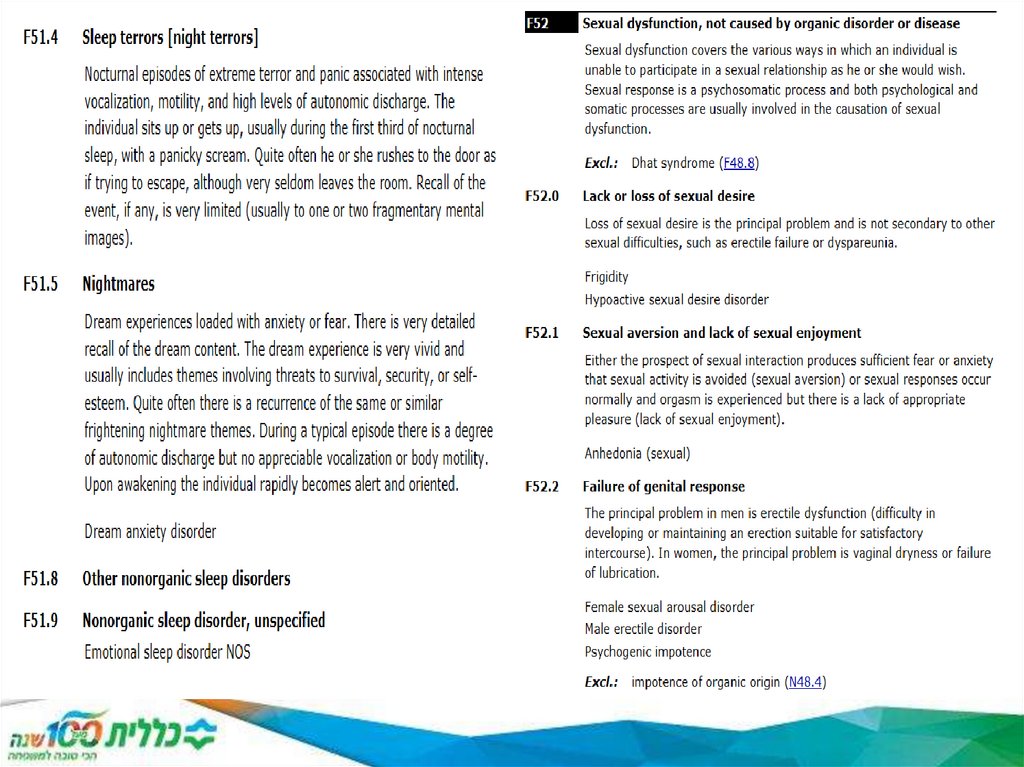
17. Framework within Chapter 5 Behavioral Health, F codes
Framework within Chapter 5ICD-10-CM Code
Description
Range Behavioral Health, F codes
F01 ‒ F09
Mental disorders due to known physiological conditions.
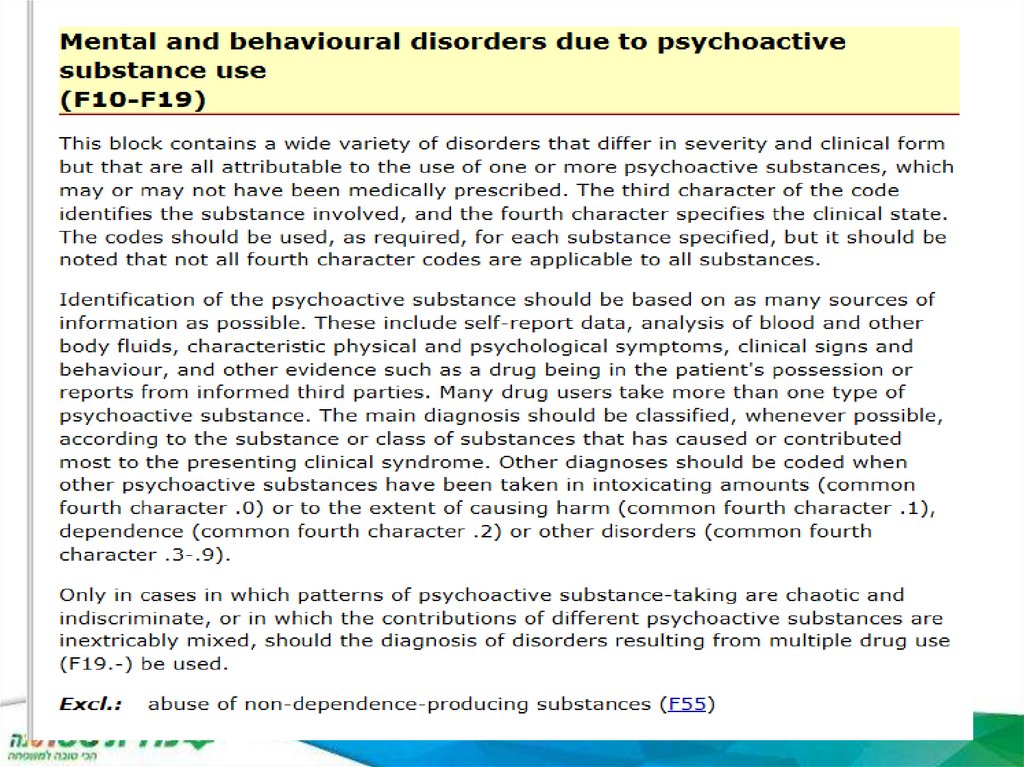
F10 ‒ F19
Mental and behavioral disorders due to psychoactive
substance abuse.
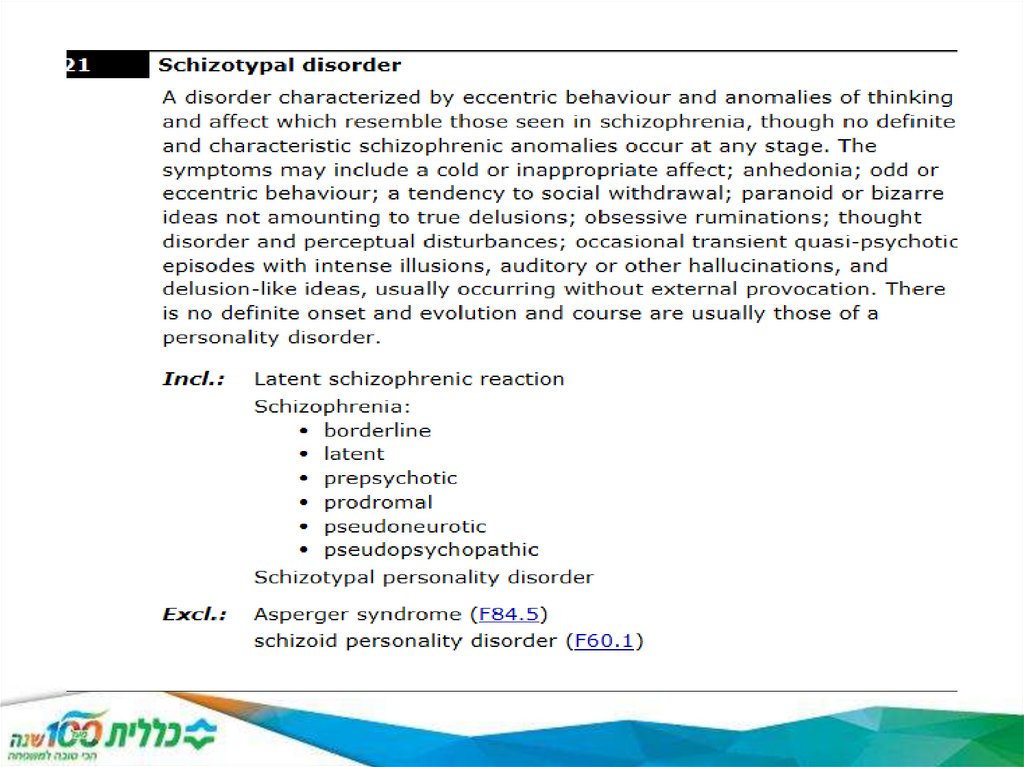
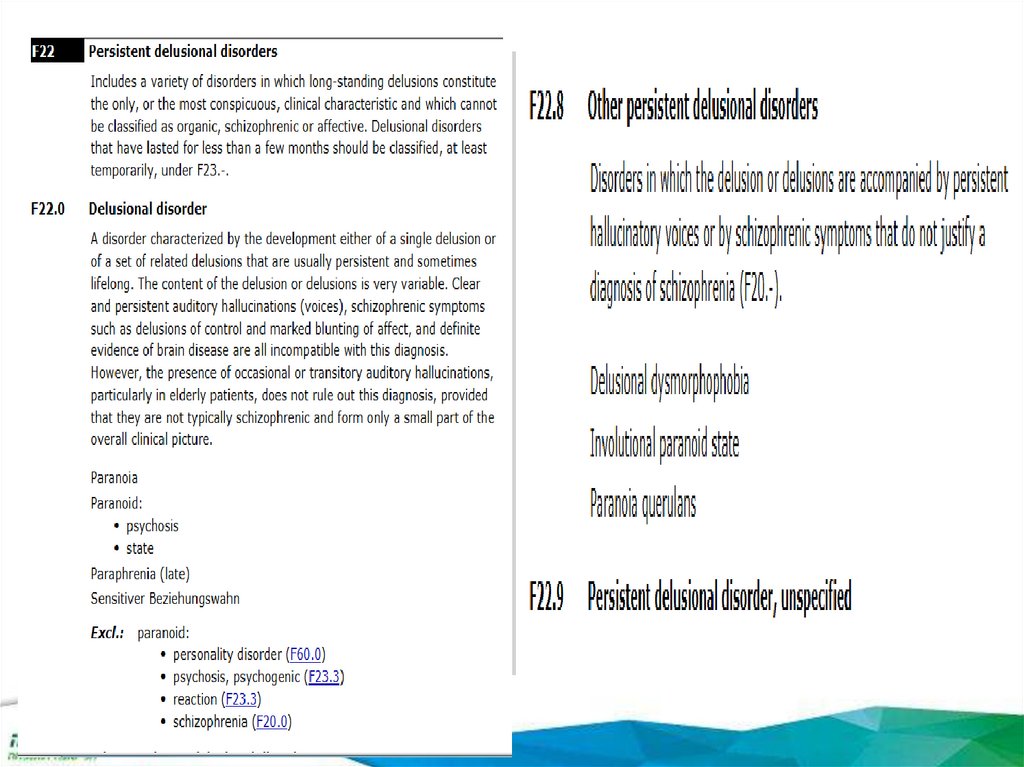
F20 ‒ F29
Schizophrenia, schizotypal, delusional, and other non-mood
psychotic disorders.
