

 biology
biologySimilar presentations:

")




 Thromboxanes Leukotrienes Related Compounds")
")
")

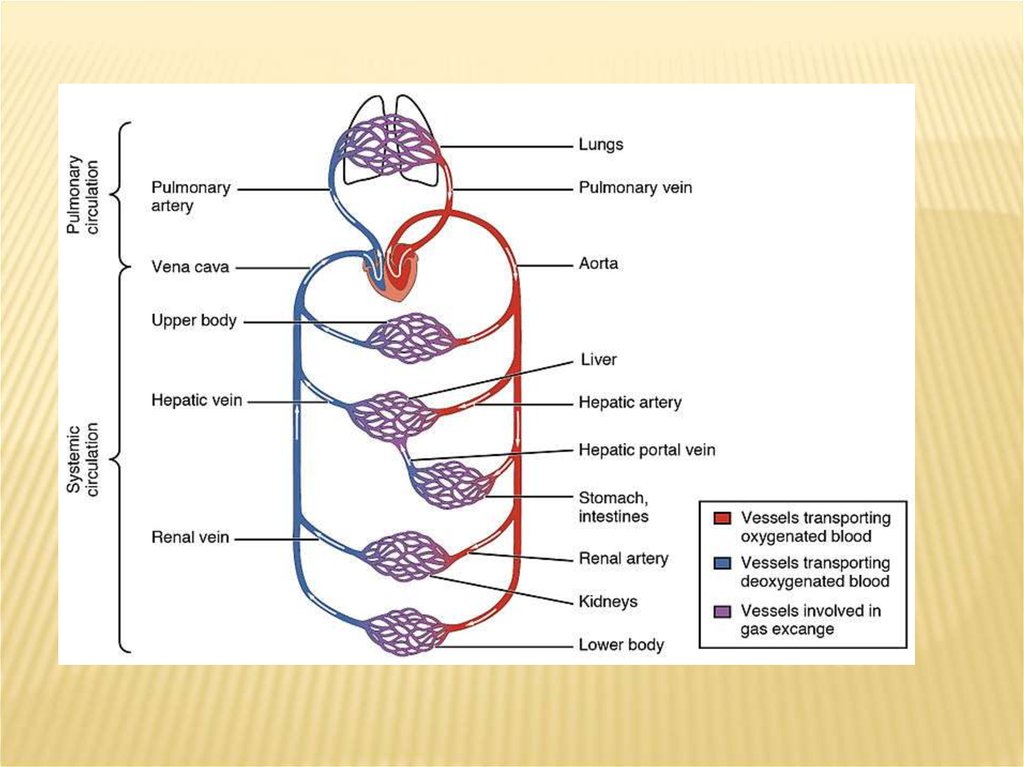
Immunophysiology of cardiovascular system
1. Immunophysiology of cardiovascular system
IMMUNOPHYSIOLOGY OFCARDIOVASCULAR SYSTEM
2.
3.
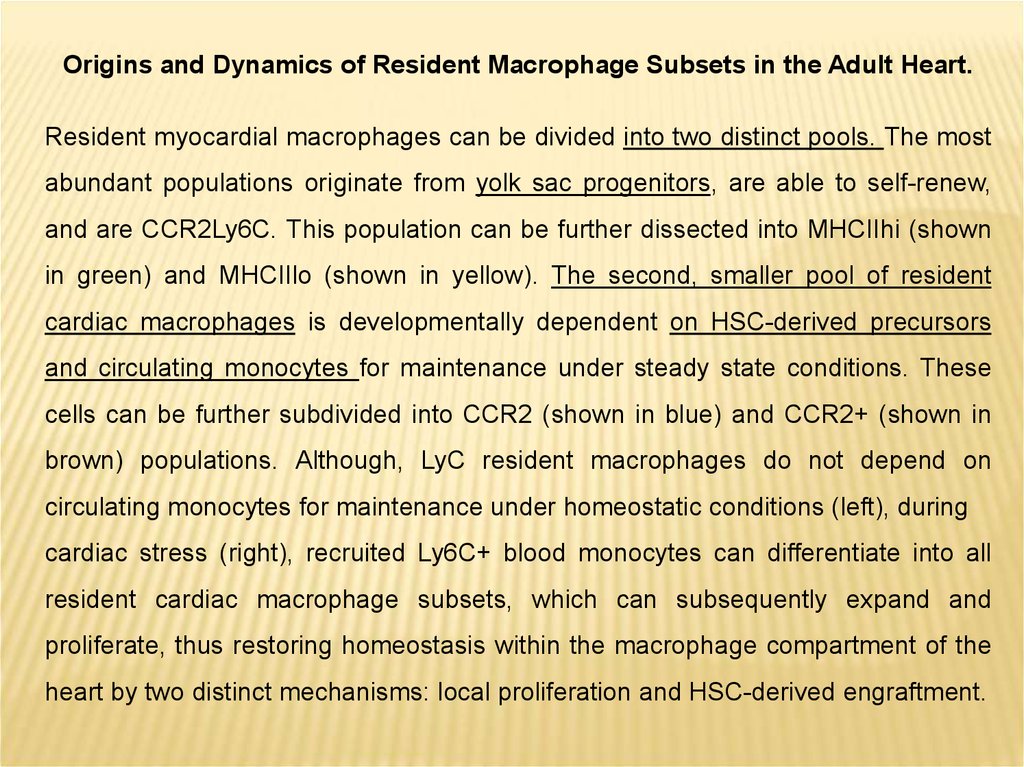
Origins and Dynamics of Resident Macrophage Subsets in the Adult Heart.Resident myocardial macrophages can be divided into two distinct pools. The most
abundant populations originate from yolk sac progenitors, are able to self-renew,
and are CCR2Ly6C. This population can be further dissected into MHCIIhi (shown
in green) and MHCIIlo (shown in yellow). The second, smaller pool of resident
cardiac macrophages is developmentally dependent on HSC-derived precursors
