

")











 labor")
 period of life")



























 prevention")



 medicine
medicineSimilar presentations:










Background of the lecture
1. Background of the lecture
• Propedutics pediatrics(Basic clinical pediatrics). Introduction
• Childhood Periods
Intrauterinal (embrional, fetal)
Extrauterinal
• Labor, pediatric aspects
• Newborns. First examination, CNS
estimation. Common transitory states,
Neonatal primary care
2.
I am a toddler!Я вас приветствую!
You are Welcome
3. Propedutics pediatrics (Basic clinical pediatrics)
4.
The Place of pediatrics as a science aboutwell and sick child
anthropology
Childhood
medicine
5. The Child is not reduced copy of adult person!
6. Study areas of the propedeutics of pediatrics
• The physical, psychic and social developmentalestimations in children.
• The anatomical and physiological particularities
of internal organs and their systems in children
according the age. The Methods of the clinical
study. The Semiotics the most important
symptoms and syndroms in pediatrics.
• Nursing (feeding) and common looking after
• Emergency care in typical situations
7.
The Practical physician in everyday work has to bealongside with a study of the individual child
particularities, it is important to work out the
differential approaches to children depending on
their age. Though the early growing and
development it is a permanent process. Each child
passes determined stages or periods of the growth.
8.
Childhood Periods9.
From the moment of the baby conception till adultcondition achievement it is necessary to select two
the most important stages of individual life:
intrauterinal and extrauterinal.
10.
Intrauterinal period of the humandevelopment
The embrional period begins with the 1-st day after
conception and lasts 9 weeks of the pregnancy. In this
time the main organogenesis, amnion and chorion are
forming.
The fetogenesis begins since 9 weeks and ends
approximately on 40-th week of the full pregnancy. In this
period the differentiation and maturation of the body organ
systems happen following by development, maturation and
aging of placenta.
11.
The child born at 22 - 38 weeks of pregnancy andshown signs of life has to be estimated as a
premature.
Children been born after 42 weeks of pregnancy and
later must be classified as a postterms.
12.
During the first 16 weeks of pregnancy the fetal growing anddevelopment goes only to account of the increase of cellular
mass (hyperplasia).
Within the following 16 weeks, (since 17 till 32 weeks of
gestation) the rate of cellular multiplication begins gradually
to decrease. At this time gradually the processes of the
cellular size increasing take power. It is so called combined
hyperplasia and hypertrophy phase of the intrauterinal
development.
Within 7 weeks of gestation (since 33 till 40 weeks of
pregnancy) in fetal development the cellular hypertrophy
dominates setting fetal growth (fetal cellular hypertrophy
phase). As a rule the fetus accumulates subcutaneous fat in
consequence of the adipocytes hypertrophy.
13. Critical periods of intrauterinal development.
• Forming of organs (organogenesis) in embryogenesistakes place unevenly, in the certain terms for every system
of organs. Critical periods appear at the moment of stormy
differentiation and growth of organ's weight. It creates
preconditions for the damage. For example, the virus gets
into the blood stream of embryo. Due to their biological
feature to create the best preconditions for reproduction
the viral bodies will be directed into the most intensively
proliferating tissue. Thus this tissues will be damaged
firstly and congenital disease starts. There is a rule: as
sooner an unfavorable factor for a fetus begins acting as
the severity of the teratosis incriases. A fetus can have
almost all defects of organs and systems. Gathering the
history of pregnancy you have to pay attention to a
possibilities of harmful environmental factors.
14. Critical periods of intrauterinal development.
• Now it is agreed to select the critical periods ofpregnancy when the embryo or fetus is especialy
sensitive to disadvantage influences into several
periods.
• The First critical period is a time of the fertilized
egg into the womb implantation. Its mistakes lead
the embrio to death and spontaneous abortion.
• The Second critical period can happen in time of
placenta development, begins at 3-st week of
pregnancy and lasts till 11-12 weeks of pregnancy.
• The Third critical period corresponds to the time of
internal organs systemogenesis. For all organs the
proper sensitive periods exist. Some times the
organogenesis does not finish with delivery and
continues within the early childhood.
15. Perinatal pediod of development includes the time since 22 weeks of pregnancy till the day of delivery and also next 7 days of life
The neonatal and infantile mortality rates is closely connected with thehappening perinatal abnormalities.
16.
Labor in focus.Pediatric point of view.
х
17.