F30 ‒ F39
Mood (affective) disorders.
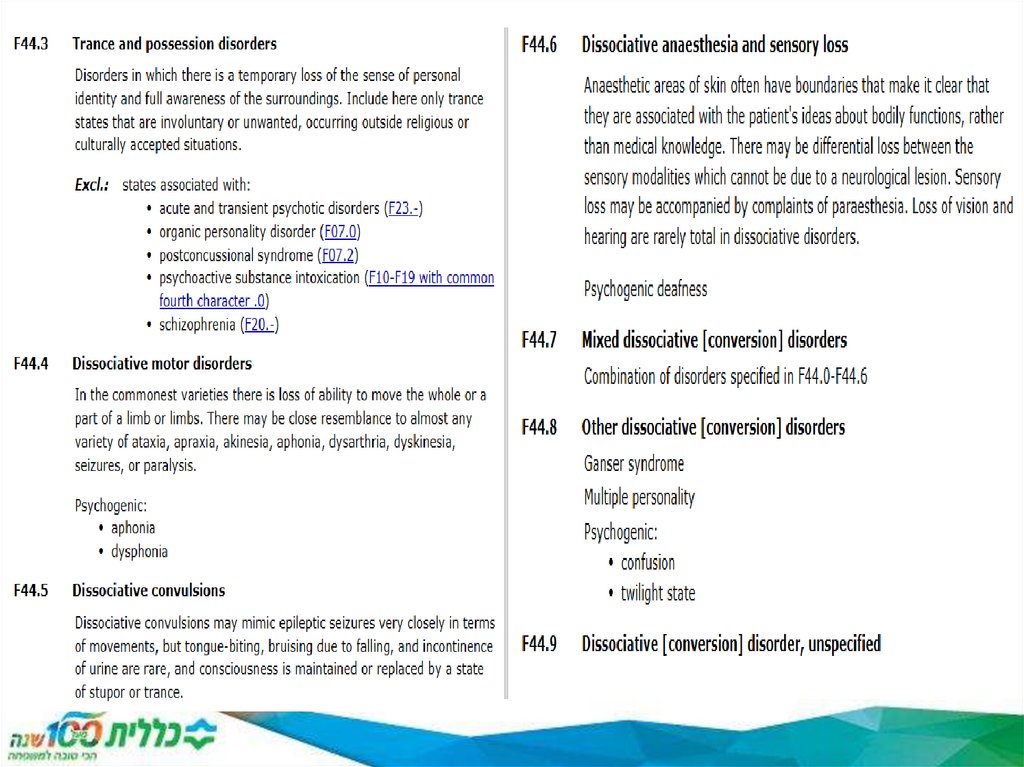
F40 ‒ F48
Anxiety, dissociative, stress-related, somatoform, and other
non-psychotic mental disorders.
F50 ‒ F59
Behavioral syndromes associated with physiological
disturbances and physical factors.
