




























")































 medicine
medicineSimilar presentations:









 clinical trial programme in patients with haemophilia A")
Diagnosis and management of VUR after first UTI
1. Diagnosis and Management of VUR after first UTI
2. Case
• 2.5 year old old white girl with 3 days of:–
–
–
–
Fever (Tmax = 40°C)
Poor appetite
Fussiness
2 loose stools a day
Urine dip shows moderate leukocyte esterase
Treatment with PO TMP/SMZ initiated
Urine culture (cath specimen) grows >105 E. coli
Child defervesces in 2 days and completely well in 3
days.
• Next steps?
3. Screening for VUR
• Infants and children 2 months to 2 years with initialUTI should have either a VCUG or RNC performed to
detect the presence and severity of VUR. (Strength of
evidence: fair)
(AAP, Practice Parameter: The Diagnosis, Treatment, and Evaluation
of the Initial UTI in Febrile Infants and Young Children, Pediatrics,
103:4; 843-852, 1999)
4. Screening for VUR
• Infants and children 2 months to 2 years with initialUTI should have either a VCUG or RNC performed
to detect the presence and severity of VUR. (Strength
of evidence: fair)
(AAP, Practice Parameter: The Diagnosis, Treatment, and Evaluation
of the Initial UTI in Febrile Infants and Young Children, Pediatrics,
103:4; 843-852, 1999)
5. Age at First UTI
0 - 2 years39%
2 - 6 years
61%
Conway, P. H. et al. JAMA 2007;298:179-186.
6. Screening for VUR
• Infants and children 2 months to 2 years with initialUTI should have either a VCUG or RNC performed
to detect the presence and severity of VUR. (Strength
of evidence: fair)
(AAP, Practice Parameter: The Diagnosis, Treatment, and Evaluation
of the Initial UTI in Febrile Infants and Young Children, Pediatrics,
103:4; 843-852, 1999)
No recommendations on
how to manage VUR
7. Management of VUR
Scarring at DxNo
Age
Initial
Yes
F/U
Initial
F/U
<1
Proph Abx
III-V: Surgery
Proph Abx
III-V: Surgery
1-5
Proph Abx
B/L grade V:
Surgery
III-V: Surgery
V: Surgery
III-V: Surgery
6-10
Proph Abx
III-IV: Surgery Proph Abx
III-IV: Surgery
B/L grade III-IV or
B/L grade III-IV
U/L V: Surgery
or U/L V: Surgery
(AUA, Report on The Management of Primary VUR in Children, Journal of Urology,
May, 1997.)
8. Management of VUR
Scarring at DxNo
Age
Initial
Yes
F/U
Initial
F/U
<1
Proph Abx
III-V: Surgery
Proph Abx
III-V: Surgery
1-5
Proph Abx
B/L grade V:
Surgery
III-V: Surgery
V: Surgery
III-V: Surgery
6-10
Proph Abx
III-IV: Surgery Proph Abx
III-IV: Surgery
B/L grade III-IV or
B/L grade III-IV
U/L V: Surgery
or U/L V: Surgery
“The recommendations, which generally lack empirical scientific
support, reflect the clinical experience and opinion of the panel.”
(AUA, Report on The Management of Primary VUR in Children, Journal of Urology,
May, 1997.)
9. Current Conceptual Model
Figure 3. Conceptual ModelProphylactic
antibiotics prevent
recurrent UTI
End Stage Renal
Disease
UTI(s)
RENAL
SCARRING
Hypertension
Surgery
corrects VUR
Pre-eclampsia
VUR
10. What is the evidence to support current model of diagnosing and treating VUR in children after UTI?
11. Ecological Evidence
• Analyses of dialysis and transplantregistries
• Expect reduction in incidence of end
stage renal disease attributable to reflux
nephropathy following the diagnosis and
treatment of VUR started in the 1960’s
• Not there
Broyer M, Chantler C, Donckerwolcke R, Ehrich JH, Rizzoni G, Scharer K. The
paediatric registry of the European Dialysis and Transplant Association: 20 years'
experience. Pediatr Nephrol. Dec 1993;7(6):758-768.