and circulating monocytes for maintenance under steady state conditions. These
cells can be further subdivided into CCR2 (shown in blue) and CCR2+ (shown in
brown) populations. Although, LyC resident macrophages do not depend on
circulating monocytes for maintenance under homeostatic conditions (left), during
cardiac stress (right), recruited Ly6C+ blood monocytes can differentiate into all
resident cardiac macrophage subsets, which can subsequently expand and
proliferate, thus restoring homeostasis within the macrophage compartment of the
heart by two distinct mechanisms: local proliferation and HSC-derived engraftment.
4.
5.
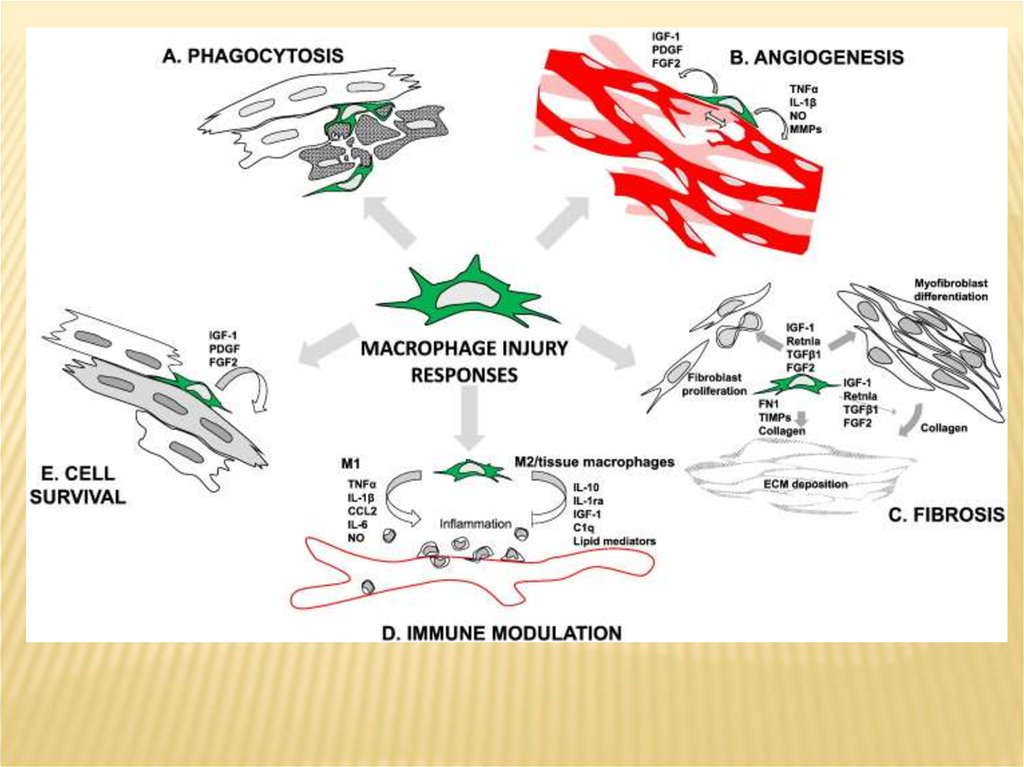
Diverse role of macrophages in injury resolution.(A) Macrophage mediated removal of cellular and tissue debris by phagocytosis.