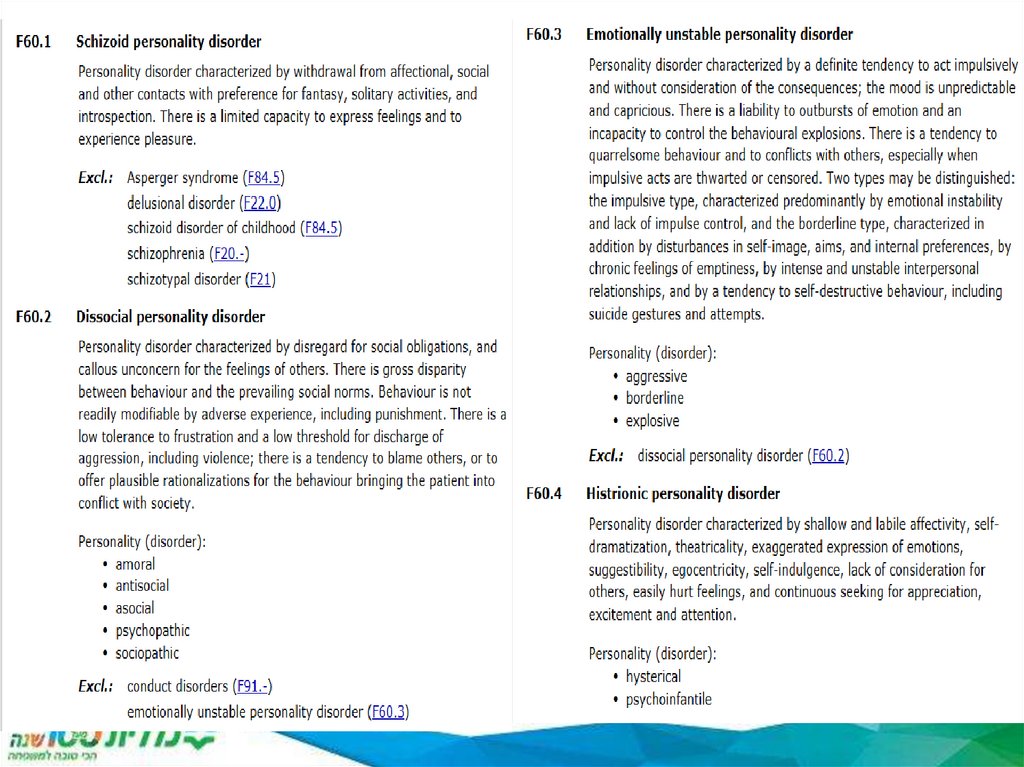
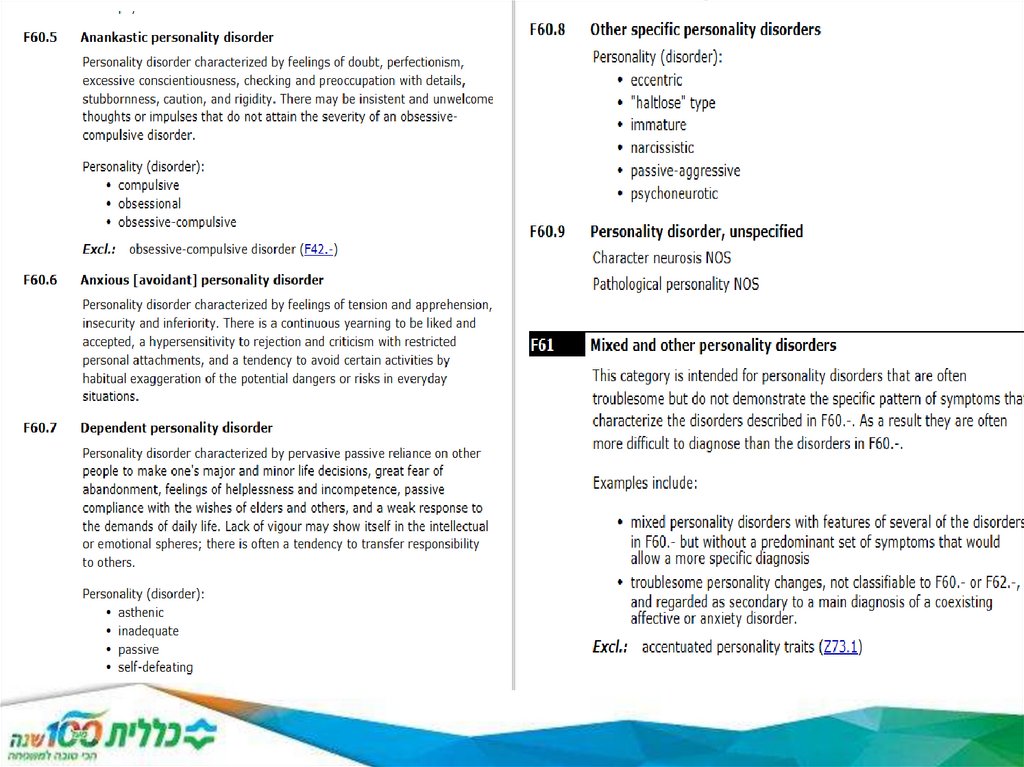
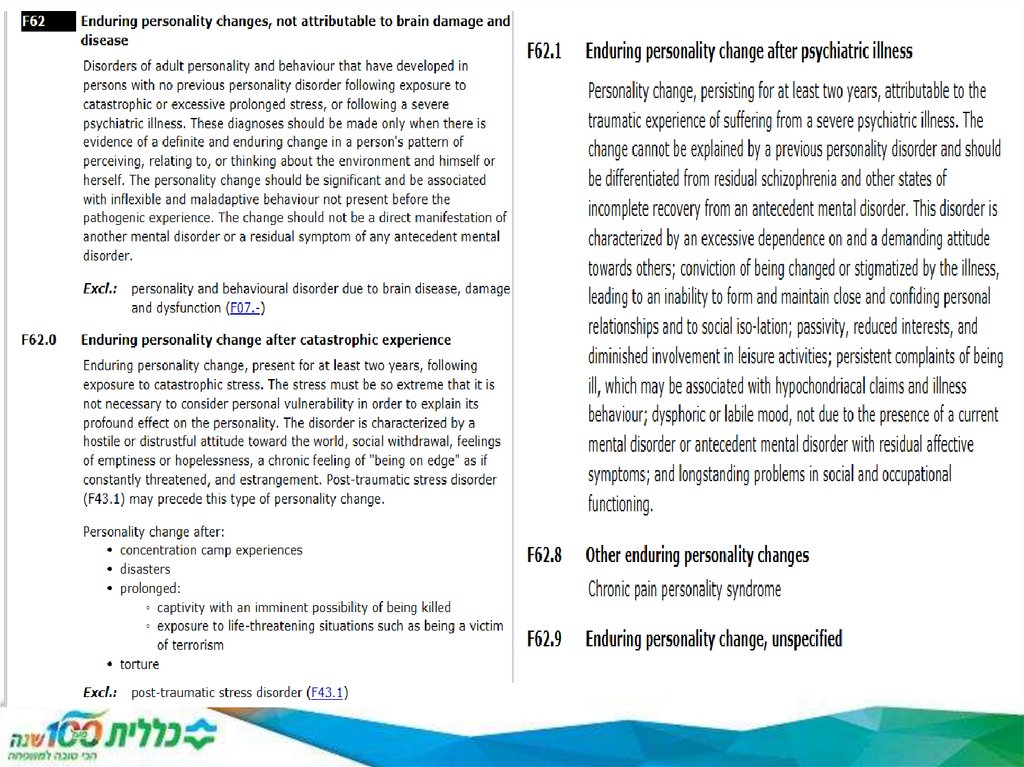
F60 ‒ F69
Disorders of adult personality and behavior.
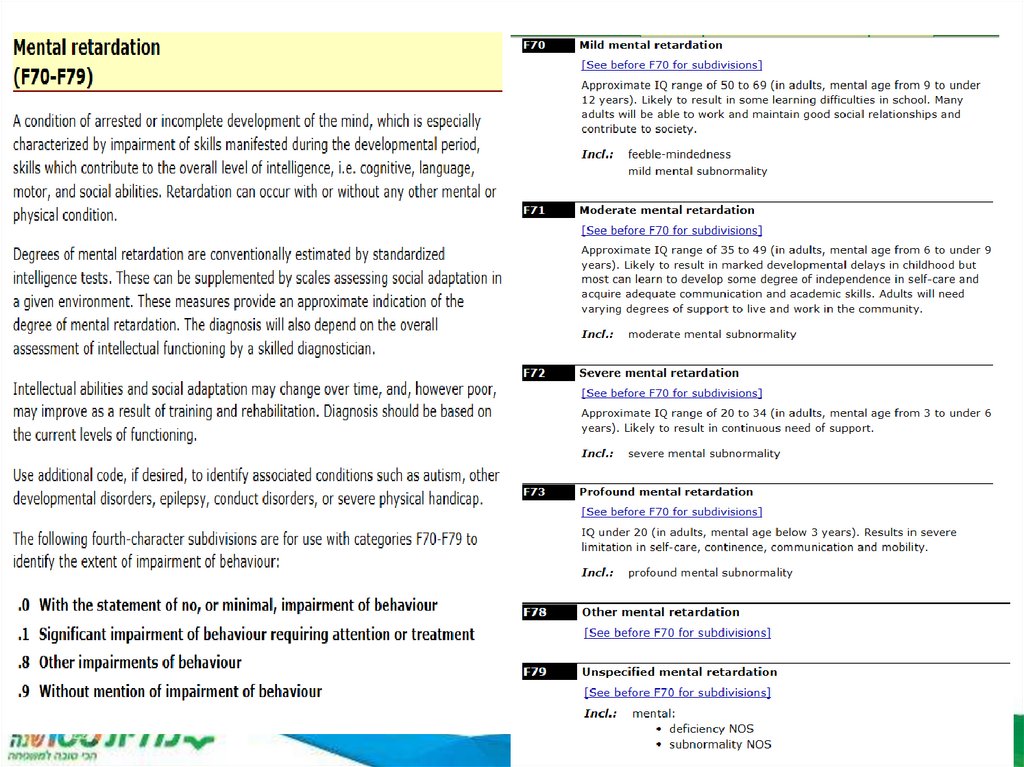
F70 ‒ F79
Intellectual disabilities.