Fenton S, Desmeules M, Copleston P, et al. Renal replacement therapy in Canada: a
report from the Canadian Organ Replacement Register. Am J Kidney Dis. Jan
1995;25(1):134-150.
12. Observational Studies
Conway, P. H. et al. JAMA 2007;298:179-186.13. Incidence Rates and Follow-up
• Incidence Rate of First UTI: 0.007/person-year– Similar to previous estimates
• Incidence Rate of Recurrent UTI after first UTI:
0.12/person-year
– Significantly lower than previous estimates of 2148% recurrence with follow-up of 6-12 months
• Mean observation time was 408 days with a
median of 310 days (IQR 150 – 584 days),
range of 24 - 1600 days
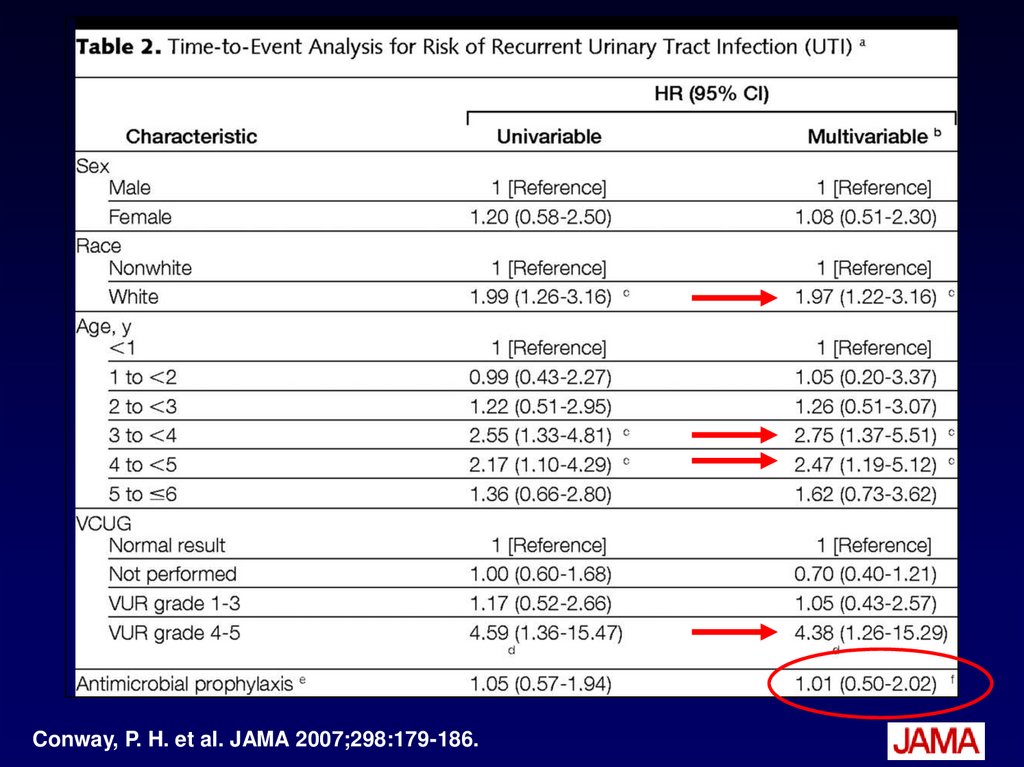
14.
15.