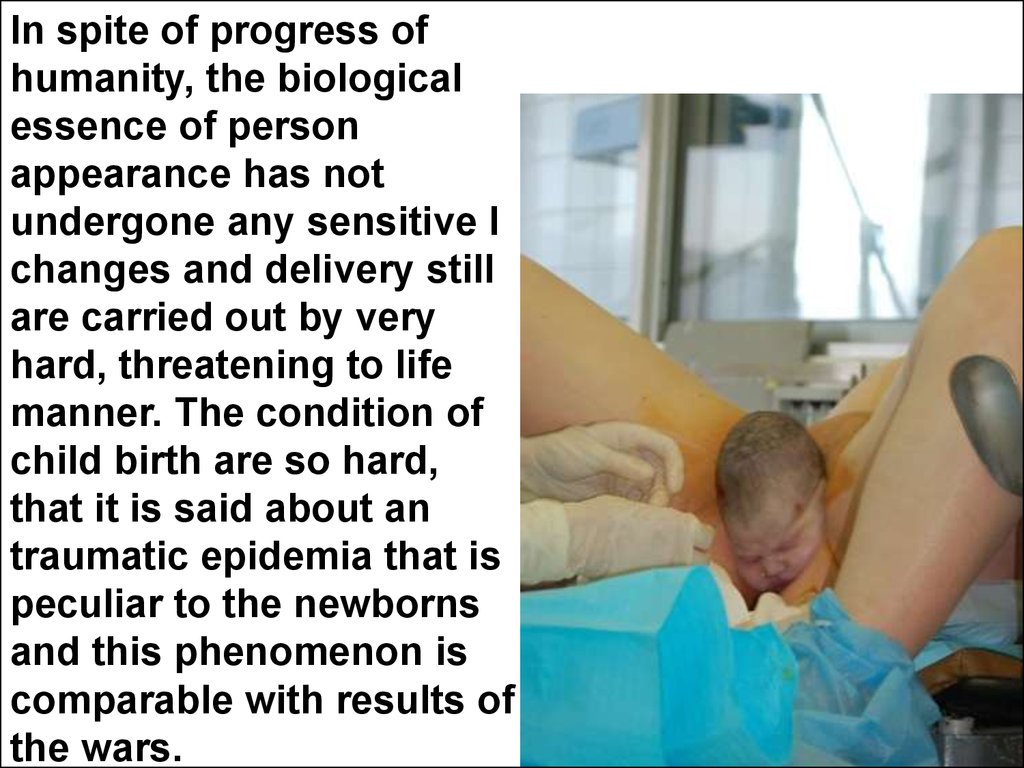
In spite of progress ofhumanity, the biological
essence of person
appearance has not
undergone any sensitive l
changes and delivery still
are carried out by very
hard, threatening to life
manner. The condition of
child birth are so hard,
that it is said about an
traumatic epidemia that is
peculiar to the newborns
and this phenomenon is
comparable with results of
the wars.
18.
The neonatal death due to intracranial hemorrhage19. Abdominal (caecarian) labor
20. Extrauterinal (postnatal) period of life
Extrauterinal (postnatal)
period of life
Labor
Neonatal (newborn, till 28 days)
Infants (1 – 12 mo)
Toddlers (1 – 3 yr)
Preschoolers (3 -7 yr)
Early school children (7 – 12 yr)
Late schoolers (12 – 18 yr)
Teens (10 – 18 yr)
21.
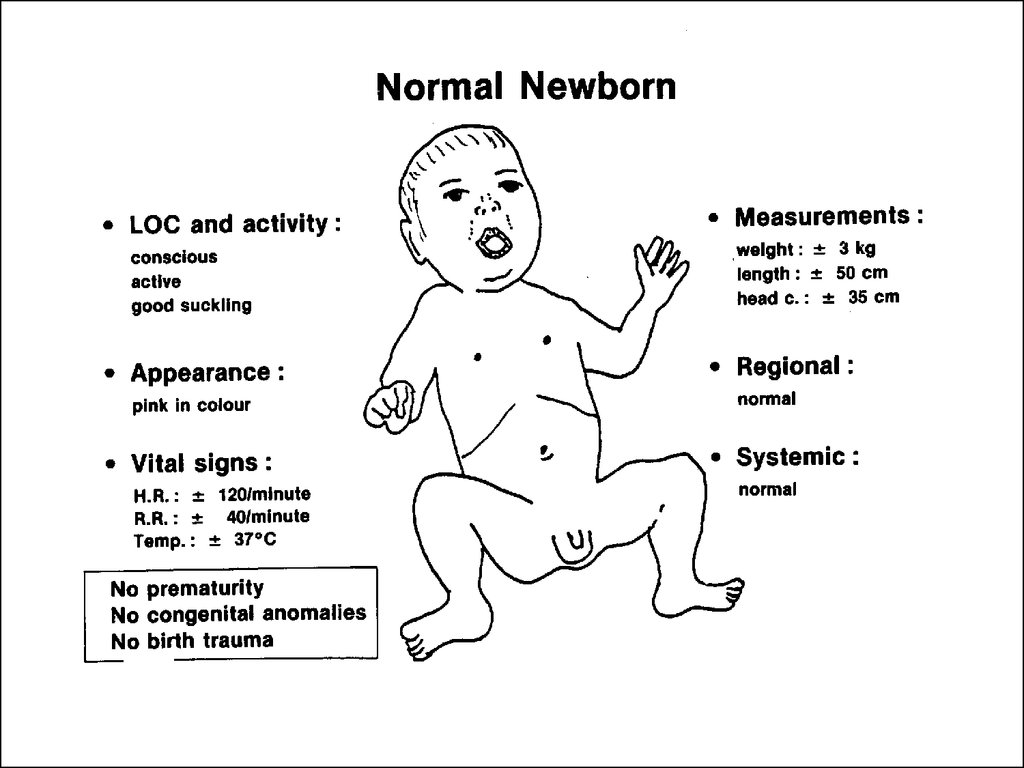
Newborn22. First examination of the newborn.