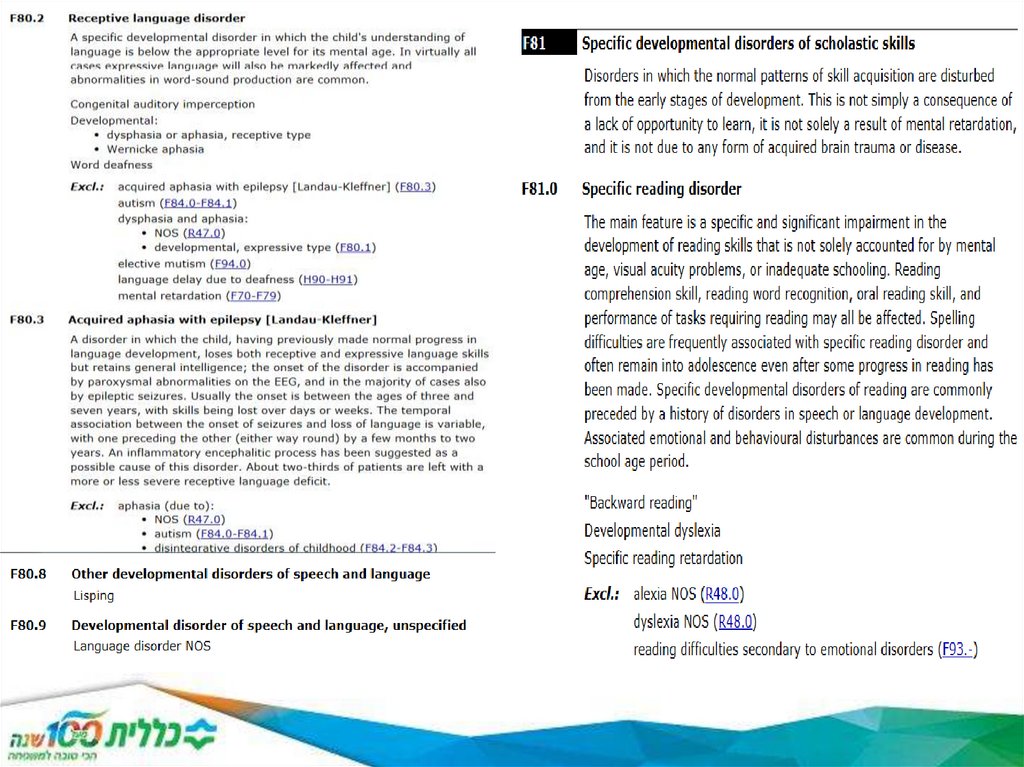
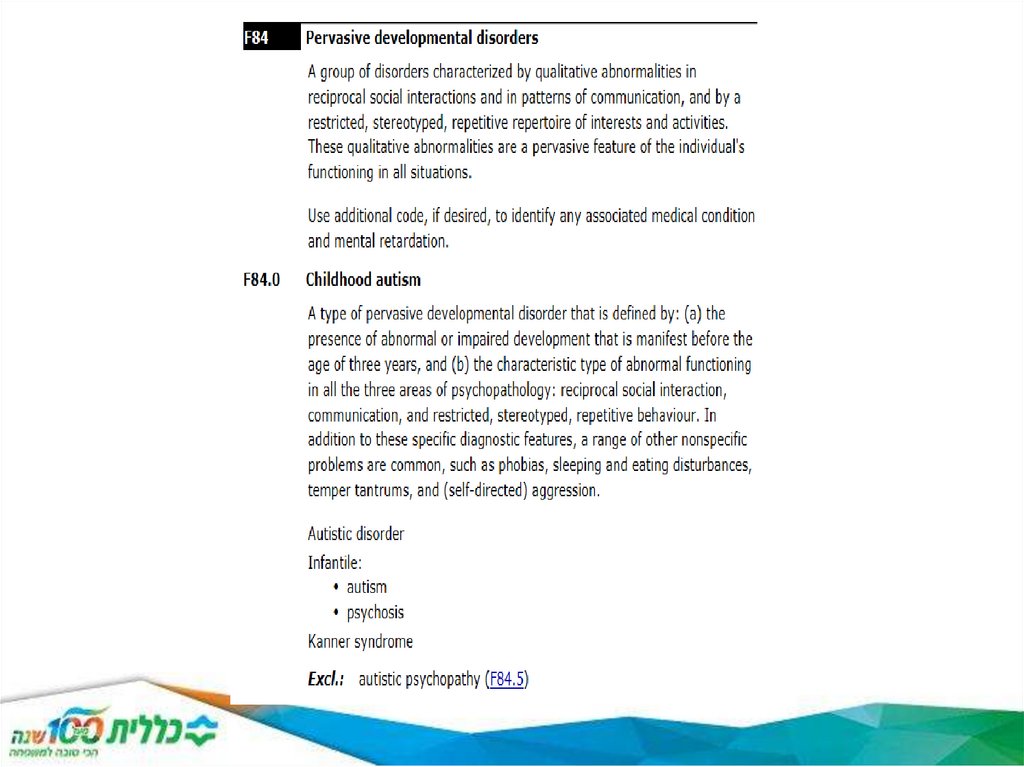
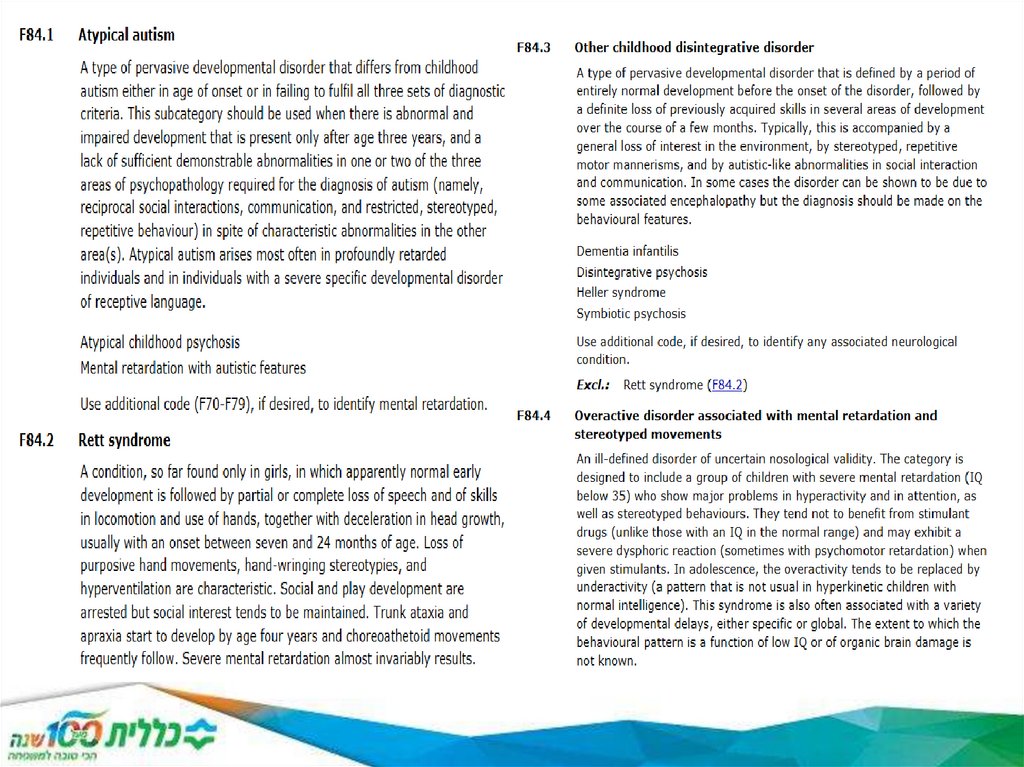
F80 ‒ F89
Pervasive and specific developmental disabilities.