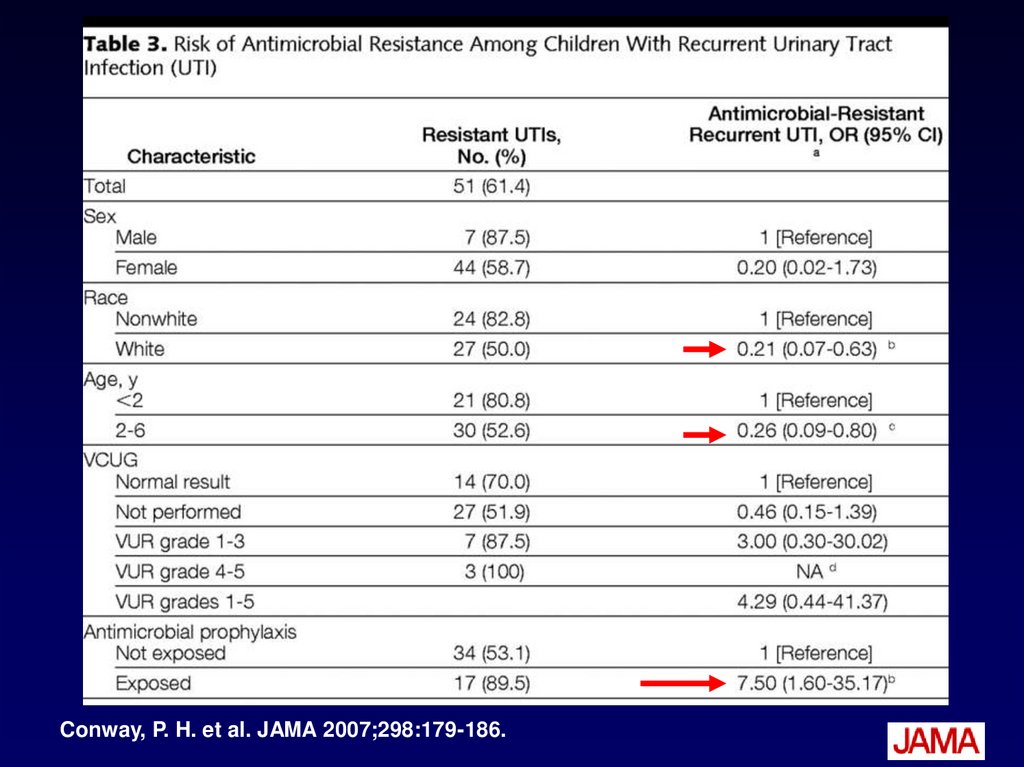
Conway, P. H. et al. JAMA 2007;298:179-186.16.
Conway, P. H. et al. JAMA 2007;298:179-186.17.
Conway, P. H. et al. JAMA 2007;298:179-186.18.
Conway, P. H. et al. JAMA 2007;298:179-186.19. Survival Analysis
• Outcome is time to an event (e.g. death,recurrent infection)
• Observation time varies from one
subject to another
– Different quantity
– Different start and stop times
• Censoring
20. Types of censoring
• Subject does notexperience event of
interest
• Incomplete follow-up
– Lost to follow-up
– Withdraws from
study
– Dies
21. Hazard Ratio
• The hazard ratio in survival analysis isthe effect of an explanatory variable on
the hazard or risk of an event.
• Consider hazard ratio to be an
estimate of relative risk
22. Clinical Trials
No. (%) with Recurrent UTIAuthor, Journal, Year
Savage, Lancet, 1975
Abx
7/29 (24%)
No Abx
RR (95% CI)
4/32 (13%)
1.9 (0.6-5.9)
Garin, Pediatrics, 2006 13/55 (24%) 12/58 (21%) 1.1 (0.6-2.3)
Roussey, JU, 2008
18/103 (17%) 32/122 (26%) 0.7 (0.4-1.1)
Garin: Up to age 18 years, febrile UTI, grades 1-3 VUR, unblinded
Roussey: 1 mo – 3 years, febrile UTI, grades 1-3 VUR, unblinded
In Garin study, recurrent acute pyelo seen in 7/55 (abx) v. 1/58 (placebo)
(p=0.03) raising specter of INCREASED risk of APN with prophylactic antibiotics.
23. Systematic Review
“The evidence to support the widespreaduse of antibiotics to prevent recurrent
symptomatic UTI is weak. Large
randomized, double blinded studies are
needed…”
Williams et al, Long-term antibiotics for preventing recurrent UTIs in children.