• All children are examined using the Apgar score(pediatrician Virginia Apgar score) in 1st and 5th
minute after the labor. Examination using Аpgar
score is based on the sum of points (grades) that are
given for five groups of symptoms. They are color of
the skin, breathing, heart rate, muscular tonus,
intensity of child irritation to unpleasant stimulus.
According to the assessment of their
intensity appearance they are given 0, 1 or 2 points
agreeably. Healthy new-born usually demonstrates 8
- 10 points in the first minute of his life and has 9 - 10
points by the Apgar score fifth minutes later.
23.
Prof. V. Apgar (1903 – 1967)24.
Apgar`s Score – the 1-st and 5-th min of lifeSigns
Points
0
1
2
Heart rate
0
<100/min
>100/min
Respiration
None
Weak cry
Vigorous cry
Muscle tone
None
Reflex
irritability
None
Some
motion
Cry,
withdrawal
Color of body
Blue
Pink body,
blue extremities
Pink all over
Some extremity Arms, legs well
flexion
flexed
25. Neonatal Asphyxia
• Quick estimation using Аpgar score ables todiagnose one of the most dangerous condition in
neonatal practice - asphyxia.
Asphyxia is an absence of natural breathing.
The respiratory deficiency in asphyxia can be seen
in the presence of heartbeats and must be revealed
immediately after the labor. The development of
asphyxia as a rule is a result of antenatal deep
hypoxia which damages a breathing regulatory
center and can be a result of the premature placenta
detachment, umbilical cord rupture or its
compression because of the tight knot etc.
26. Apgar score and asphyxia
• 7 – 6 points – mild asphyxia• 5 - 4 – moderated
• 3 - 1 – severe, life threatening
In asphyxic children with low index of Аpgar
score on 1-th and 5-th minutes and
especially after 2 hours of treatment it is
necessary to expect the development of
severe neurological disease like cerebral
palsy.
27.
28.
29. Preterm babies
• There are 4 degrees of prematurity according to theterms of antenatal development and weight of body:
• 1st degree of prematurity is the most prognostic
well. It is characterized by the term of antenatal
development less than 34-38 weeks and by the
weight of body from 2000 to 2500 grams.
• 2nd degree - 32 - 34 weeks, mass from 1500 to 2000
grams.
• 3rd degree - 30 - 32 weeks, mass from 1000 to 1500
grams.
• 4th degree is the most severe premature state with
extremely low weight. The term of antenatal
development lasts less than 30 weeks. The weight
corresponds to 1 kg and less.
30.
Twins31. Fetal immaturity
• If a child been born in term or nearly in termcorrespondes to expectant body weight but
has morphological and functional features of
preterm newborn, this condition should be
considered as an immaturity. For inmature
children especially are typical of the low
muscle tone and weak sucking. Many
mother`s condition make fetuses prone to
inmaturity especially renal, heart end
endocrinal diseases as well as the young
mother`s age.
32.
33.
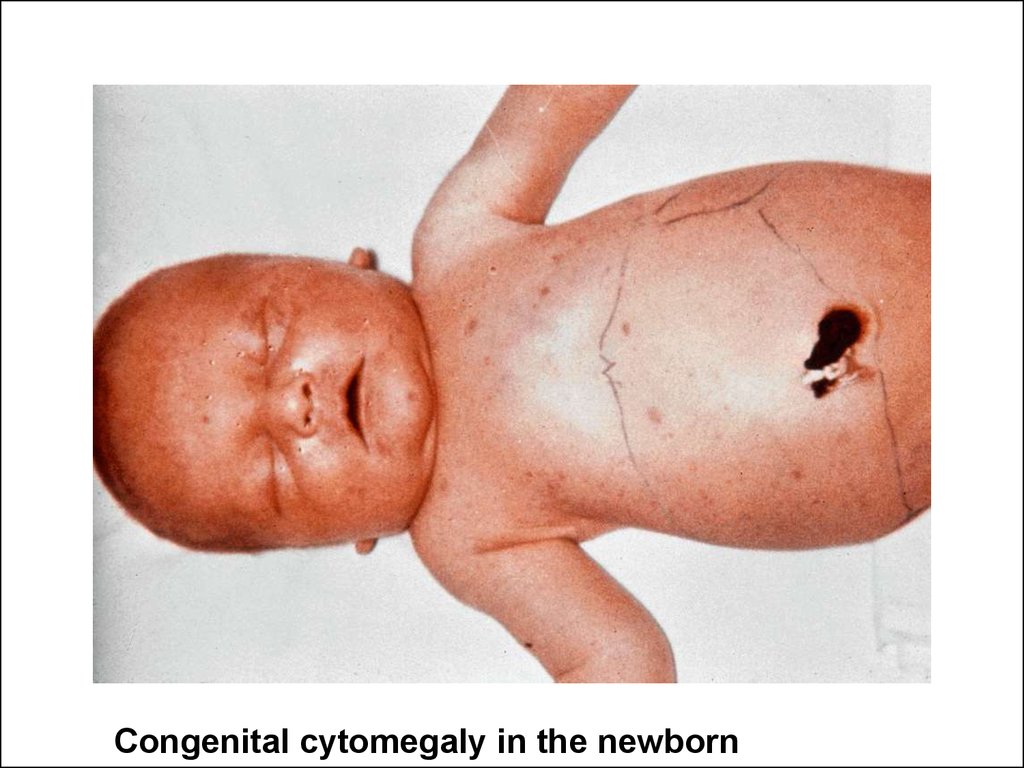
Congenital cytomegaly in the newborn34.