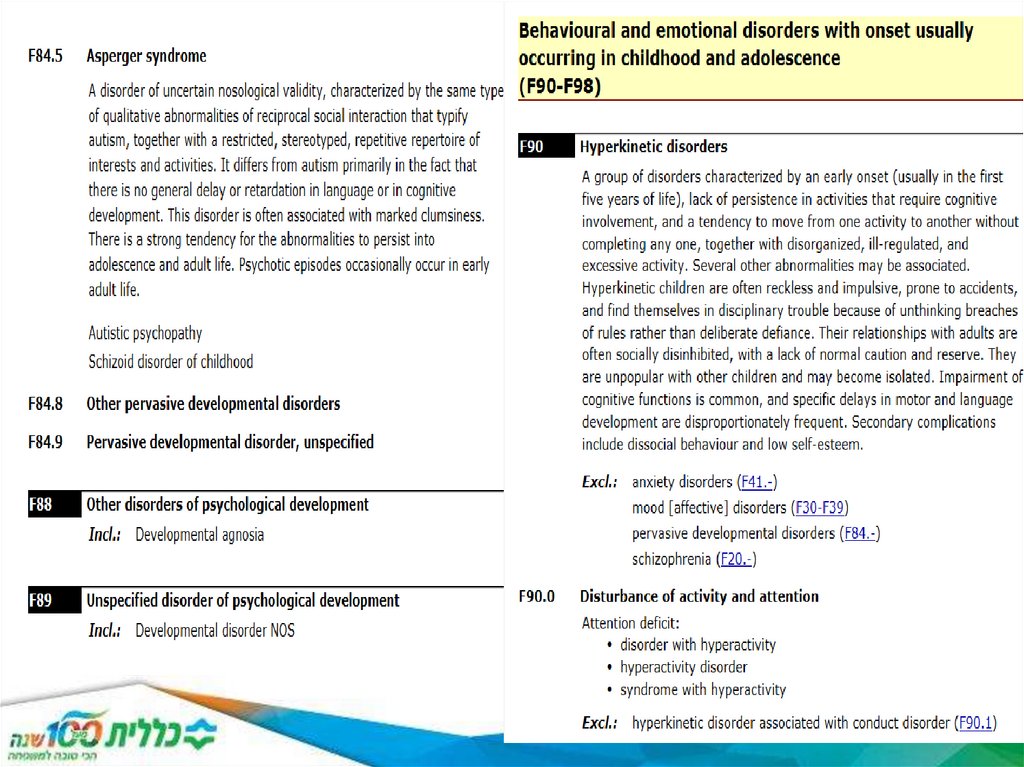
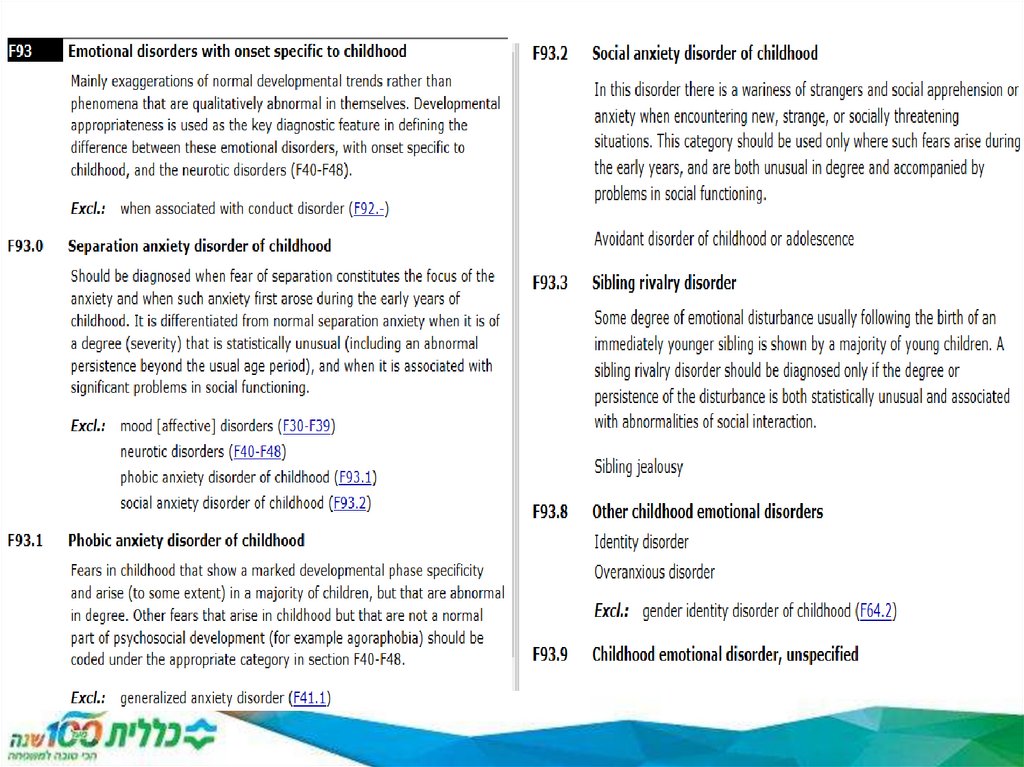
F90 ‒ F98
Behavioral and emotional disorders with onset usually
occurring in childhood or adolescence.
17
F99
Unspecified mental disorder.
18. ICD-10 Chapter V
Chapter V is used to code mental and behavioral disorders.It includes:
• disorders with an organic origin, where disease or injury
causes the mental or behavioral condition
• conditions caused by substance abuse
• psychotic and delusion conditions such as
schizophrenia
• mood disorders such as depression and mania
• behavioral and personality disorders, including those
caused by stress or traumatic events
• developmental disorders, such as hyperactivity, and
mental retardation.
19. ICD-10-CM Coding Structure Sample 1
F33.2F = Mental and Behavioral Disorders
F30-39 = Mood [affective] disorders
F33 = Recurrent Depressive Disorder
F33.2 = Recurrent Depressive Disorder, current episode
severe, without psychotic symptoms
ICD-9-CM 296.3 Major depressive disorder, recurrent
episode
DSM-5 codes: 296.33 while the ICD-9-CM is in effect, and
F33.2 for when ICD-10-CM is implemented. Harmonized.
20. ICD-10 Chapter V
There are two asterisk codes in the organic disordersblock, F00* and F02*, which are used to record dementia in
diseases recorded
using dagger codes from other chapters
21. Organic, including symptomatic, mental disorders (F00-F09)
This block comprises a range of mentaldisorders grouped together on the basis of their
having in common a demonstrable etiology in
cerebral disease, brain injury, or other insult
leading to cerebral dysfunction. The
dysfunction may be primary, as in diseases,
injuries, and insults that affect the brain directly
and selectively; or secondary, as in systemic