Cochrane Database of Systematic Reviews 2006, Issue 3.
24. What’s a pediatrician/parent to do?
25. Maintain Status Quo
• Absence of evidence is not evidence ofabsence of benefit
• Continue to screen all children for VUR
after first UTI
• Continue antibiotic prophylaxis for
children with VUR until VUR resolves
• Conservative, one size fits all approach
26. Individualize Care
• 3 y.o. girl with first afebrile UTIconcurrent with potty training vs…
• 5 mo. girl with febrile UTI requiring
hospitalization; history of other febrile
illnesses that got better with antibiotics;
mother with duplicated collecting
system and h/o bilateral grade 4 VUR
that never completely resolved.
27. Consider Dysfunctional Elimination
• Abnormal elimination pattern(frequent/infrequent voids, urgency,
constipation)
• Bladder/bowel incontinence
• Withholding maneuvers
• Underdiagnosed and undertreated
• 40% 1st UTI; 80% recurrent UTI
• Treatment decreases UTI recurrence and
speeds resolution of VUR
28. Dysfunctional Elimination Treatment
• Scheduled voids q 2-3 hours• Treat constipation
– Laxatives
– Increase fluid intake
• Avoid bladder irritants
– Caffeine, food coloring, chocolate, citrus, carbonation
• Urology referral
– Further evaluation
– Biofeedback for pelvic floor muscle training
– Anticholinergics
29. “Top Down” Imaging Approach
• You don’t need VUR to develop kidneyscars after UTI
• If you have a normal DMSA scan with a
febrile UTI, you are VERY unlikely to
have high grade (>3/5) VUR
30. APN
DMSA Renal ScansNormal
APN
Renal Scarring
31. Renal Scarring on DMSA
VURNo VUR
45%
40%
35%
30%
25%
20%
15%
10%
5%
0%
Rushton
1992
Jakobsson
1994
Hoberman
2003
Garin
2006
32. Dilating VUR (Grades 3-5)
Normal DMSAAbnormal DMSA
25%
20%
15%
10%
5%
0%
Tseng 2007
Preda 2007
Normal
DMSA
Abnormal
DMSA
No VUR
133
105
16
VUR 1-2
7
18
21
VUR 3-5
1
26
Normal
DMSA
Abnormal
DMSA
No VUR
36
64
VUR 1-2
5
VUR 3-5
0
33. “Top Down” Approach
• Perform DMSA within 30 days of UTI• Normal: reassure parents that kidneys
are normal and child unlikely to have
dilating VUR skip the VCUG
• Abnormal: obtain VCUG, consider
antibiotics v. surgery if VUR present,
repeat DMSA in 4-6 months to diagnose
scars
34. “Top Down” Approach
• Spares a lot of children a VCUG (48%in Preda study)
• DMSA less than half the radiation of a
VCUG
• DMSA less invasive than a VCUG
• DMSA gives information about the
health of the kidneys, which can be
followed over time.
35. No Work-up
• Defer work-up until 2nd or 3rd UTI• Heightened vigilance
–
–
–
–
Educate on early signs and symptoms
Emphasize need for rapid diagnosis
Treat dysfunctional elimination
?Provide urine collection kits and dip sticks
• Likely that early diagnosis and treatment will
prevent most UTI-related scarring.