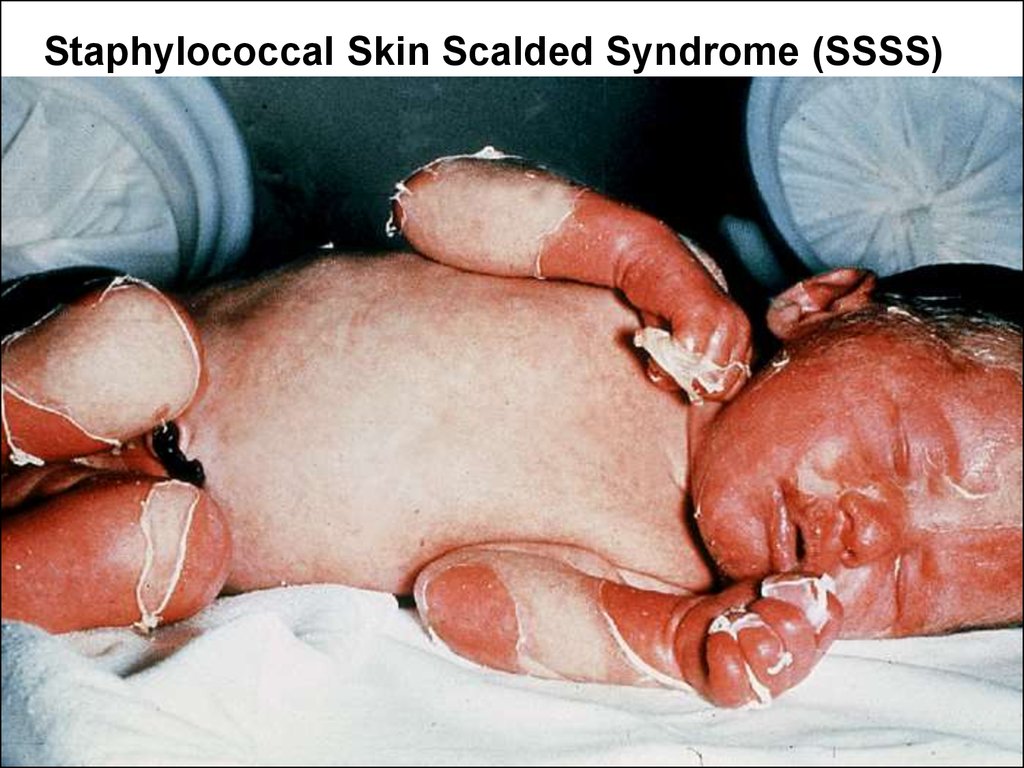
Staphylococcal Skin Scalded Syndrome (SSSS)35.
Twins XX,47(21+) andХХ,46
36.
Cleft lip37.
The CNS condition ofnewborn is the prime
estimation criterion for
determination of the fetus
maturity and for prognosis
of his life.
38.
• The deep long sleeping is common in newborn and lastsusually 18 – 22 h per day. Within the sleeping the children
hold “conscious appearance”. After awake the most
children scream from hungry requiring the mother`s
breast. At this moment a plenty of spontaneous motions is
a typical style of the behavior in full-term, mature and
healthy children. The relative flexors hypertonia is also
common property of the skeletal muscles state. The
manifestation of flexors hypertone perhaps is the
consequence of newborn's trying to save so-called "pose
of embryo" after the birth. The presence of primitive
neonatal reflexes is also necessary for full-term, mature
healthy child. These reflex arches are closed on different
levels of spinal cord and brainstem. The neonatal reflexes
as a rule persist in infants within the first months. The
follow up to their appearance and disappearance can give
important information about CNS development.
39.
CNS.Neonetal responses
(Newborn's Reflexes )
40.
Oral responses.Suckling – it is the most important reflex in small children. Its
absence in newborns means severe condition. The response
fades in children aged approximately 1 yr.