diseases and disorders that attack the brain
only as one of the multiple organs or systems
of the body that are involved.
22. Dementia F00-03
Dementia (F00-F03) is a syndrome due to disease of the brain, usuallyof a chronic or progressive nature, in which there is disturbance of
multiple higher cortical functions, including memory, thinking,
orientation, comprehension, calculation, learning capacity, language,
and judgement. Consciousness is not clouded. The impairments of
cognitive function are commonly accompanied, and occasionally
preceded, by deterioration in emotional control, social behaviour, or
motivation. This syndrome occurs in Alzheimer disease, in
cerebrovascular disease, and in other conditions primarily or
secondarily affecting the brain.
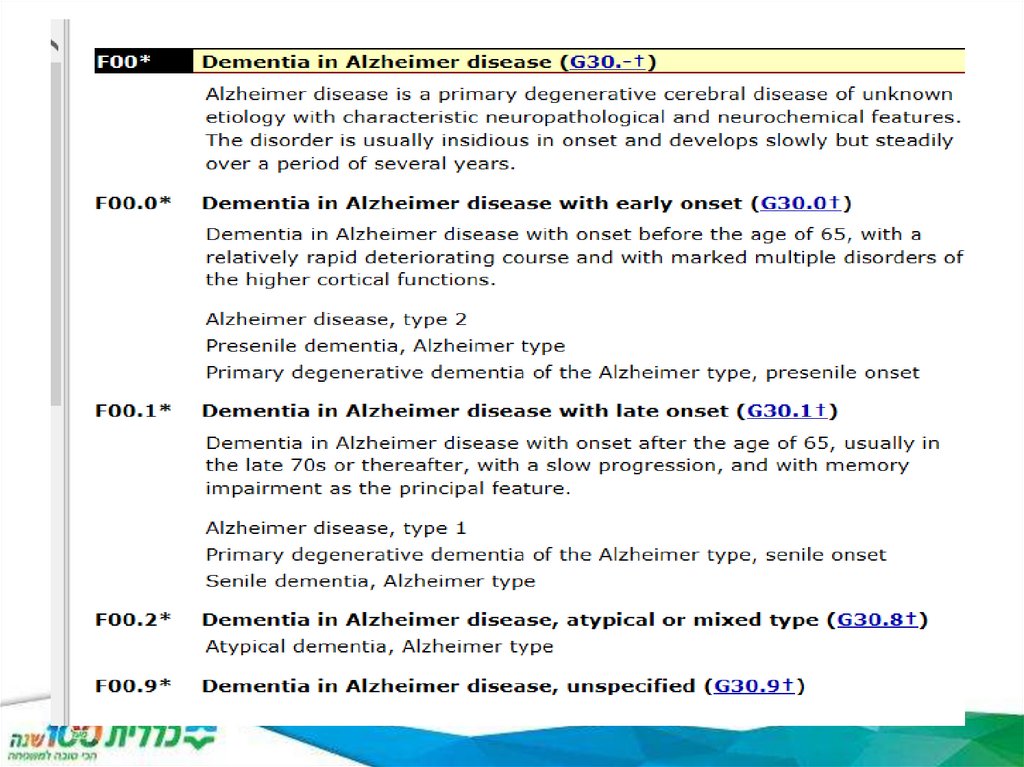
F00-00.9 Dementia in Alzheimer disease
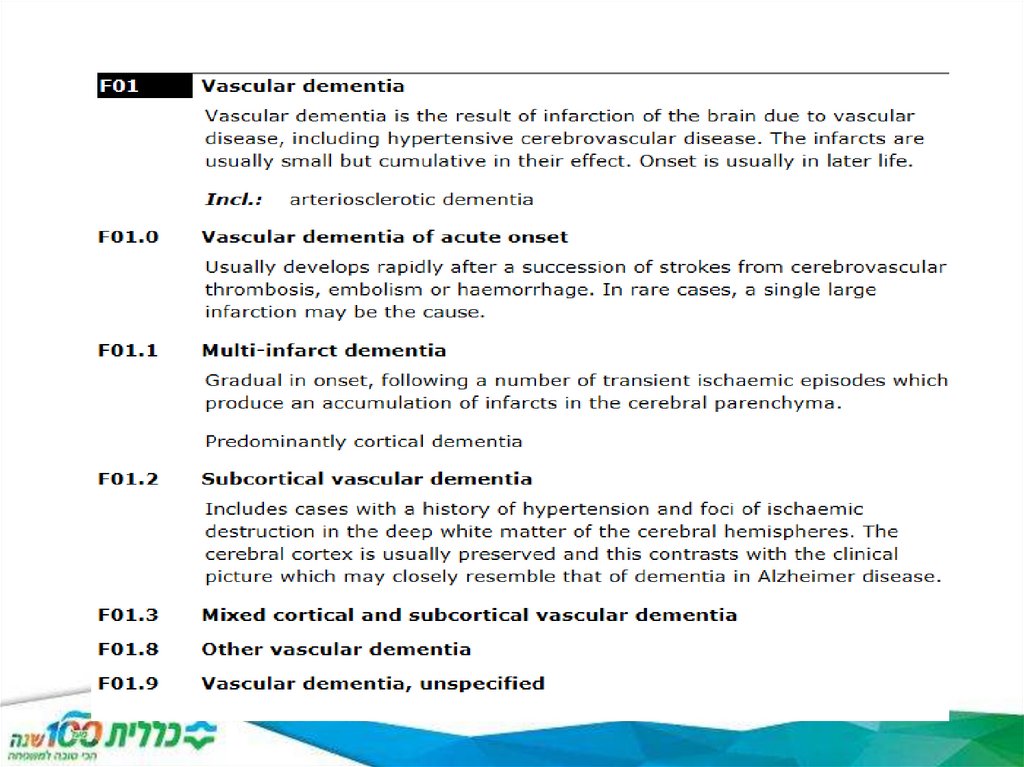
F01-01.9 Vascular Dementia
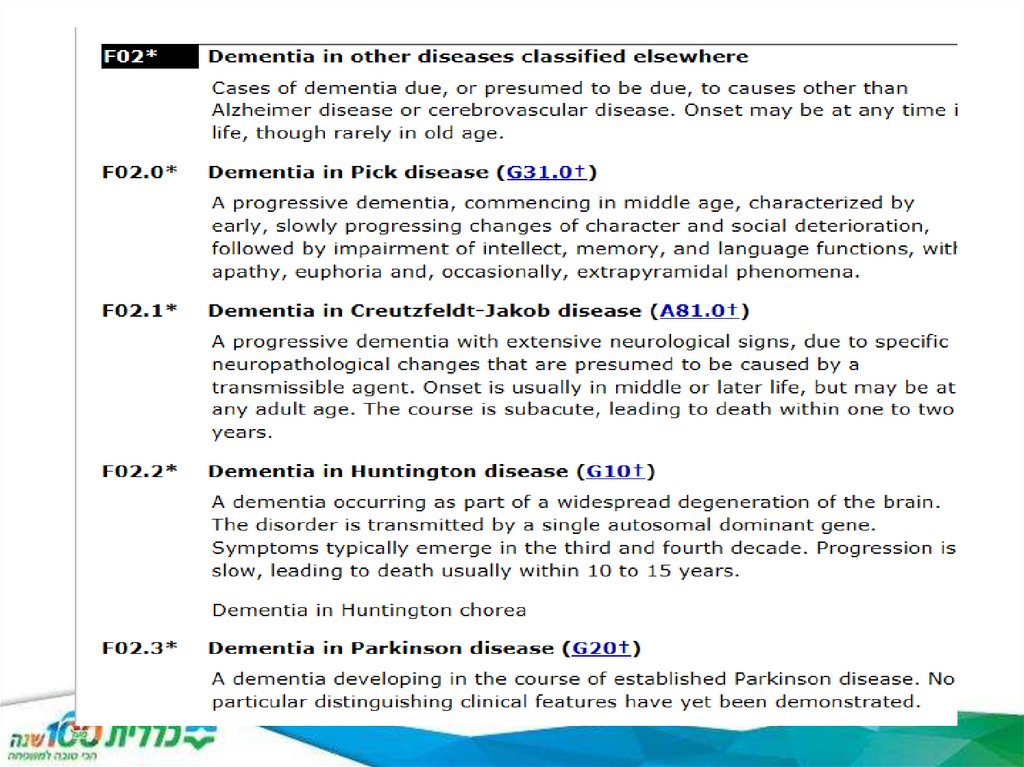
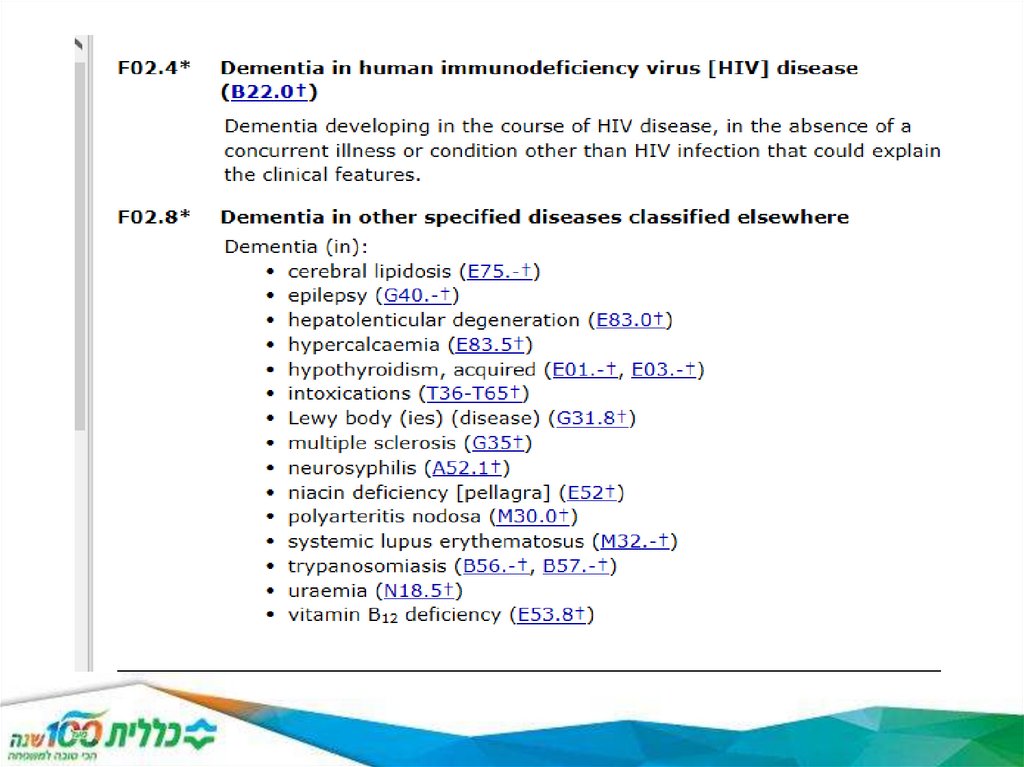
F02-02.9 Dementia in other diseases classified elsewhere
F03 Unspecified dementia
23. Dementia
Example 1: a 90 year old woman diagnosed with multi-infarct dementia after aseries of strokes
This would be coded to F01.1 Multi-infarct dementia. If the dementia had
developed suddenly, for example after a single stroke, it would be coded to
F01.0 Vascular
dementia of acute onset.
Example 2: a 72 year old man diagnosed with senile dementia in Alzheimer’s
disease
This would be coded to:
F00.1* Dementia in Alzheimer's disease with late onset.
24.
25.
26.
27.
28. Organic amnesic syndrome, not induced by F04 alcohol and other psychoactive substances
F04 Organic amnesic syndrome, not induced byalcohol and other psychoactive substances
29.