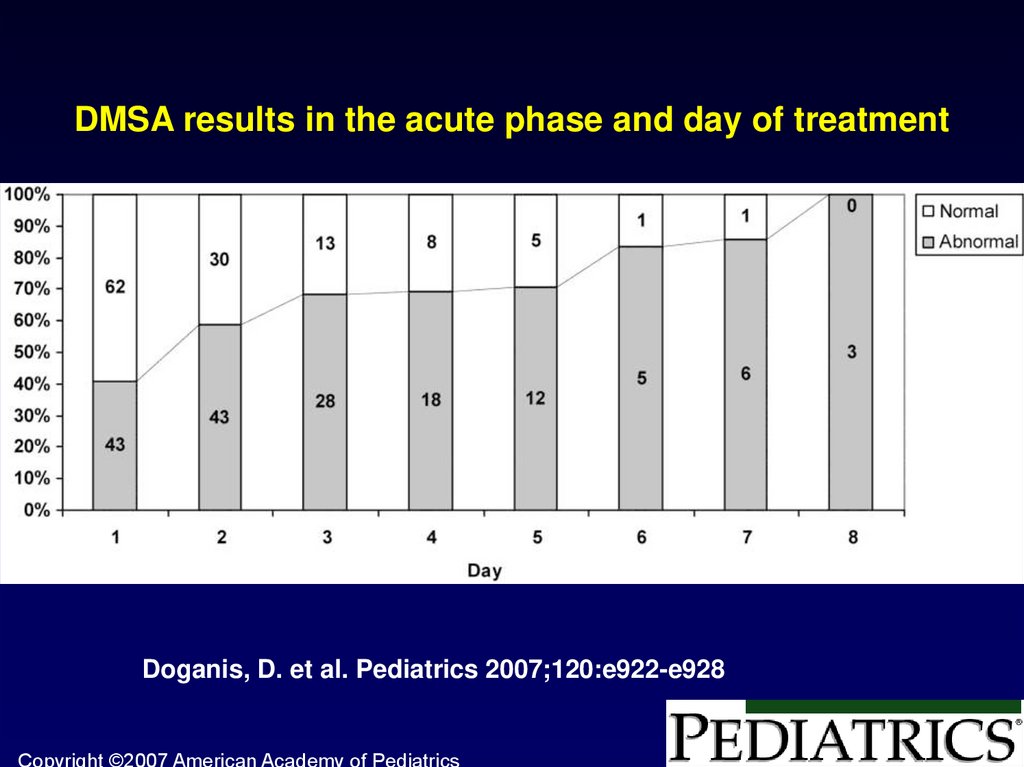
36.
DMSA results in the acute phase and day of treatmentDoganis, D. et al. Pediatrics 2007;120:e922-e928
Copyright ©2007 American Academy of Pediatrics
37. Refer to RIVUR study
• Randomized Intervention for Childrenwith VesicoUreteral Reflux
• CMH KC Site PI: Dr. Uri Alon
38. Study Design
• NIDDK funded (U01 contract)• Multi-center
– 15 Clinical Trial Centers across the US
– Data Coordinating Center at UNC Chapel Hill
• Randomized Placebo Controlled Trial
• Initial UTI, presence of grades I-IV VUR
• Effect of prophylactic TMP/SMZ on:
– Recurrent UTI
– Renal scarring
– Antimicrobial resistance
39. Inclusion Criteria
• 2 months – 6 years at time ofrandomization
• Diagnosed 1st or 2nd F/SUTI within 16
weeks prior to randomization
• Presence of Grade I- IV VUR on VCUG
40. Time Line
Recruitment started July 2007
2 years of recruitment
2 years of follow-up
Plan to recruit 600 patients
41. Endpoints
• Primary– Recurrence of F/SUTI
• Secondary
– Time to first recurrence of F/SUTI
– Renal scars on DMSA scan
– Stool E. coli resistant to TMP/SMZ
– Recurrent F/SUTI caused by TMP/SMZ
resistant organisms
42. Modified Conceptual Model
Delayed UTIdiagnosis and
treatment
UTI(s)
UTI (s)
Prompt diagnosis and
treatment of UTI
Prophylactic antibiotics
prevent recurrent UTI
Renal
Scarring
End Stage Renal
Disease
Hypertension
VUR
Congenital
VUR and renal
dysplasia
Pre -eclampsia
VUR
43. Questions
44. International Classification of VUR
45. Renal Ultrasound
46. Deflux
47. Endoscopic Correction of VUR
• Deflux procedure– Endoscopic injection of bulking agent
(Dextranomer/hyaluronic acid) into submucosal
layer of bladder just beneath or within the ureteric
orifice.