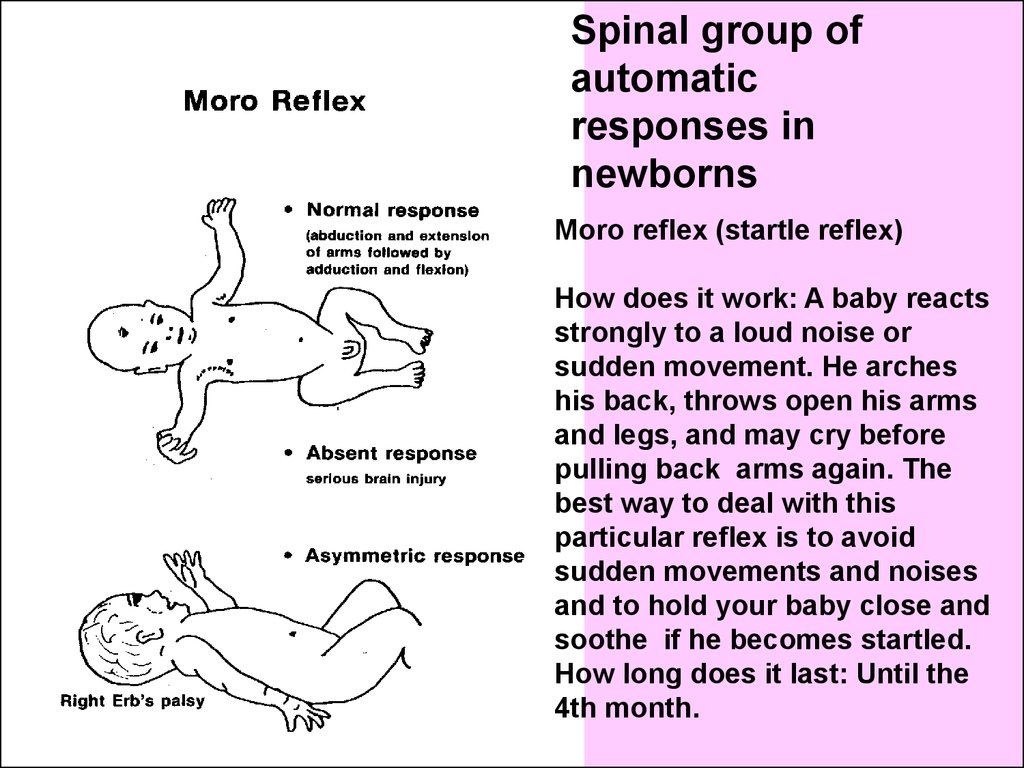
41.
Spinal group ofautomatic
responses in
newborns
Moro reflex (startle reflex)
How does it work: A baby reacts
strongly to a loud noise or
sudden movement. He arches
his back, throws open his arms
and legs, and may cry before
pulling back arms again. The
best way to deal with this
particular reflex is to avoid
sudden movements and noises
and to hold your baby close and
soothe if he becomes startled.
How long does it last: Until the
4th month.
42.
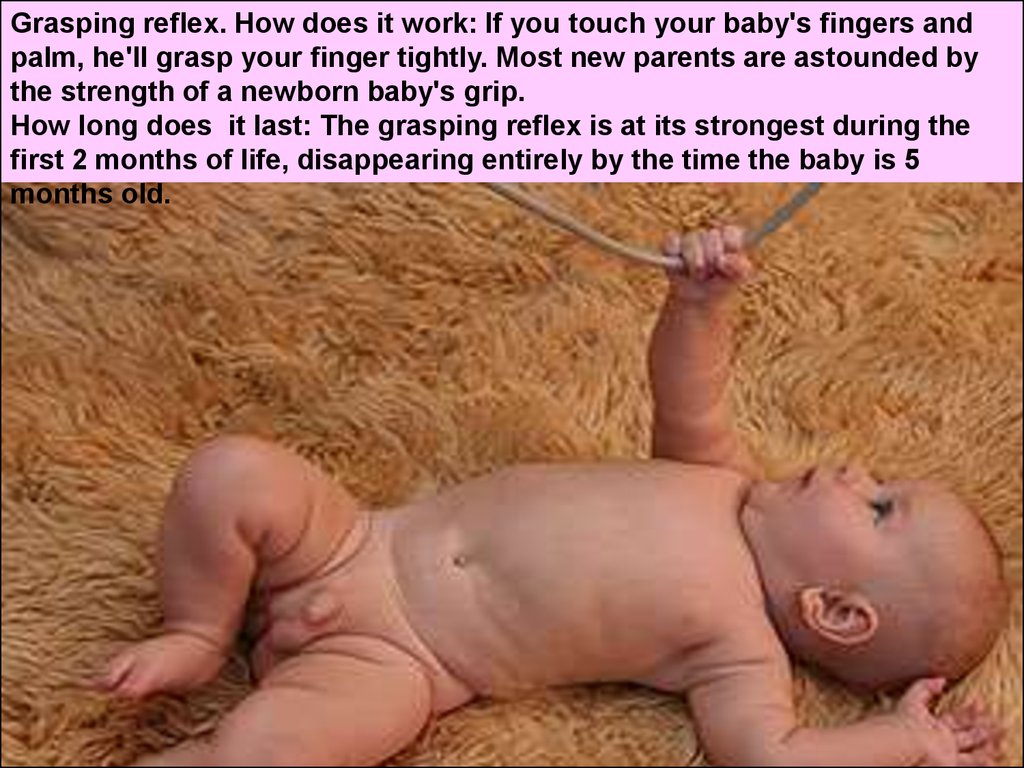
Grasping reflex. How does it work: If you touch your baby's fingers andpalm, he'll grasp your finger tightly. Most new parents are astounded by
the strength of a newborn baby's grip.