30.
31.
32.
33.
34.
35.
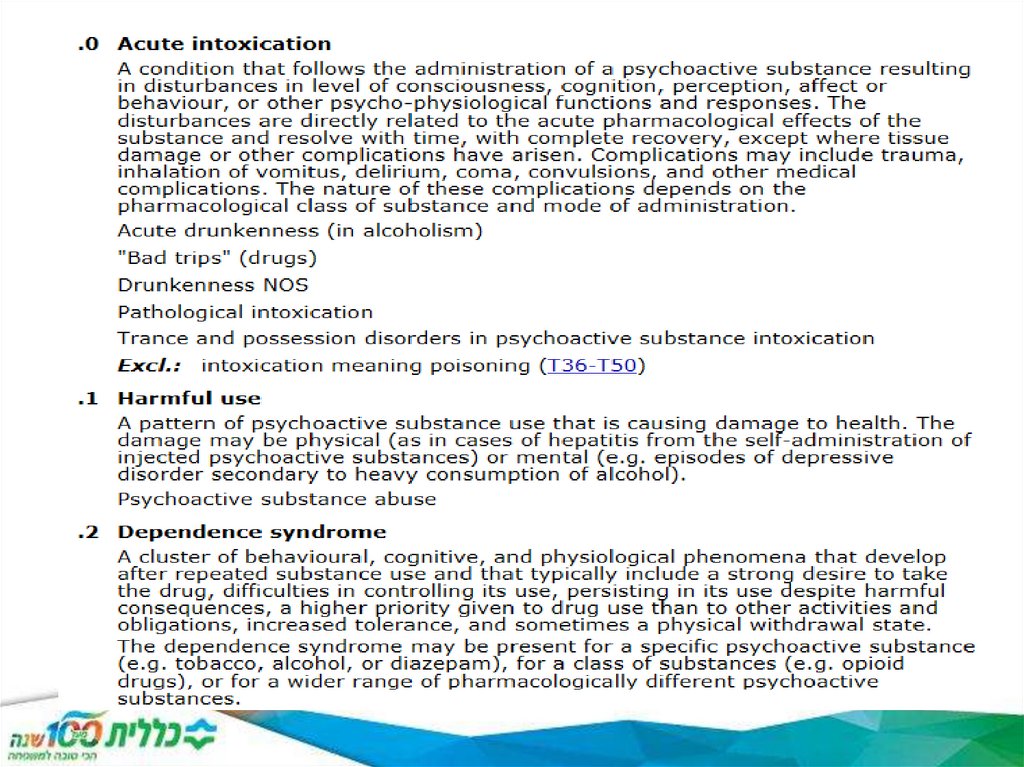
36. F 10-19
F10- AlcoholF 11- Opioids
F12- Cannabinoids
F13- Sedative or hypnotics
F14- Cocaine
F15-Stimulants including caffeine
F16- Hallucinogens
F17-Tobacco
F18-Volatile solvents
F19- Multiple drug use
37.
F20-SchizophreniaF20.0-Paranoid
F20.1-Hebephrenic
F20.2-Catatonic
F20.3-Undifferentiated
F20.4- Post-schizophrenic depression
F20.5- Residual
F20.6-Simple
F20.8-Other
F20.9- Unspecified
38.
39.
40.
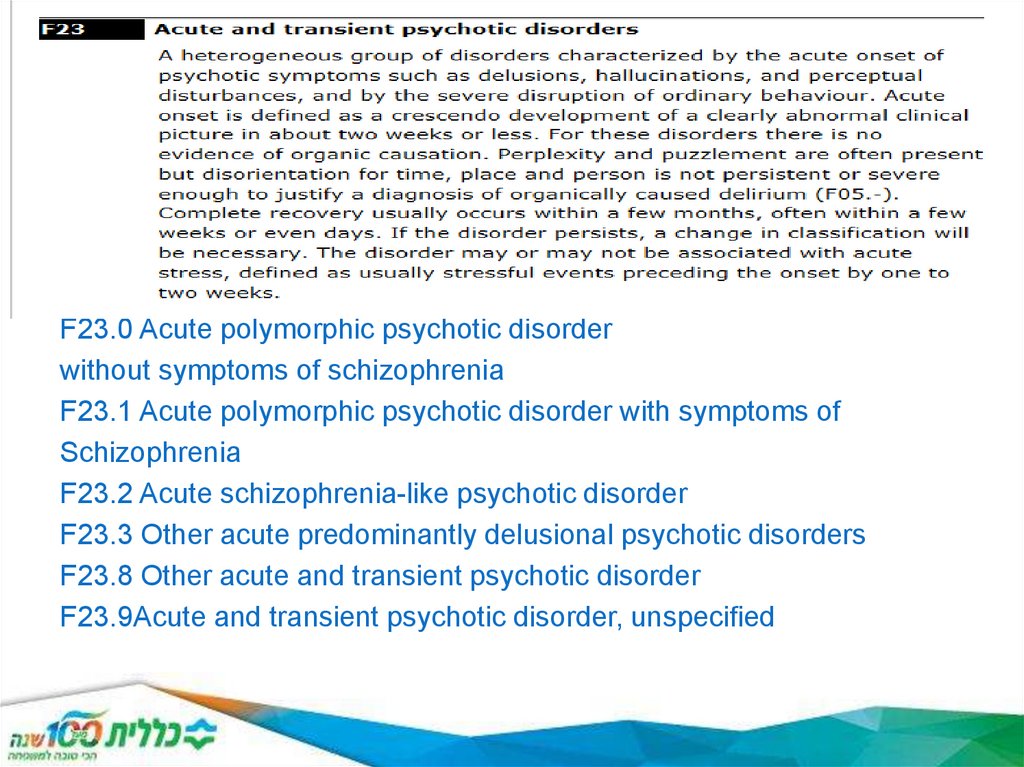
F23.0 Acute polymorphic psychotic disorderwithout symptoms of schizophrenia
F23.1 Acute polymorphic psychotic disorder with symptoms of
Schizophrenia
F23.2 Acute schizophrenia-like psychotic disorder
F23.3 Other acute predominantly delusional psychotic disorders
F23.8 Other acute and transient psychotic disorder
F23.9Acute and transient psychotic disorder, unspecified
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
60.
61.
62.
63.
64.
65.
66.
67.
68.
69.
70.
71.
72.
73.
74.
75.
76.
77.
78.
79.
80.
81.
82.
83.
84.
85. https://www.psychiatry.org/psychiatrists/practice/dsm/history-of-the-dsm https://icd.who.int/browse10/2016/en#/V
https://www.psychiatry.org/psychiatrists/practice/dsm/history-of-the-dsm
https://icd.who.int/browse10/2016/en#/V
86. Культурные аспекты психиатрии
What comes to mind when you think about culture? For a lot of us, we
immediately think of what’s right in front of us: unique languages, different
clothing and diverse food. But a society’s culture also impacts a person’s
beliefs, norms and values. It impacts how you view certain ideas or
behaviors. And in the case of mental health, it can impact whether or not
you seek help, what type of help you seek and what support you have
around you.
According to research published by The Commonwealth Fund, minorities in
the United States are less likely to get mental health treatment or will wait
until symptoms are severe before looking. In fact, only 66 percent of
minority adults have a regular health care provider compared to 80 percent
of white adults. Hispanic and Asian populations report the lowest rates of
having a regular doctor or provider, at 58 percent and 60 percent.
It’s important that we understand the role culture plays in mental health care
so we can support our loved ones and encourage treatment when it’s
needed most.
87. Культурные аспекты психиатрии
Here are four ways culture can impact mental health:
1.Cultural stigma. Every culture has a different way of looking at mental
health. For many, there is growing stigma around mental health, and mental
health challenges are considered a weakness and something to hide. This
can make it harder for those struggling to talk openly and ask for help.
2.Understanding symptoms. Culture can influence how people describe and
feel about their symptoms. It can affect whether someone chooses to
recognize and talk about only physical symptoms, only emotional symptoms
or both.
3.Community Support. Cultural factors can determine how much support
someone gets from their family and community when it comes to mental
health. Because of existing stigma, minorities are sometimes left to find
mental health treatment and support alone.
4.Resources. When looking for mental health treatment, you want to talk to
someone who understands your specific experiences and concerns. It can
sometimes be difficult or time-consuming to find resources and treatment
options that take into account specific cultures factors and needs.
