








 medicine
medicineSimilar presentations:










Blood supply
1.
- weight: 1-1.5 kg largest bodyorgan
represents 1.5-2.5% lean
body mass
- held in place by ligamentous
attachments to diaphragm,
peritoneum, great vessels and
upper GI organs
2.
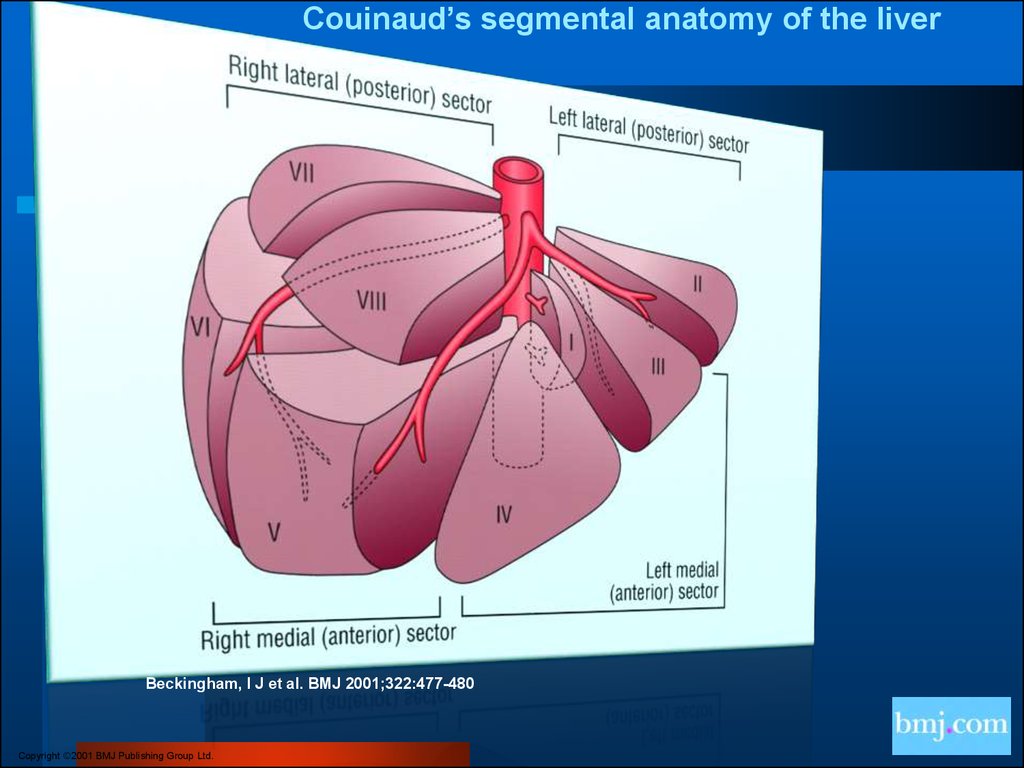
Couinaud’s segmental anatomy of the liverBeckingham, I J et al. BMJ 2001;322:477-480
Copyright ©2001 BMJ Publishing Group Ltd.
3. blood supply
- receives dual blood supply:20% = hepatic artery: oxygenrich
80% = portal vein: nutrient rich
-cell majority (2/3 of liver mass):
hepatocytes
-other cell types: Kupffer cells
stellate (Ito or fat-storing) cells
bile ductular structures
supporting structures
4. Liver Test Patterns in Hepatobiliary Disorders
Type of disorderBilirubin
Aminotransferases
Hemolysis/Gilbert’s
Syndrome
Normal to 5 mg/dl
85% due to indirect
fractions
No bilirubinuria
Normal
Acute Hepatocellular
necrosis (viral and
drug hepatitis ,
hepatotoxins, acute
heart failure)
Both fractions may
be elevated
Peak usually follows
aminotransferase
Bilirubinuria
Elevated, often
> 500 IU
ALT > AST
Chronic hepatocellular
disorders
Both fractions may
be elevated
Bilirubinuria
Elevated, usually
< 300 IU
5.