How long does it last: The grasping reflex is at its strongest during the
first 2 months of life, disappearing entirely by the time the baby is 5
months old.
43.
Grasping reflex from the soles44.
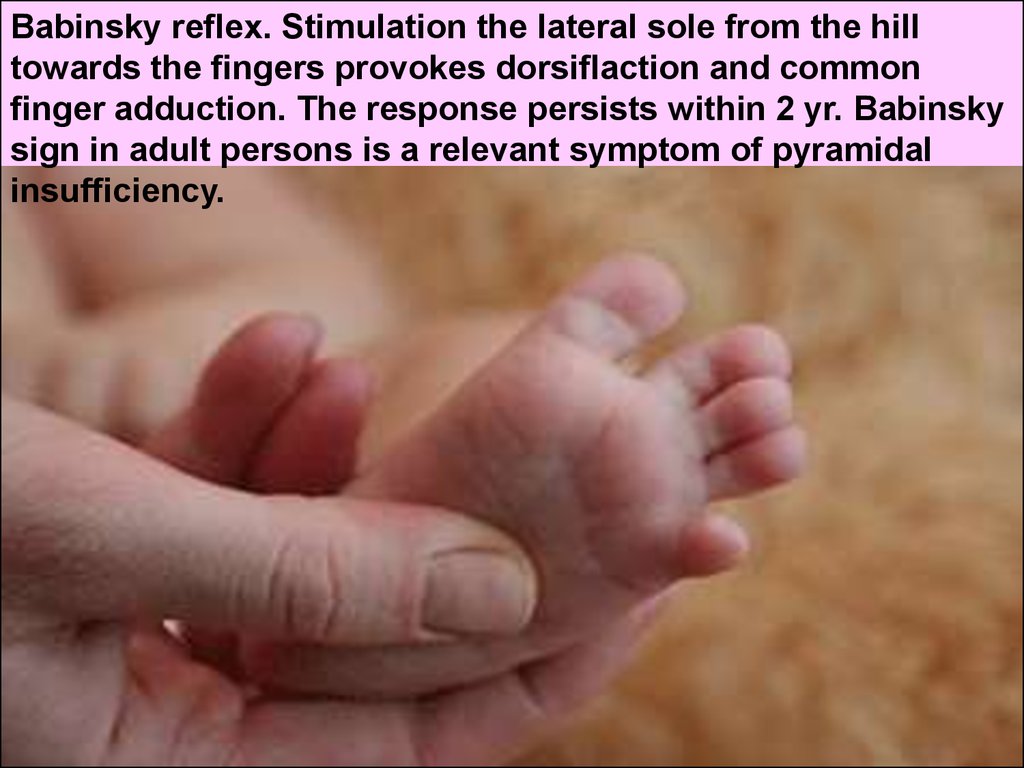
Babinsky reflex. Stimulation the lateral sole from the hilltowards the fingers provokes dorsiflaction and common
finger adduction. The response persists within 2 yr. Babinsky
sign in adult persons is a relevant symptom of pyramidal
insufficiency.
45.
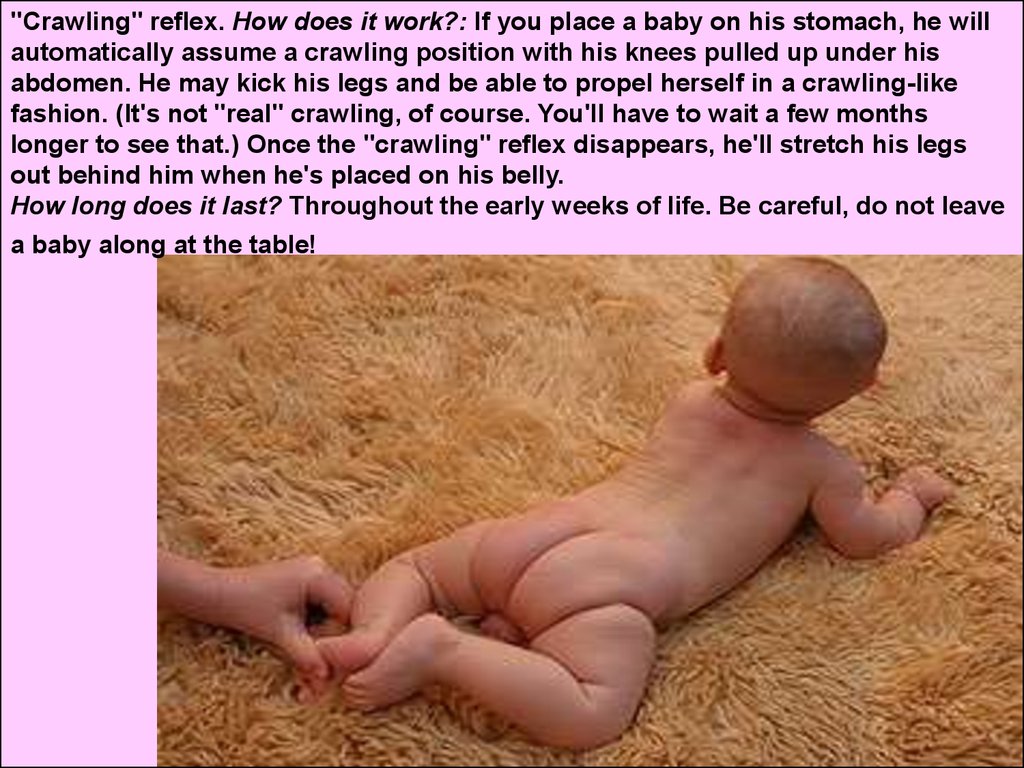
"Crawling" reflex. How does it work?: If you place a baby on his stomach, he willautomatically assume a crawling position with his knees pulled up under his
abdomen. He may kick his legs and be able to propel herself in a crawling-like
fashion. (It's not "real" crawling, of course. You'll have to wait a few months
longer to see that.) Once the "crawling" reflex disappears, he'll stretch his legs
out behind him when he's placed on his belly.