(B) Angiogenesis mediated by macrophage paracrine factors and direct interaction of
macrophage with endothelial tip cells.
(C) Induction of tissue fibrosis by various paracrine factors. Macrophage-derived
factors can induce fibroblast proliferation and myofibroblast differentiation, and can
directly and indirectly contribute to extracellular matrix (ECM) deposition.
(D) Macrophage subtypes (‘M1’ and ‘M2’) can promote and suppress inflammation,
respectively by enhancing or inhibiting leukocyte infiltration and secretion of
inflammatory mediators by local cells.
(E) Various macrophage-derived factors can promote cell survival.
While M2 macrophages may be the principal drivers of angiogenesis associated
with injury resolution, M1 macrophages are highly fibrolytic, which may facilitate
angiogenesis, and secrete pro-angiogenic factors such as TNFα and IL-1β, and nitric
oxide. Therefore, both injury-associated macrophage subsets may contribute to
blood vessel growth, which is critical for the minimization of cell death due to
hypoxia.
6.
7.
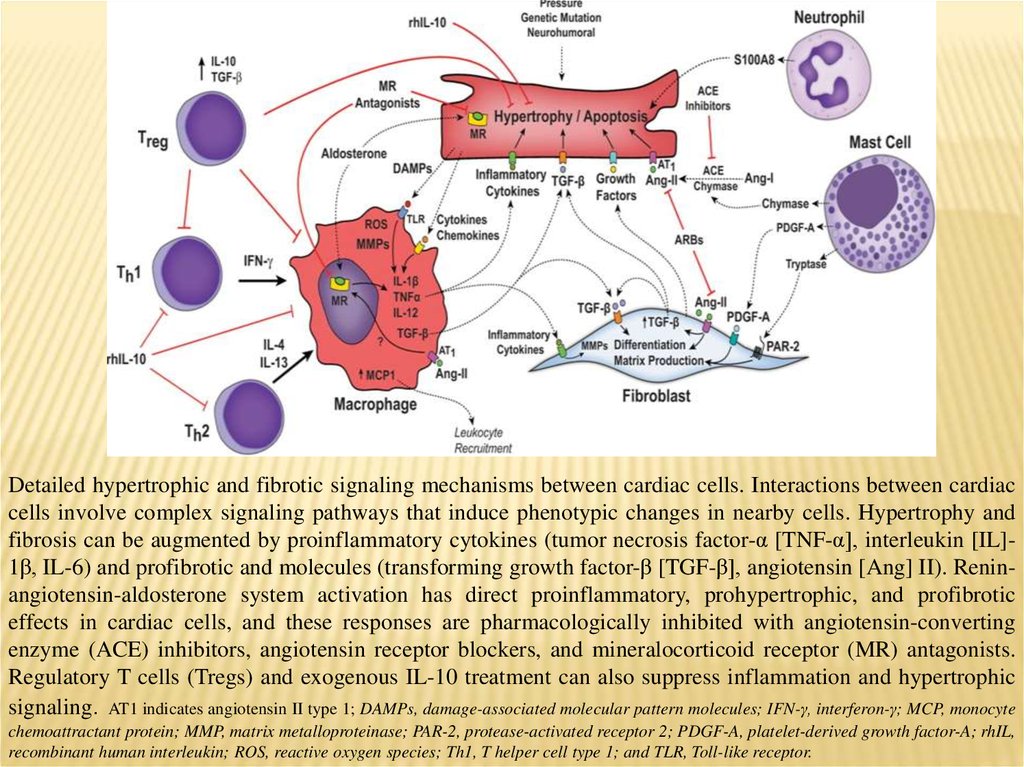
Detailed hypertrophic and fibrotic signaling mechanisms between cardiac cells. Interactions between cardiaccells involve complex signaling pathways that induce phenotypic changes in nearby cells. Hypertrophy and
fibrosis can be augmented by proinflammatory cytokines (tumor necrosis factor-α [TNF-α], interleukin [IL]1β, IL-6) and profibrotic and molecules (transforming growth factor-β [TGF-β], angiotensin [Ang] II). Reninangiotensin-aldosterone system activation has direct proinflammatory, prohypertrophic, and profibrotic
effects in cardiac cells, and these responses are pharmacologically inhibited with angiotensin-converting
enzyme (ACE) inhibitors, angiotensin receptor blockers, and mineralocorticoid receptor (MR) antagonists.