88. Теории развития личности и психопатологии
89. Definitions
PersonalityDistinctive and relatively stable pattern of behaviors,
thoughts, motives, and emotions that characterizes an
individual
Trait
A characteristic of an individual, describing a habitual way
of behaving, thinking, and feeling
shy, outgoing, ambitious, lazy, easy-going, anal, high-strung,
confident, grumpy, happy, friendly, etc
90. Theories of Personality
Sigmund Freud: Founder ofClassic Pcychoanalysis
Psychodinamic Theories
Eric Ericson
Schools Derived from
Psychoanalysis
91. Psychodynamic theories
Explains behavior and personality in terms of unconsciousdynamics within the individual
Emphasizes internal conflicts, attachments, and motivations
• Adult personalities are formed by experiences in early
childhood
•Three variations:
Freud and traditional psychoanalysis
Jungian Theory
Object-Relations School
92. Freud’s Psychoanalysis: The structure of personality
1. Id- Unconscious
2. Ego
- unconscious,
preconscious,
conscious
3. Superego
- unconscious,
preconscious, conscious
93. Freud’s Psychoanalysis: The ID
Operates according to thepleasure principle
–Present from birth
–Primitive
• basic needs and
wants
–2 competing instincts:
• Life (sexual) - libido
• Death (aggressive)
–Unconscious
94. Freud’s Psychoanalysis: The Ego
Operates according to thereality principle
– Arises in first 3 years of life
–Mediates between ID and
Superego
–Rational part of mind
• you can’t always get
what you want
– Floats between all 3 levels of
consciousness
95. Freud’s Psychoanalysis: The Superego
Moral Conscience– Develops around age 5
• At end of Phallic Stage
–Stores and enforces rules
• Inner voice that tells you
not to do something or
that what you did was
wrong
–2 subsystems:
• Ego Ideal = parents
approve/value
• Conscience = parents
disapproval
96. Freud’s Psychoanalysis: Defense mechanisms
1.Repression
2.
Projection
3.
When a feeling or belief that causes anxiety is transformed into the opposite
feeling or belief in our consciousness
Regression
6.
When a person’s emotions are directed towards people or animals that
are not the real object of the emotion
Sublimation: acting out socially unacceptable impulses in a socially
acceptable way
Reaction formation
5.
When repressed feelings are attributed to someone else
Displacement
4.
When a threatening idea, memory, or emotion is blocked (either
consciously or unconsciously) from consciousness
Returning to a previous stage of development
Denial
Refusal to admit something unpleasant or that something that provokes
anxiety is happening
97. Your turn
Your math instructor caught youwith the textbook open during a test.
Despite the fact that you know he
knows you were cheating, you
protest your innocence. This defense
mechanism is:
1. Denial
2. Reaction formation
3. Regression
4. Displacement
98. Personality development: Freud’s Psychosexual Stages
Fixation occurs when the conflicts at a given stagearen’t resolved successfully
Freud’s Psychosexual Stages
1.
Oral (birth – 18 months)
2.
Anal (18 months – 3 years)
3.
Pleasure zone is the genitals
Oedipus complex – development of feelings for opposite sex parent and rivalry
feelings towards same sex parent
–
Boys – fear of castration; Girls – penis envy
Latency (6 – puberty)
5.
Control of eliminating and retaining feces, toilet training issues
Anal retentive – obsession with cleanliness, perfection, control
Anal expulsive – messy, disorganized
Phallic (Oedipal; 3 – 5 or 6 years)
4.
Babies learn about the world with their mouths, oral pleasures
Oral fixation – preoccupation with oral activities as an adult
Sexual urges repressed, play with same sex peers
Genital (puberty on)
Leads to adult sexuality
99. Other psychodynamic approaches
1. Jungian theory2. The Object-Relations School
100. Jungian Theory (aka analytical psychology)
Carl Jung (1875-1961)Divides unconscious into 2 parts:
Personal unconscious: reservoir of personal information and
memories that was once conscious, but has been forgotten or
suppressed and is unique to the individual
Collective unconscious: deepest level of the human psyche that
contains universal memories, symbols, and experiences of all
humans
a reservoir of inherited experiences
Archetype: a generic, idealized model of a person, personality or
behavior
– Innate, universal prototypes
– Appear in myths, stories, art, and dreams
101. Jungian Theory (aka analytical psychology)
•Archetype: a generic, idealized model of a person,personality or behavior
Stereotype, epitome
4 main archetypes:
–
–
–
–
The
The
The
The
Self
Shadow
Anima
Animus
Commonly seen archetypes
– The Child
– The Hero
– The Great Mother
102. Object-Relations School
Melanie Klein & D.W. WinnicottEmphasizes interpersonal relationships and believes the ego-self
exists only in relation to other objects
most important = mother-child relationship
Central problem = balance between need for independence and need
for others
Emphasizes the importance of the infant’s first two years of life and
the baby’s formative relationships, especially with mother
Object: Something to which the subject relates, usually a
person, a part of a person or symbols for these.
External object: an actual person, place, or thing
Internal object: a memory, idea, or fantasy about a person
place or thing
103. Humanistic Approaches to Personality
Humanistic psychologyAn approach that emphasizes personal growth, resilience, and
the achievement of human potential
Humanist psychologists:
1.
Abraham Maslow
2.
Carl Rogers
3.
Rollo May
104. Humanistic Psychology: Abraham Maslow
Personalitydevelopment is a
gradual
progression to
self-actualization
105. Your turn
You are on your way to a restaurant tomeet some friends, and you are hungry.
As you are walking from your car to the
restaurant, you are looking forward to
talking with your friends. Just then, you
hear a gunshot. According to Maslow,
your primary motivation would be
determined by
1. Your hunger
2. Your desire to converse with your friends
3. Your desire for safety
106. Humanistic Psychology: Carl Rogers
Interested in fully functioning individualsCongruence
this is displayed by fully functioning people and is a harmony
between the image they project to others and their true feelings
or wishes
To become fully functioning we need:
Unconditional positive regard
A situation in which the acceptance and love one receives from
significant others is unqualified, no strings attached
Unfortunately many children and adults are treated
with:
Conditional positive regard
A situation in which the acceptance and love one receives from
significant others is contingent upon one’s behavior
107. Erik Erikson's Stages of Psychosocial Development
Erik Erikson's Stages ofPsychosocial Development
• Erik Erikson was an ego
psychologist who developed
one of the most popular and
influential theories of
development. While his theory
was impacted by
psychoanalyst Sigmund
Freud's work, Erikson's theory
centered on psychosocial
development rather than
psychosexual development
• The stages that make up his
theory are as follows
• Stage 1: Trust vs. Mistrust
• Stage 2: Autonomy vs. Shame
and Doubt
• Stage 3: Initiative vs. Guilt
• Stage 4: Industry vs. Inferiority
• Stage 5: Identity vs. Confusion
• Stage 6: Intimacy vs. Isolation
• Stage 7: Generativity vs.
Stagnation
• Stage 8: Integrity vs. Despair
108. Erik Erikson's Stages of Psychosocial Development
Erik Erikson's Stages ofPsychosocial Development
109. The 4 Stages of Cognitive Development Background and Key Concepts of Piaget's Theory
The 4 Stages of Cognitive DevelopmentBackground and Key Concepts of Piaget's Theory
• Jean Piaget's theory of cognitive development suggests
that children move through four different stages of
mental development. His theory focuses not only on
understanding how children acquire knowledge, but also
on understanding the nature of intelligence.1 Piaget's
stages are:
• Sensorimotor stage: birth to 2 years
• Preoperational stage: ages 2 to 7
• Concrete operational stage: ages 7 to 11
• Formal operational stage: ages 12 and up
110. Based on his observations, he concluded that children were not less intelligent than adults, they simply think differently.
AlbertEinstein called Piaget's discovery "so simple only a genius could
have thought of it."
111. Behaviorism
• The theory originates from the works of Ivan Pavlov’s, classicalconditioning, and B. F. Skinner’s, operant conditioning.
Classical Conditioning is when an unconditioned stimulus
and response is manipulated with a conditioned stimulus to create
a conditioned response.
Operant Conditioning is a controlled response with a reward/
punishment system according to the behavior.
• The learner needs reinforcements to keep interest.
Stimuli are effective in controlling behavior.
• As a result, the behaviors can be measured to record learning success.