How long does it last? Throughout the early weeks of life. Be careful, do not leave
a baby along at the table!
46.
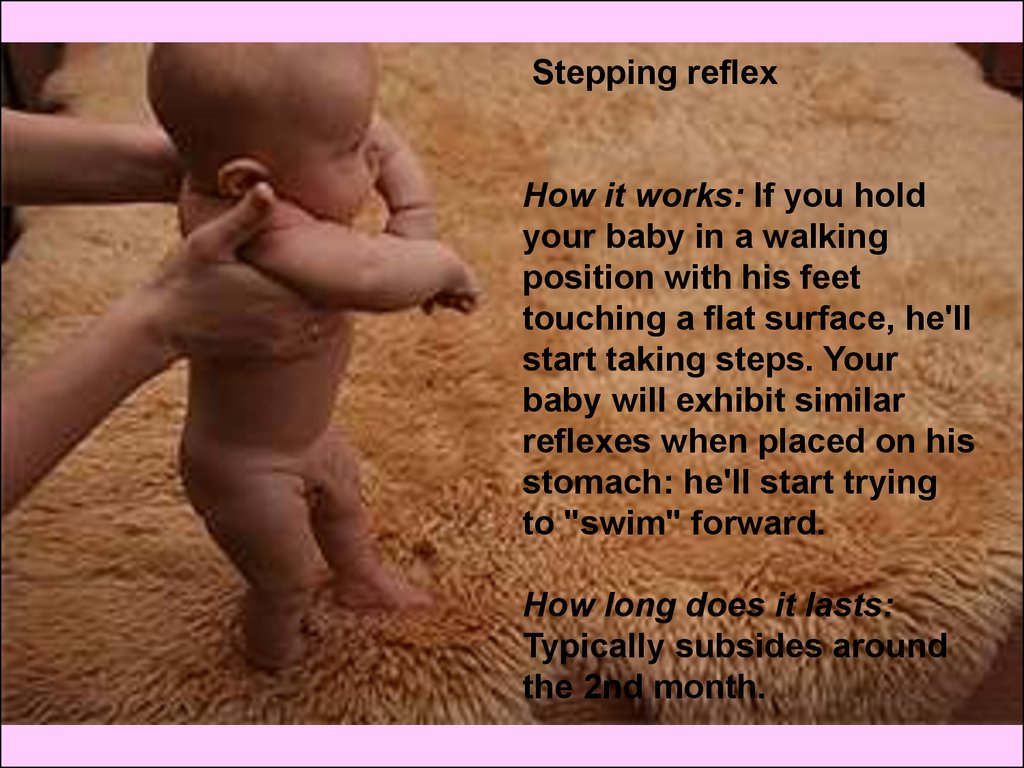
Stepping reflexHow it works: If you hold
your baby in a walking
position with his feet
touching a flat surface, he'll
start taking steps. Your
baby will exhibit similar
reflexes when placed on his
stomach: he'll start trying
to "swim" forward.
How long does it lasts:
Typically subsides around
the 2nd month.
47. Postural reflexes
Tonic neck reflex (fencer's reflex)How it works: If a baby is placed on her back, she will turn
her head to one side and extend the arm and leg on that same
side in a classic fencing position. She'll then turn her head in
the opposite direction and extend her other arm and leg in
turn.
How long it lasts: About 6 months.
48.
Transitory states in neonatalperiod are reflecting their early
adaptation to the extrauterinal life
and can be missed with pathologic
states.
49. The syndrom just right now been born baby
• It is featured by brief child inability to moveand short apnea. Deep inspiration and
scream follow after that. During the following
5-6 minutes a child is getting active with
typical mydriatic pupils in spite of the bright
light in delivery room. This condition appears
due to reaction on catecholamins surplus
production getting into the child's blood.
Also the primary reaction of cerebral cortex
for the new tactile, gravity, temperature
stimuluses can explicate the condition.
50. Transitory hyperventilation, gasps, apnoe.
• The child after labor should catch first breath-in getting theareas of lungs which are still being in pulmonary collapse
to inflate up. Expiration efforts followed by the first
neonatal scream also is very useful in this situation to fight
pulmonary collapse. Some children develop the so-called
gasps-breathing. Gasp is the sort of exaggerated deep
breathing with prolonged expiration. During the gasp
breathing the CO 2 level is getting low. That's why often
the children have short periods of breathing absents
(apnoes) till to 5 sec. long (irregular breathing). Transitory
hyperventilation in newborns is completely self limited
condition and does not need any treatment.