Regulatory T cells (Tregs) and exogenous IL-10 treatment can also suppress inflammation and hypertrophic
signaling. AT1 indicates angiotensin II type 1; DAMPs, damage-associated molecular pattern molecules; IFN-γ, interferon-γ; MCP, monocyte
chemoattractant protein; MMP, matrix metalloproteinase; PAR-2, protease-activated receptor 2; PDGF-A, platelet-derived growth factor-A; rhIL,
recombinant human interleukin; ROS, reactive oxygen species; Th1, T helper cell type 1; and TLR, Toll-like receptor.
8.
Macrophages play an important role in regulating new blood vessel and lymphatic vesselgrowth in many species. Macrophages play an essential role in many injury contexts by
supporting angiogenesis through expression of Vascular endothleial growth factor A.
Macrophage depletion prior to cardiac cryo-injury results in impaired cardiac function
and poor survival. Normal regeneration activates myofibroblast conversion in the epicardium
but the depletion of macrophages results in fibroblast activation not normally found within the
lesioned site. This observation gives weight to the notion that wound macrophages act as a
negative regulator of fibroblast differentiation. Macrophage depletion results in disruption of
the regeneration program by induction of fibroblast activation. Dynamic regulatory feedback
mechanisms between mesenchymal and macrophage cell types are now appreciated to be
important for regulating inflammation and fibrotic activation.
9.
Recent research findings suggest thatmacrophages contribute to tissue
regeneration and may play a role in the activation and mobilisation of stem
cells. A key mechanism whereby macrophages may affect tissue repair and
regeneration is by instructing the stem cell niche by paracrine mechanisms.
Macrophages likewise positively regulate mesenchymal stem cells (MSC). In vitro
experiments on cultured human MSCs demonstrate that macrophage-derived
growth factors enhance MSC growth, viability, motility and secretion of paracrine
factors. However, macrophage-MSC interactions are not uni-directional. MSCs
transplanted to the injured myocardium induce a shift in the balance of
macrophages to an M2-like phenotype Taken together, these examples
underscore the importance of macrophage-stem cell cross talk for stem cell
homeostasis and mobilisation. Considering the close interaction of cTMs with the
epicardium, these observations indicate that cTMs may be important for epicardial
progenitor cell homeostasis and potential maintenance of the progenitor cell
phenotype.
10.
11.
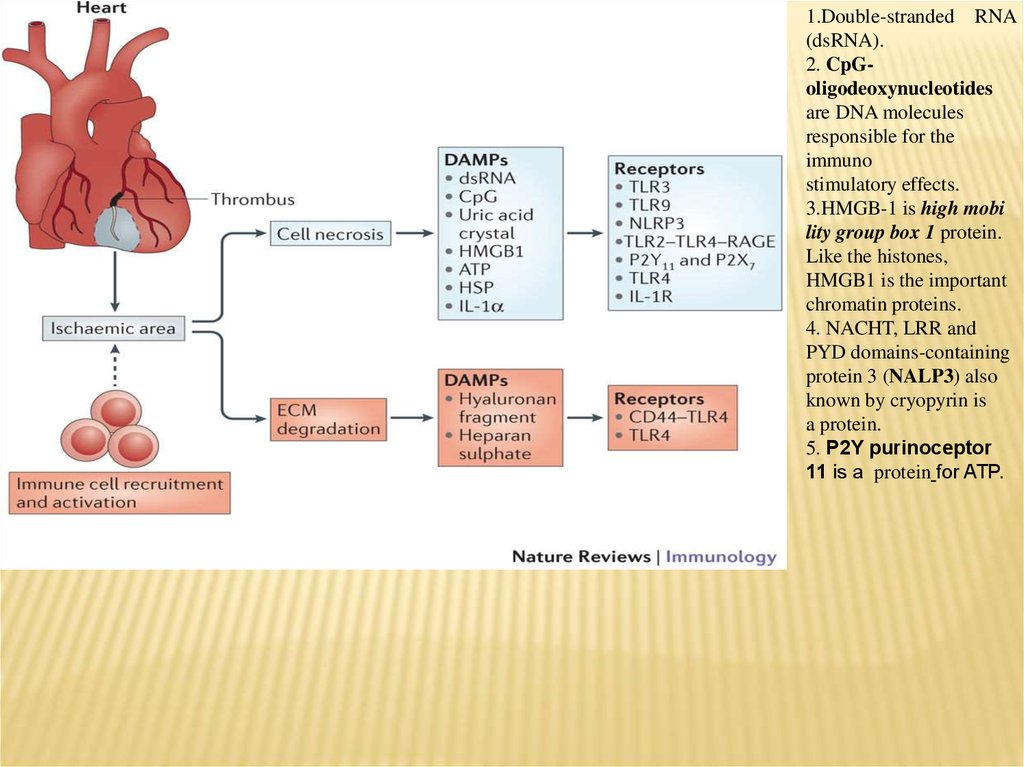
1.Double-stranded RNA(dsRNA).