– “Minimally invasive” compared with open surgery
– Day surgery
– Requires sedation
48. Deflux: Capozza
• >1 y.o• Grades II-IV VUR persistent for at least 6
months
• Randomly assigned (2:1) to:
– Dextranomer/Hyaluronic Acid (n = 40)
– Prophylactic abx (n = 21)
• 12 months later 69% v. 38% (p=0.03) had
bilateral grade I or less VUR.
• 11 (25%) needed 2nd injection at month 3,
only 2 successful
Capozza, N, Dextranomer/hyaluronic acid copolymer implantation for VUR: a randomized
comparison with antibiotic prophylaxis, J Pediatr, 2002 Feb; 140(2):230-4.
49. Deflux: Capozza
Recurrent UTIDeflux
Proph abx
p-value
6/40 (15%)
0/21 (0%)
0.08
New renal
3/80 (4%)
1/42 (2%) 0.6
scars*
Renal scars
11/80 (14%) 7/42 (16%) 0.4
healed*
Parenchymal
1/40 (3%)
3/21 (14%) 0.11
kidney damage*
*As determined by renal US, not DMSA.
50. PIC VUR
PatientsRenal Units
Recurrent
febrile UTIs/
No VUR on
conventional
VCUG
30/30
48/60
No febrile
UTIs/ No VUR
on
conventional
VCUG
0/15
Recurrent
febrile UTIs/
VUR on
conventional
VCUG
12/12
(all 48 ureteral
orifices lateral
and/or patulous)
0/30
(all 30 ureteral
orifices normal
appearing)
20/24
(all 20 ureteral
orifices lateral
and/or patulous)
Interpretation
“Explains”
recurrent UTIs
Doesn’t show
VUR in kids
with no h/o UTI
Shows VUR in
kids with h/o
UTI
51. PIC VUR
• Invasive – Requires general anesthesia andinstrumentation of bladder
• Specificity needs confirmation – 0/15 does
not mean no false positives
• % children with febrile UTI found to have PIC
VUR after negative VCUG fell to 82% in small
prospective validation study (Edmonson,
Urol, 2006)
• No evidence that treating those found to have
PIC VUR prevents recurrent UTI or renal
scarring.
52. International Reflux Study
53. Effectiveness of Interventions for VUR
Open surgical correction of VUR plus prophylacticantibiotics v. prophylactic antibiotics alone to prevent
recurrent UTIs
Author, Journal, Year
RR recurrent UTI RR recurrent UTI
2 years
5 years
Wheeler, ADC, 2003
(meta-analysis)
1.1 (0.6-2.1)
0.99 (0.8-1.3)
54. Effectiveness of Interventions for VUR
Open surgical correction of VUR plus prophylacticantibiotics v. prophylactic antibiotics alone to prevent
renal scarring
Author, Journal, Year
Wheeler, ADC, 2003
(meta-analysis)
RR new renal
scars (2 years)
1.1 (0.3-3.4)
RR new renal
scars (5 years)
1.1 (0.8-1.5)
“It is not clear whether any intervention for children with primary VUR
does more good than harm. Well designed and adequately powered
placebo controlled randomized trials of antibiotics alone in children with
VUR are now required.” (Wheeler et al, Antibiotics and surgery for VUR:
a meta-analysis of RCTs, ADC, 2003)
55. RIVUR Study
56. Definitions
Appropriately treated UTIAntibiotic therapy continues for a minimum of 7
days AND:
1) There is documented sensitivity of the
organism to the antibiotic used for treatment
OR
2) There is a documented test of cure
(negative urine culture) 1-14 days after
initiation of therapy.
57.
Screening PhaseFebrile or Symptomatic
UTI
Check Preliminary Eligibility Criteria
Complete Study Screening / Baseline Imaging
US
(within 6 weeks of
index UTI)
RANDOMIZATION VISIT
Treatment Phase
1.
2.
3.
4.
5.