The cases of long gasping and apneas lasted more 20
sec., accompanied by cyanosis (pathological apnea) are
peculiar to the children with intracranial hemorrhages or
pulmonary diseases.
51. Common transitory neonatal states.
• Physiological (primary) body weight losshappens on 3-4 day of life, riches 4 -10%
calculating on initial mass and restores
approximately at day 7 – 10 .
• Physiological skin redness
• Physiological intestinal disfunction
• Uric acid crystalluria
52. Physiological jaundice in newborns
It appears at day 3 of life or
little bit later and looks like
intensive yellow coloration of
the skin. At this time the level of
bilirubin riches 100 - 140 mmol/l
of blood serum. Jaundice
disappears spontaneously in 10
- 14 days.
In any case the physiologic
(benign) jaundice should be
distinguished from the neonatal
hemolytic disease which can be
life threatening condition in
affected baby.
53.
So-called sexual crisis in newborns ormastopathy belongs to the most
amazing physiological states in
newborns. The fact is that 75% of babies
have sexual crisis and more often in
girls. It's characterized by:
a) Transitory mastopathy (enlargement
of breasts) in newborn usually
symmetric. It appears on 3-4 day and is
being evident for 1-1,5 months. The
outflow of milk (so-called "milk of
witches") from this breasts is not rare.
b) The girls quite often have
desquamative vulvovaginitis or
neonatal menses. It is featured by
appearance of bloody excretions from
vagina. As a rule not more then 1-2 ml of
blood can be excreted. Does not require
treatment, but requires a close hygienic
care.
54.
It is not allowed tosqueeze out the milk,
because there is the
danger of microbial
contamination and
local infection`s
development. Like
other benign neonatal
states it need only
observation.
Neonatal mastitis
55.
Toxic neonatal erythema56.
Neonatal primarycare
As a rule in 90% of all
newborns the labors take
place without the
necessity of a doctor`s
close intervention.
But prime
measures of care are
executed in all cases.
57. Suction of the mucus and fluids from oral and nasal cavities.
This easy procedure prevents anaspiration of fluids and secretions
during the first breath-in (after the
appearance of fetus head) and should
be done in any case before the
umbilical cord cut.
58.
Neonatal primarycare
Clamping and
cut of the
umbilical cord
59. Clamping and cut of the umbilical cord.
• The terms of clamping of the umbilical cord can be:• a) ordinary or traditional in 1,5 - 2 minutes after the labor in healthy fullterm children, usually after the first inspiration and in 1 - 1,5 minutes
after in children who has been born prematurely. In case of the late
umbilical cord clamping, especially when a newborn is disposed below
the cavity of uterus there is the danger of additional placental-fetal
hemotransfusion. The surplus volume of blood gets to the fetus.
Clinically it can be evident by blood concentration and its high
viscosity, by total skin dark blue-red appearance (cyanosis), because
of the heightened load on the pumping ability of heart. A physiological
jaundice proceeds in children considerably longer.
• b) Clamping of the umbilical cord after stopping of its pulsation in
children which were born by cesarean section should be done into
the practice in more late terms;
• c) an umbilical cord cut should be put into the practice in early terms
after the birth in condition of very low body weight, in women with
fever and in condition when the hemolytic diseases is expected.
• In such situation the early umbilical cord cut prevents the penetration
of mother's pathogens to the child after the labor and relieves severity
of hemolytic or infectious diseases of newborns.
60. The Humid newborn is quickly coolling!
The separated from the mother newbornhas to be placed on a sterile and heated
diaper. The amniotic fluids must be
removed gently from the skin. The moist
diaper should be changed. After the child
is set on the mother chest and covered
with blanket. The identification bracelets
on the hands and legs showing the exact
time of delivery, baby sex and mother`s
name must be put.
To warm up!
61. Gonoblenorrhea (gonococcal conjunctivitis) prevention
It is established by the antisepticsolution or ointment (for instance,
sodium sulphacyl 20% in water)
instillation from the individual dropper
into the conjunctival bag twice:
immediately after the delivery and 2 h
later. The same procedure must be
done in girls for external genitalia.
62.
Unfulfilled preventive maintenance of Gonoblenorrhea(gonococcal conjunctivitis)
The Newborn child was born at home without rendering medical help. On
5 day after birth at checkup the child demonstrates severe eyelids
edema, brightly red conjunctiva and abundant purulent discharge from
the eyes.
63. We Congratulate you. The first lecture on pediatrics is over! Apropos…
• отработки лекций и индивидуальныеконсультации производятся на
второй академической неделе с 15 до
17.30 по понедельникам в кабинете
зав. кафедрой д.м.н., проф. Иванько
Олегом Григорьевичем.
64. Consolidation
Haw long does the human gestation last?
A. 40 min
B. 40 h
C. 40 days
D. 40 weeks
E. 4 mo
The most important hereditary response in
newborns is:
A. Crying
B. Crawling
C. Cramping
D. Suckling
E. Sleeping