2. CpGoligodeoxynucleotides
are DNA molecules
responsible for the
immuno
stimulatory effects.
3.HMGB-1 is high mobi
lity group box 1 protein.
Like the histones,
HMGB1 is the important
chromatin proteins.
4. NACHT, LRR and
PYD domains-containing
protein 3 (NALP3) also
known by cryopyrin is
a protein.
5. P2Y purinoceptor
11 is a protein for ATP.
12.
13.
14.
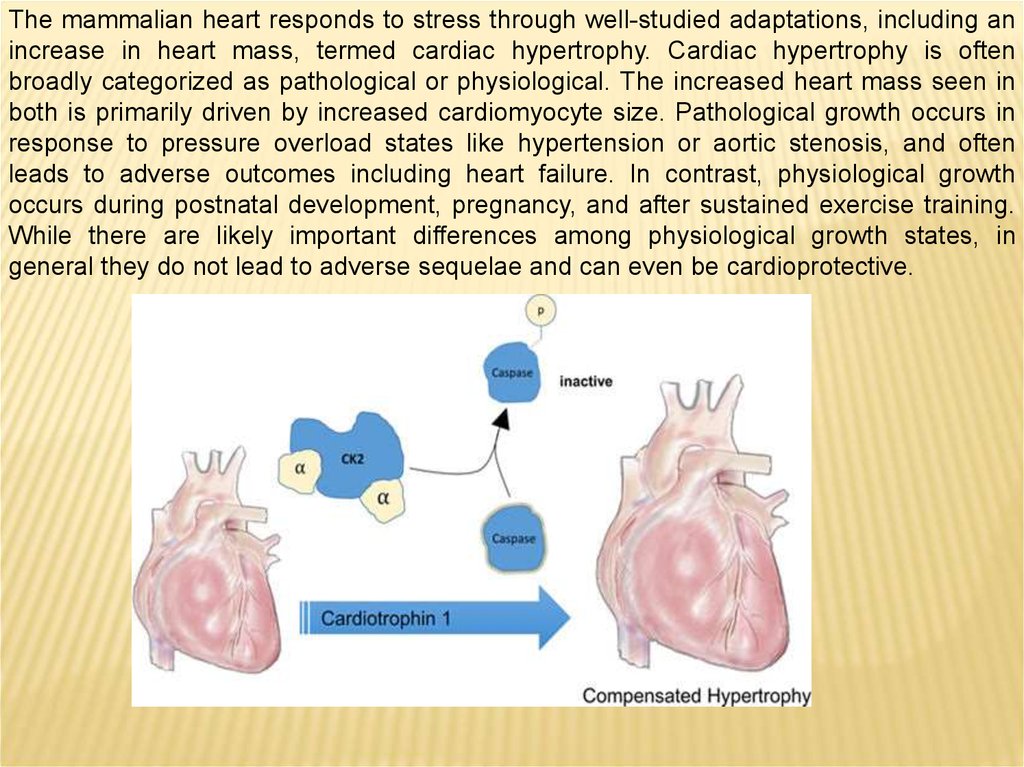
The mammalian heart responds to stress through well-studied adaptations, including anincrease in heart mass, termed cardiac hypertrophy. Cardiac hypertrophy is often
broadly categorized as pathological or physiological. The increased heart mass seen in
both is primarily driven by increased cardiomyocyte size. Pathological growth occurs in
response to pressure overload states like hypertension or aortic stenosis, and often
leads to adverse outcomes including heart failure. In contrast, physiological growth
occurs during postnatal development, pregnancy, and after sustained exercise training.
While there are likely important differences among physiological growth states, in
general they do not lead to adverse sequelae and can even be cardioprotective.