Confirm Eligibility
Treatment Phase Consent
Randomize
Baseline Data Collection
Specimen Collection
VCUG
(within 6 weeks of
index UTI)
DMSA
(If VUR; within 8 weeks of
index UTI)
Scheduled Follow-up Contacts
Calls
(Every 2
months)
Routine Visits
6, 12, 18 months
Specimen
Collection
UTI Evaluation Visits
(unscheduled visits)
END OF STUDY - EXIT EXAM
24 months
1. Scheduled Data Collection
2. Specimen Collection
3. VCUG
4. DMSA
58. Definitions
UTI• Pyuria on urinalysis
–
–
–
>10 WBC/mm3 (uncentrifuged specimen) OR
>5 WBC/hpf (centrifuged specimen), OR
>1+ leukocyte esterase on dipstick
• Culture proven infection with a single
organism
– >5 x 104 CFU/mL (catheterized or suprapubic aspiration
urine specimen) OR
–
>105 CFU/mL (clean voided specimen).
59. Definitions
Fever• Documented temperature of at least 100.4 °F
(38 °C), measured anywhere on the body
either at home or at doctor’s office
Symptoms
• Suprapubic, abdominal, or flank pain or
tenderness
• Urinary urgency, frequency, hesitancy, or
dysuria, or foul smelling urine
• In infants < 4 months old: failure to thrive,
dehydration, or hypothermia
60. Endpoints
Treatment Failures• Occurrence of 2 recurrent FUTIs within
the study period, OR
• Total of 4 recurrent F/SUTIs within the
study period
• Additional renal segment involvement at
12 mo. DMSA scan
61.
Study MonthType of Contact
Informed Consent
DMSA
Contrast VCUG
Medical History and Physical
Examination
Questionnaires
Dysf Void Symp Score,
PACCT (age>3),
QOL assessment
Parent Questionnaire
Randomization
Study medication
dispensation
Study medication
Accountability
Urine tests
Urinalysis, Culture**,
Microalbumin/Creatinine,
Urine for central
Repository
Blood tests
CBC with diff;
Creatinine, lytes, SGOT,
SGPT; Cystatin ; Blood for
central Repository
Rectal Swabs
Telephone Follow-up
0
(Visit)
Randomization/
Baseline
6 month
(Visit)
Follow-up
X
X*
12 month
(Visit)
Follow-up
18 month
24 month
(Visit)
(Exit Visit)
Follow-up Follow-up
X
Every 2
months
(Phone)
Follow-up
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
62. Renal Scarring
Author, Journal, YearVUR
No VUR
RR (95% CI)
Rushton, J Urol, 1992
40%
43%
0.9 (0.4-2)
Jakobsson, ADC, 1994
42%
19%
2.2 (1.3-3.8)
Hoberman, NEJM, 2003
15%
6%
2.4 (1.1-5.2)
Garin, Pediatrics, 2006
6%
6%
1.1 (0.4-3.1)
63. Renal Scarring Less Common
Author, Journal, YearN
# (%)
F/U
Rushton, J Urol, 1992
33
16 (48) 11 mo (mean)
Jakobsson, ADC, 1994
Stokland, J Peds, 1996
Hoberman, NEJM, 2003
76
157
275
28 (37)
59 (38)
26 (9)
2 years
1 year
6 mo
Garin, Pediatrics, 2006
118
6 (5)
1 year
Decreasing rates of renal scarring possibly due to
increased awareness and earlier Dx and Rx of UTIs in
febrile infants?
64. Potential Harms and Costs
• VCUG and RNC are invasive and cause physicaldiscomfort and psychological distress.
• VCUG involves exposure to ionizing radiation.
• Diagnosis of VUR and perceived risk of renal scarring
causes anxiety to patient and family.
• Prophylactic antibiotics contribute to antimicrobial
resistance in the patient and the community.
– Recurrent UTIs with bacteria resistant to Cefotaxime = 27%
in children receiving prophylactic antibiotics v. 3% in children
not receiving them (RR=9.9; 95% CI [4-24.5]). (Lutter et al.,
Antibiotic resistance patterns in children hospitalized for UTIs, APAM, 2006)
• Costs of diagnosis and treatment potentially great.