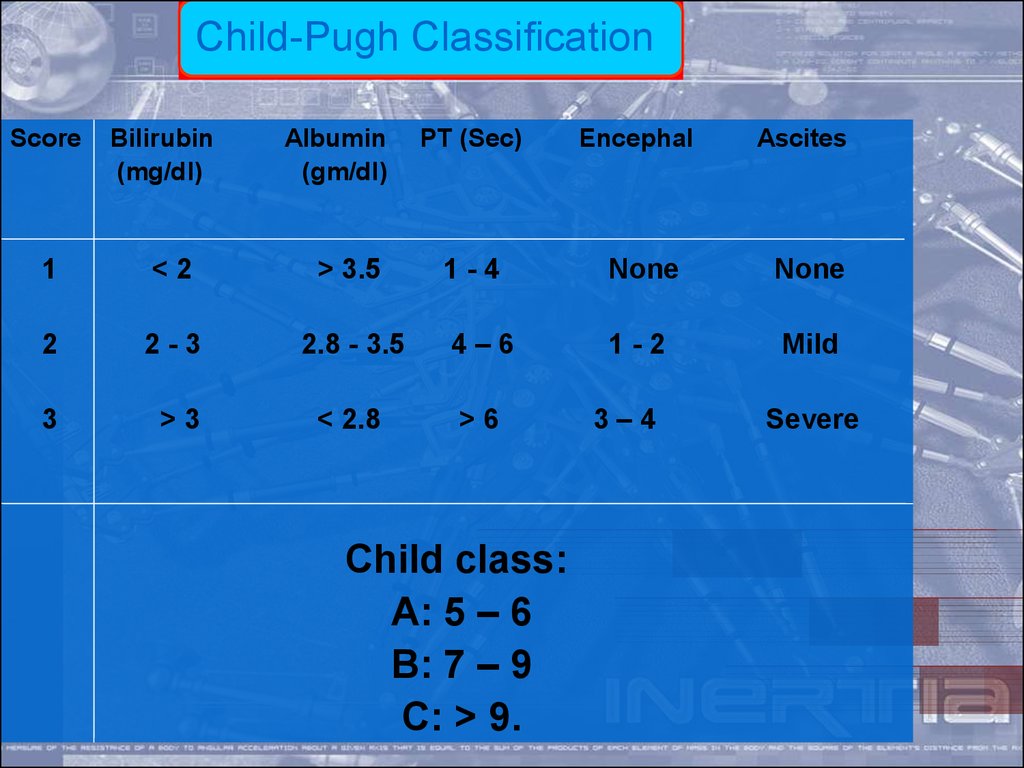
Child-Pugh ClassificationScore
Bilirubin
(mg/dl)
Albumin
(gm/dl)
1
<2
> 3.5
2
2-3
3
>3
PT (Sec)
Encephal
Ascites
1-4
None
None
2.8 - 3.5
4–6
1-2
Mild
< 2.8
>6
Child class:
A: 5 – 6
B: 7 – 9
C: > 9.
3–4
Severe
6. Causes of portal hypertension
SINUSOIDAL•SARCOIDOSIS
•SCHISTOSOMIASIS
•NODULAR REGENERATIVE HYPERPLASIA
•CONGENITAL HEPATIC FIBROSIS
•IDIOPATHIC PORTAL FIBROSIS
•EARLY PRIMARY BILIARY CIRRHOSIS
•CHRONIC ACTIVE HEPATITIS
•MYELOPROLIFERATIVE DISORDER
•GRAFT VS HOST DISEASE
7. CIRRHOSIS
Term was 1st coined by Laennec in 1826Many definitions but common theme is
injury, repair, regeneration and scarring
NOT a localized process; involves entire
liver
Primary histologic features:
1.
2.
3.
4.
Marked fibrosis
Destruction of vascular & biliary elements
Regeneration
Nodule formation
8. Classification of Cirrhosis
WHO divided cirrhosis into 3categories based on morphological
characteristics of the hepatic
nodules
1. Micronodular
2. Macronodular
3. Mixed
9. DIAGNOSIS
Canbe asymptomatic for decades
History
Physical findings: Hepatomegaly,
jaundice, ascites, spider angioma,
splenomegaly, palmar erythema,
fetor hepaticus, purpura etc.
Elevated LFTs, thrombocytopenia,
10.
ManagementOf course the definitive treatment for most of the complications
of end- stage liver disease, including recurrent GI bleeding due
to severe portal hypertension,
orthotopic liver transplantation.
Since the presence of a surgical portacaval or mesocaval
shunt greatly complicates the transplantation procedure, we
have generally abandoned these types of shunting operations
in patients with cirrhosis.
11. SURGERY
1- LIVER TRANSPLANTATION• ONLY DEFINITIVE PROCEDURE
# primary in Child’s C
2- SHUNT PROCEDURE
3- DEVASCULARIZATION
12. Devascularization
Sugiura proceduremortality is 10-35%
5% recurrence rate of rebleeding
thoraco & abdominal incision
splenectomy, devasc. Stomach, esopsophagus, transect the
esoph with reanastamosis, ligate all collaterals