15.
Cardiotrophin-1 (CT1) is a cytokine in the interleukin-6 family and is known to inducecardiac hypertrophy. Initially, CT1 was thought to drive pathological hypertrophy but was
found to promote cell survival and induce proliferation of embryonic cardiomyocytes. In a
recent paper in Cell Research, Abdul-Ghani et al. (2017) show that CT1 causes a
reversible, protective form of cardiomyocyte hypertrophy.
Cardiotrophin 1 (CT-1) stimulates the production of interleukin 6 (IL-6). This suggests
that at least in some pathological situations CT-1 might represent an
immunomodulator regulating cytokine-induced gene products.
16.
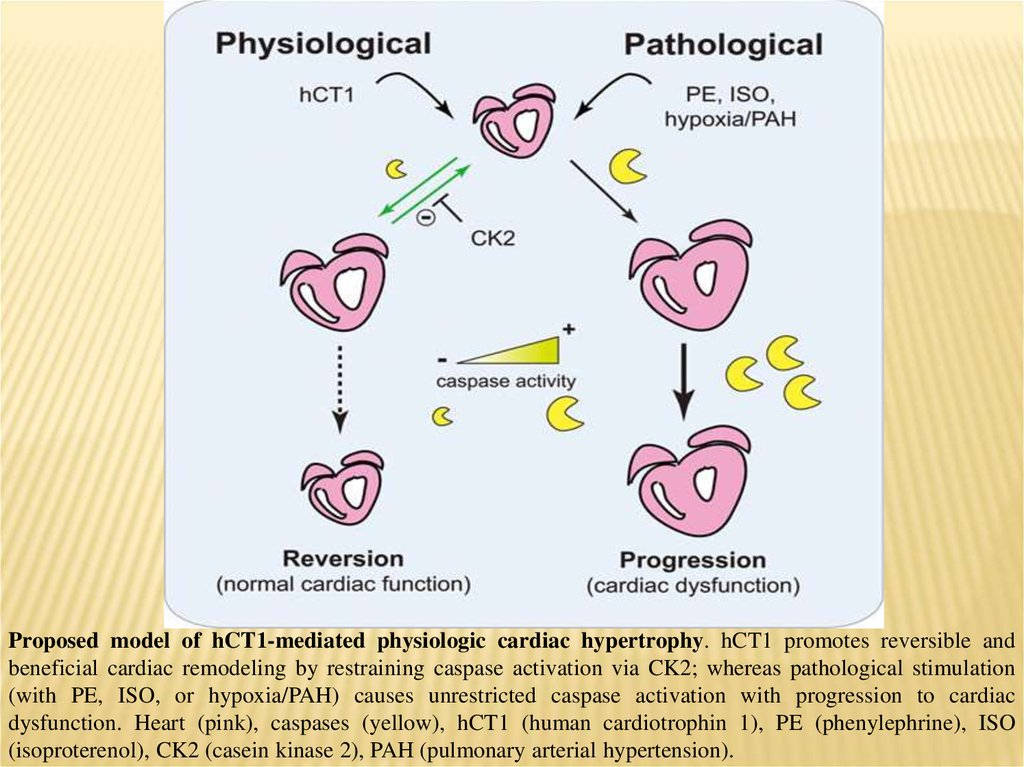
Proposed model of hCT1-mediated physiologic cardiac hypertrophy. hCT1 promotes reversible andbeneficial cardiac remodeling by restraining caspase activation via CK2; whereas pathological stimulation
(with PE, ISO, or hypoxia/PAH) causes unrestricted caspase activation with progression to cardiac
dysfunction. Heart (pink), caspases (yellow), hCT1 (human cardiotrophin 1), PE (phenylephrine), ISO
(isoproterenol), CK2 (casein kinase 2), PAH (pulmonary arterial hypertension).
17.
Interestingly, cardiomyocytes themselves can phagocytose latex particles invitro and potentially cardiomyocyte debris in vivo, the latter of which may have
an important role in the developing heart. Recently, myofibroblasts were
identified as another non-professional phagocyte that were capable of engulfing apoptotic cardiomyocytes. While the presence of professional cardiac
phagocytes, such as macrophages, minimalizes the necessity for nonprofessional phagocytes, such as myofibroblasts, to phagocytose a dying
neighbor, the contribution of non-professional phagocytes to the clearance of
apoptotic and necrotic debris is underexplored and whether these cells
cooperate with macrophages in the heart to promote cardiac repair requires
additional study.